
Abstract
Sixty-five patients with severe alpha1-antitrypsin (AAT) deficiency (phenotype PiZ) were followed with spirometry at regular intervals of one year and a median observation period of four years.
The annual decline in pulmonary function was adjusted for sex, age and height by division with the predicted normal pulmonary function. The median decline in FEV1 was 1.9% predicted/year. The rate of decline was independent of age and pulmonary function, except for patients with FEV1 below 25% of predicted normal.
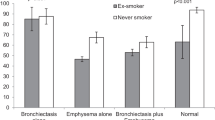
There was a tendency towards a slower median decline in FEV1 in exsmokers (1.7% predicted/year) compared to smokers (3.8% predicted/year) and never-smokers (3.7% predicted/year), however, this difference was not significant (p > 0.1). At the time of diagnosis smokers and ex-smokers had a lower FEV1 (44 and 38% predicted) than never-smokers (85% predicted) (p < 0.02), and smokers and ex-smokers were generally younger (median age 44 and 42 years, respectively) than never smokers (median age 55 years) (p > 0.1).
Our data indicate that smokers as well as nonsmokers with severe AAT deficiency are at risk of developing pulmonary emphysema. The disease seems to appear later in nonsmokers, though once initiated it progresses at the same rate.
Similar content being viewed by others
References
Larsson C (1978) Natural history and life expectancy in severe alpha1-antitrypsin deficiency, PiZZ. Acta Med Scand 204:345–351.
Gadek JE (1988) Alpha1-antitrypsin deficiency. Usage of alpha1-protease inhibitor concentrate in replacement therapy. Am J Med 84(suppl 6A)
Hubbard RC, Sellers S, Czerski D, Stephens L, Crystal RG (1988) Biochemical efficacy and safety of monthly augmentation therapy for alfa1-antitrypsin deficiency. JAMA 260:1259–1264
Quanjer PH (Compiler and Editor) (1983) Standardized lung function testing. Report Working Part ‘Standardization of Lung Function Tests,” European Community for Coal and Steel. Bull Europ Physiopat Resp 19(suppl 5):1–95
Fagerhol MK, Cox DW (1981) The Pi polymorphism: genetic, biochemical and clinical aspects of human alpha1-antitrypsin. Adv Hum Gen 11:1–62
Thymann M (1986) Distribution of Alpha1-antitrypsin (Pi) phenotypes in Denmark determined by separator isoelectric focusing in agarose gel. Hum Hered 36:19–23
Janus ED, Phillips NT, Carrell RW (1985) Smoking, lung function and alpha1-antitrypsin deficiency. Lancet i:152–154
Tobin MJ, Cook PJL, Hutchison CS (1983) Alpha1-antitrypsin deficiency: The clinical and physiological features in subjects homozygous for Pi type Z. Br J Dis Chest 77:14–27
Hutchison DCS (1988) Natural history of alpha1-protease inhibitor deficiency. Am J Med 84(suppl 6A):3–12
Brantly ML, Paul LD, Miller BH, Falk RT, Wu M, Crystal RG (1988) Clinical features and history of the destructive lung disease associated with alpha1-antitripysin deficiency in adults with pulmonary symptoms. Am Rev Resp Dis 138:327–336
Wu MC, Eriksson S (1988) Lung function, smoking and survival in severe alpha1-antitrypsin deficiency, PiZZ. J Clin Epidemiol 41:1157–1165
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Evald, T., Dirksen, A., Keittelmann, S. et al. Decline in pulmonary function in patients with α1-antitrypsin deficiency. Lung 168 (Suppl 1), 579–585 (1990). https://doi.org/10.1007/BF02718180
Issue Date:
DOI: https://doi.org/10.1007/BF02718180