
Abstract
Purpose: To review the clinical benefits of dextromethorphan (DM) in pain management, describe its neuropharmacological properties.
Source: A Medline search was made for experimental and clinical data on DM use from 1967 to date using keywordsnociception, acute and chronic pain control, N-methyl-D-aspartate, antagonists, dextromethorphan.
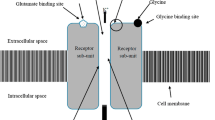
Principle findings: The 930 DM citations mostly described its antitussive, metabolic and toxicological aspects, animal studies and its possible role in minimizing post-brain ischemia complications in humans. The use of DM inacute pain revealed eight original studies involving 443 patients, as well as two preliminary reports and our own unpublished data on 513 patients. Most of the 956 patients had general anesthesia. Eight studies (154 patients) and one case report dealt withchronic pain management. This N-methyl-D-aspartate (NMDA) receptor antagonist binds to receptor sites in the spinal cord and central nervous system, thereby blocking the generation of central acute and chronic pain sensations arising from peripheral nociceptive stimuli and enabling reduction in the amount of analgesics required for pain control. DM attenuated the sensation ofacute pain at doses of 30–90 mg, without major side effects, and reduced the amount of analgesics in 73% of the postoperative DM-treated patients. Studies in secondary pain models in healthy volunteers and in various types ofchronic pain showed DM to be associated with unsatisfactory pain relief.
Conclusion: DM attenuatesacute pain sensation with tolerable side effects. Its availability in oral form bestow advantages over other NMDA antagonists.
Résumé
Objectif: Passer en revue les bénéfices cliniques du dextrométhorphane (DM) et décrire ses propriétés neuropharmacologiques.
Source: Une recherche dans Medline a fourni des données expérimentales et cliniques sur le DM, utilisé de 1967 à aujourd’hui, à l’aide des mots-clésnociception, soulagement de la douleur aiguë et chronique, N-méthyl-D-aspartate, antagonistes, dextrométhorphane.
Constations principales: Les 930 références trouvées décrivent surtout les aspects antitussifs, métaboliques et toxicologiques du DM, les études sur des animaux et le rôle possible dans la réduction des complications de l’ischémie cérébrale chez l’humain. Huit études originales auprès de 443 patients, deux rapports préliminaires et nos propres données non publiées sur 513 patients concernent le soulagement de la douleuraiguë. La majorité des 956 patients ont eu une anesthésie générale. Huit études (154 patients) et une observation portent sur le traitement de la douleurchronique. Cet antagoniste des récepteurs N-méthyl-D-aspartate (NMDA) se fixe sur les sites récepteurs dans la moelle épinière et le système nerveux central. Il empêche ainsi la propagation centrale des sensations de douleurs aiguës et chroniques provenant de stimuli nociceptifs périphériques, et contribue à la réduction de la quantité d’analgésiques nécessaires au traitement. Des doses de 30–90 mg de DM atténuent la sensation de douleuraiguë, sans produire d’effets secondaires importants, et permettent de réduire la quantité d’analgésiques chez 73 % des patients traités avec du DM après une intervention chirurgicale. Les études de modèles de douleurs secondaires chez des volontaires sains et de différents types de douleurschroniques, ont révélé que le DM n’apporte pas de soulagement de la douleur satisfaisant.
Conclusion: Le DM atténue la sensation de douleuraiguë et présente des effets secondaires acceptables. Son conditionnement sous forme orale lui confère des avantages sur d’autres antagonistes de NMDA.
Article PDF
Similar content being viewed by others

References
Plesan A, Hedman U, Xu XJ, Wiesenfeld-Hallin Z. Comparison of ketamine and dextromethorphan in potentiating the antinociceptive effect of morphine in rats. Anesth Analg 1998; 86: 825–9.
Klepstad P, Maurset A, Moberg ER, Oye I. Evidence of a role for NMDA receptors in pain perception. Eur J Pharmacol 1990; 187: 513–8.
Eisenberg E, Pud D. Can patients with chronic neuropathic pain be cured by acute administration of the NMDA receptor antagonist amantadine? Pain 1998; 74: 337–9.
Kinnman E, Nygards EB, Hansson P. Effects of dextromethorphan in clinical doses on capsaicin-induced ongoing pain and mechanical hypersensitivity. J Pain Symptom Manage 1997; 14: 195–201.
Kawamata T, Omote K, Kawamata M, Namiki A Premedication with oral dextromethorphan reduces postoperative pain after tonsillectomy. Anesth Analg 1998; 86: 594–7.
Woolf CJ, Chong MS. Preemptive analgesia — treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg 1993; 77: 362–79.
