
Abstract
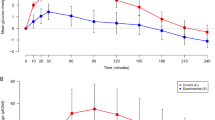
A comparison was made between isocaloric amounts of 24% glucose and 24% Triofusin® (composed of 120 g fructose, 60 g glucose and 60 g xylitol per liter) during the course of a 6-day, 3-phase crossover study of 15 patients undergoing total parenteral nutrition. The patients received a total of 0.5 g carbohydrate per kilogram body weight per hour and 6 g carbohydrate per kg per day. Plasma glucose was significantly higher during glucose infusion (7–22 mmol/l, median: 9 mmol/l) than during Triofusin® infusion (5–16 mmol/l, median: 6 mmol/l). A moderate to severe glucosuria was detected in three patients during infusion of 24% glucose, and this declined considerably during the Triofusin® period. The total renal carbohydrate loss during the glucose period was 0–143 g, median: 6 g per day, and during the Triofusin® period was 6–68 g, median: 10 g per day. The nitrogen balance and carbamide production rate were the same in the two infusion regimes. Changes in biochemical liver parameters were observed in most of the patients, but these could not be attributed to parenteral nutrition. None of the patients developed symptoms of metabolic acidosis. There was a slightly but significantly higher urinary excretion of oxalate in the Triofusin® period (0.1–1.1 mmol per day, median: 0.5 mmol per day) than in the glucose period (0.1–1.0 mmol per day, median: 0.4 mmol per day). Most of the patients exhibited a slightly increased urinary excretion of urate, irrespective of the infusion regimen. Serum urate remained normal. It was concluded that Triofusin® infused in the described dosage is a suitable calorie source for parenteral nutrition, but that it does not present a distinct advantage over the use of pure glucose solution. In patients suffering from reduced glucose tolerance, however, Triofusin® represents a more easily manageable calorie source.
Similar content being viewed by others

References
Ahnefeld FW, Bässler KH, Bauer BL, Berg G, Bergmann H, Bessert I, Dick W, Dietze G, Dölp R, Dudziak R, Förster H, Geser CA, Grunst J, Halmagyi M, Heidland A, Heller L, Horatz K, Kuhlmann H, Kult J, Lutz H, Matzkies F, Mehnert H, Milewski P, Paulini K, Pesch HJ, Peter K, Rittmeyer P (1975) Suitability of non-glucose-carbohydrates for parenteral nutrition. Eur J Intensive Care Medicine 1:105
Archer HE, Dormer AE, Scowen EF, Watts RWE (1957) Studies on the urinary excretion of oxalate by normal subjects. Clin Sci 16:405
Bässler KH (1974) Xylit. In: Bergmayer HU (ed) Methoden der enzymatischen Analyse, 3. Auflage, Band II. Verlag Chemie, Weinheim p 1425
Berg G, Matzkies F, Bickel H (1974) Dosierungsgrenzen bei der Infusion von Glucose, Sorbit, Fructose, Xylit und deren Mischungen. Dtsch Med Wochenschr 99:633
Bergmayer HU, Bernt E, Schmidt F, Stork H (1974) D-Glucose. In: Bergmayer HU (ed) Methoden der enzymatischen Analyse, 3. Auflage, Band II. Verlag Chemie, Weinheim, p 1241
Bernt E, Bergmayer HU (1974) D-Fructose. In: Bergmayer HU (ed) Methoden der enzymatischen Analyse, 3. Auflage, Band II. Verlag Chemie, Weinheim, p 1349
Bickel H, Schwemmle K, Scranowitz P, Wopfner F (1975) Glucose, Fructose und Xylit als Energieträger in der postoperativen parenteralen Ernährung. Dtsch Med Wochenschr 100:527
Calloway DH, Odell ACF, Margen SJ (1971) Sweat and miscellaneous nitrogen losses in human balance studies. J Nutr 101:775
Dudrick SJ, Long JM (1977) Applications and hazards of intravenous hyperalimentation. Ann Rev Med 28:517
Faber M (1959) Nitrogen determination by Kjeldahl's method (Danish). In: Astrup P, Brøckner-Mortensen K, Faber M. Klinisk laboratorieteknik. August Bang's Forlag, Copenhagen, p 166
Förster H (1976) Carbohydrates in parenteral nutrition. Nutr Metab 20 (Suppl 1):57
Hauschildt S, Chalmers RA, Lawson AM, Schultis K, Watts RWE (1976) Metabolic investigations after xylitol infusion in human subjects. Am J Clin Nutr 29:258
Keller U, Froesch ER (1972) Vergleichende Untersuchungen über den Stoffwechsel von Xylit, Sorbit und Fruktose beim Menschen. Schweiz Med Wochenschr 102:1017
Leutenegger AF, Göschke H, Stutz K, Mannhart H, Werdenberg D, Wolff G, Allgöwer M (1977) Comparison between glucose and a combination of glucose, fructose and xylitol as carbohydrates for total parenteral nutrition of surgical intensive care patients. Am J Surg 133:199
Schröder R, Féaux de Lacroix W, Franzen U, Klein PJ, Müller W (1974) Therapie-bedingte Form einer reno-cerebralen Oxalose? Acta Neuropathol (Berlin) 27:181
Stoner HB, Heath DF (1973) The effects of trauma on carbohydrate metabolism. Br J Anaesth 45:244
Thomas DW, Edwards JB, Gilligan JE, Lawrence JR, Edwards RG (1972) Complications following intravenous administration of solutions containing xylitol. Med J Aust 1:1238
Thomas DW, Gilligan JE, Edwards JB, Edwards RG (1972). Lactic acidosis and osmotic diuresis produced by xylitol infusion. Med J Aust 1:1246
Woolfson AMJ, Heatley RV, Allison SP (1979) Insulin to inhibit protein catabolism after injury. N Engl J Med 300:14
Author information
Authors and Affiliations
Additional information
This work was supported by grants from the Danish Medical Research Council (J.No. 512-15484), King Christian X's Foundation, P. Carl Petersen's Foundation and the Foundation for Advancement of Medical Science
Rights and permissions
About this article
Cite this article
Ladefoged, K., Berthelsen, P., Brøckner-Nielsen, J. et al. Fructose, xylitol and glucose in total parenteral nutrition. Intensive Care Med 8, 19–23 (1982). https://doi.org/10.1007/BF01686849
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01686849