Bem JL, Peck R. Dextromethorphan. An overview of safety issues. Drug Saf 1992; 7: 190–9.
Battaglia G, Rustioni A Coexistence of glutamate and substance P in dorsal root ganglion neurons of the rat and monkey. J Comp Neurol 1988; 277: 302–12.
Aanonsen LM, Wilcox GL. Nociceptive action of excitatory amino acids in the mouse: effects of spinally administered opioids, phencyclidine andsigma agonists. J Pharmacol Exp Ther 1987; 243: 9–19.
Davies SN, Lodge D. Evidence for involvement ofN-methyl-D-aspartate receptors in ‘wind-up’ of class 2 neurones in the dorsal horn of the rat. Brain Res 1987; 424: 402–6.
Dickenson AH. Spinal cord pharmacology of pain. Br J Anaesth 1995; 75: 193–200.
Felsby S, Nielsen J, Arendt-Nielsen L, Jensen TS. NMDA receptor blockade in chronic neuropathic pain: a comparison of ketamine and magnesium chloride. Pain 1995; 64: 283–91.
Dickenson AH. A cure for wind up: NMDA receptor antagonists as potential analgesics. Trends Pharmacol Sci 1990; 11: 307–9.
Dickenson AH, Sullivan AF. Differential effects of excitatory amino acid antagonists on dorsal horn nociceptive neurones in the rat. Brain Res 1990; 506: 31–9.
Ilkjaer S, Petersen KL, Brennum J, Wernberg M, Dahl JB. Effect of systemicN-methyl-D-aspartate receptor antagonist (ketamine) on primary and secondary hyperalgesia in humans. Br J Anaesth 1996; 76: 829–34.
Grotta J, Clark W, Coull B, et al. Safety and tolerability of the glutamate antagonists CGS 19755 (Selfotel) in patients with acute ischemic stroke. Results of a phase IIa randomized trial. Stroke 1995; 26: 602–5.
Albers GW, Atkinson RP, Kelley RE, Rosenbaum DM. Safety, tolerability, and pharmacokinetics of theN-methyl-D-aspartate antagonist dextrorphan in patients with acute stroke. Stroke 1995; 26: 254–8.
Muir KW, Lees KR. Clinical experience with excitatory amino acid antagonist drugs. Stroke 1995; 26: 503–13.
Roytblat L, Korotkoruchko A, Katz J, Glazer M, Greemberg L, Fisher A. Postoperative pain: the effect of low-dose ketamine in addition to general anesthesia. Anesth Analg 1993; 77: 1161–5.
Mercadante S. Ketamine in cancer pain: an update. Palliat Med 1996; 10: 225–30.
Kornhuber J, Quack G, Danysz W, et al. Therapeutic brain concentration of the NMDA receptor antagonist amantadine. Neuropharmacology 1995; 34: 713–21.
Benson WM, Stefko PL, Randall LO. Comparative pharmacology of levorphanol, racemorphan and dextrorphan and related methyl ethers. J Pharmacol Exp Ther 1953; 109: 189–200.
Karlsson MO, Dahlström NA, Neil A. Characterization of high-affinity binding sites for the antitussive [3H] noscapine in guinea pig brain tissue. Eur J Pharmacol 1988; 145: 195–203.
Mendell LM. Physiological properties of unmyelinated fiber projection to the spinal cord. Exp Neurol 1966; 16: 316–32.
Church J, Lodge D, Berry SC. Differential effects of dextrorphan and levorphanol on the excitation of rat spinal neurons by amino acids. Eur J Pharmacol 1985; 111: 185–90.
Musacchio JM, Klein M. Dextromethorphan binding sites in the guinea pig brain. Cell Mol Neurobiol 1988; 8: 149–56.
Church J, Shacklock JA, Baimbridge KG Dextromethorphan and phencyclidine receptor ligands: differential effects on K+ and NMDA-evoked increases in cytosolic free Ca2+ concentration. Neurosci Lett 1991; 124: 232–4.
Ferkany JW, Borosky SA, Clissold DB, Pontecorvo MJ. Dextromethorphan inhibits NMDA-induced convulsions. Eur J Pharmacol 1988; 151: 151–4.
Choi DW. Dextrorphan and dextromethorphan attenuate glutamate neurotoxicity. Brain Res 1987; 403: 333–6.
Albers GW, Sáenz RE, Moses JA Jr,Choi DW. Safety and tolerance of oral dextromethorphan in patients at risk from brain ischemia. Stroke 1991; 22: 1075–7.
Bonuccelli U, Del Dotto P, Piccini P, Behge F, Corsini GU, Muratorio A. Dextromethorphan and parkinsonism (Letter). Lancet 1992; 340: 53.
Fisher RS, Cysyk BJ, Lesser RP, et al. Dextromethorphan for treatment of complex partial seizures. Neurology 1990; 40: 547–9.
Ziemann U, Chen R, Cohen LG, Hallett M Dextromethorphan decreases the excitability of the human motor cortex. Neurology 1998; 51: 1320–4.
Verhagen Metman L, Del Dotto P, Natté R, Van den Munchof P, Chase TN Dextromethorphan improves levodopa-induced dyskinesias in Parkinson’s disease. Neurology 1998; 51: 203–6.
Woodworth JR, Denis SRK, Moore L, Rotenberg KS. The polymorphic metabolism of dextromethorphan. J Clin Pharmacol 1987; 27: 139–43.
Musacchio JM, Klein M, Canoll PD. Dextromethorphan and sigma ligands: common sites but diverse effects. Life Sci 1989; 45: 1721–32.
Kiss IE, Killian M. Does opiate premedication influence postoperative analgesia? A prospective study. Pain 1992; 48: 157–8.
Tverskoy M, Oz Y, Isakson A, Finger J, Bradley EL Jr,Kissin I. Preemptive effect of fentanyl and ketamine on postoperative pain and wound hyperalgesia. Anesth Analg 1994; 78: 205–9.
Henderson DJ, Withington BS, Wilson JA, Morrison LMM. Perioperative dextromethorphan reduces postoperative pain after hysterectomy. Anesth Analg 1999; 89: 399–402.
Ilkjaer S, Dirks J, Brennum M, Wernberg M, Dahl JB. Effect of systemic N-methyl-D-aspartate receptor antagonist (dextromethorphan) on primary and secondary hyperalgesia in humans. Br J Anaesth 1997; 79: 600–5.
Price DD, Mao J, Frenk H, Mayer DJ. TheN-methyl-D-aspartate receptor antagonist dextromethorphan selectivity reduces temporal summation of second pain in man. Pain 1994; 59: 165–74.
Chia YY, Liu K, Chow LH, Lee TY. The operative administration of intravenous dextromethorphan reduces postoperative morphine consumption. Anesth Analg 1999; 89: 748–52.
Yamamoto T, Yaksh TL. Comparison of the antinociceptive effects of pre-and posttreatment with intrathecal morphine and MK-801, an NMDA antagonist, on formalin test in rat. Anesthesiology 1992; 77: 757–63.
Rose JB, Cuy R, Cohen DE, Schreiner MS. Preoperative oral dextromethorphan does not reduce pain or analgesic consumption in children after adenotonsillectomy. Anesth Analg 1999; 88: 749–53.
Grace RF, Power I, Umedaly H, et al. Preoperative dextromethorphan reduces intraoperative but not postoperative morphine requirements after laparotomy. Anesth Analg 1998; 87: 1135–8.
Wu CT, Yu YC, Yeh CC, et al. Preincisional dextromethorphan treatment decreases postoperative pain and opioid requirement after laparoscopic cholecystectomy. Anesth Analg 1999; 88: 1331–4.
Wong CS, Wu CT, Yu JC, Yeh CC, Lee MMS, Tao PL. Preincisional dextromethorphan decreases postoperative pain and opioid requirement after modified radical mastectomy. Can J Anesth 1999; 46: 1122–6.
Caruso FS, Mehlisch DR, Minn FL, Daniels SE, Nemarich AN, Conforto ME. Synergistic analgesic interaction of morphine with dextromethorphan, an NMDA receptor antagonist in oral surgery pain. (Abstract) Clin Pharmacol Ther 1998; 63: 139.
Minn FL, Nelson SL, Brahim J, Caruso FS. Superior analgesic activity of morphine with dextromethorphan, an NMDA receptor antagonist in oral surgery pain. (Abstract) Clin Pharmacol Ther 1998; 63: 140.
McConaghy PM, McSorley P, McCaugey W, Campbell WI. Dextromethorphan and pain after total abdominal hysterectomy. Br J Anaesth 1998; 81: 731–6.
Kauppila T, Grönroos M, Pertovaara A An attempt to attenuate experimental pain in humans by dextromethorphan, an NMDA receptor antagonist. Pharmacol Biochem Behav 1995; 52: 641–4.
McQuay HJ, Carroll D, Jadad AR, et al. Dextromethorphan for the treatment of neuropathic pain: a double-blind randomized controlled crossover trial with integral n-of-1 design. Pain 1994; 59: 127–33.
Mercadante S, Casuccio A, Genovese G Ineffectiveness of dextromethorphan in cancer pain. J Pain Symptom Manage 1998; 16: 317–22.
Suzuki T, Kato J, Saeki S, Ogawa S, Suzuki H. Analgesic effect of dextromethorphan for postherpetic neuralgia. (Japanese) Masui 1996; 45: 629–33.
Nelson KA, Park KM, Robinovitz E, Tsigos C, Max MB. High dose oral dextromethorphan versus placebo in painful diabetic neuropathy and postherpetic neuralgia. Neurology 1997; 48: 1212–8.
Goto T, Marota JJA, Crosby G Nitrous oxide induces preemptive analgesia in the rat that is antagonized by halothane. Anesthesiology 1994; 80: 409–16.
Berkowitz BA, Ngai SH, Fink AD. Nitrous oxide “analgesia”: resemblance to opiate action. Science 1976; 194: 967–8.
Kastrup J, Petersen P, Dejgård A, Angelo HR, Hilsted J. Intravenous lidocaine infusion — a new treatment of chronic painful diabetic neuropathy? Pain 1987; 28: 69–75.
Rowbotham M, Harden N, Stacey B, Bernstein P, Magnus-Miller L. Gabapentin for the treatment of postherpetic neuralgia. JAMA 1998; 280: 1837–42.
Cherny NI, Thaler HT, Friedlander-Klar H, et al. Opioid responsiveness of cancer pain syndromes caused by neuropathic or nociceptive mechanisms: a combined analysis of controlled, single-dose studies. Neurology 1994; 44: 857–61.
Sindrup SH, Andersen G, Madsen C, Smith T, Brøsen K, Jensen TS. Tramadol relieves pain and allodynia in polyneuropathy: a randomized, double-blind, controlled trial. Pain 1999; 83: 85–90.
Sindrup SH, Bjerre U, Dejgaard A, Brøsen K, Aaes-Jørgensen T, Gram LF. The selective serotonin reuptake inhibitor citalopram relieves the symptoms of diabetic neuropathy. Clin Pharmacol Ther 1992; 52: 547–52.
Verthem M, Boivie J, Arnqvist H, Holmgren H, Lindström T, Thorell LH. A comparison of amitripyyline and maprotiline in the treatment of painful polyneuropathy in diabetics and nondiabetics. Clin J Pain 1997; 13: 313–23.
Low PA, Opfer-Gehrking TL, Dyck PJ, Litchy WJ, O’Brien PC. Double-blind, placebo-controlled study of the application of capsaicin cream in chronic distal painful polyneuropathy. Pain 1995; 62: 163–8.
Vinik AI. Diabetic neuropathy: pathogenesis and therapy. Am J Med 1999; 107: 17S-26S.
Sindrup SH, Jensen TS. Efficacy of pharmacological treatment of neuropathic pain: an update and effect related to mechanism of drug action. Pain 1999; 83: 389–400.
Kristensen JD, Post C, Gordh T Jr,Svensson BA Spinal cord morphology and antinociception after chronic intrathecal administration of excitatory amino acid antagonists in the rat. Pain 1993; 54: 309–16.
Eide PK, Stubhaug A, Øye I, Breivik H. Continuous subcutaneous administration of theN-methyl-D-aspartic acid (NMDA) receptor antagonist ketamine in the treatment of postherpetic neuralgia. Pain 1995; 61: 221–8.
Max MB, Byas-Smith MG, Gracely RH, Bennett GJ. Intravenous infusion of the NMDA antagonist, ketamine in chronic posttraumatic pain with allodynia: a double-blind comparison to alfentanyl and placebo. Clin Neuropharmacol 1995; 18: 360–8.
Elliott KJ, Brodsky M, Hynansky AD, Foley KM, Inturrisi CE. Dextromethorphan suppresses both formalin-induced nociceptive behavior and the formalin-induced increase in spinal cord c-fos mRNA. Pain 1995; 61: 401–9.
Mao J, Price DD, Hayes RL, Lu J, Mayer DJ, Frenk H Intrathecal treatment with dextromethorphan or ketamine potently reduces pain-related behaviors in a rat model of peripheral mononeuropathy. Brain Res 1993; 605: 164–8.
Hao JX, Xu XJ. Treatment of a chronic allodynia-like response in spinally injured rats: effects of systematically administered excitatory amino acid receptor antagonists. Pain 1996; 66: 279–85.
Steinberg GK, Bell TE, Yenari MA Dose escalation safety and tolerance study of theN-methyl-D-aspartate antagonist dextromethrophan in neurosurgery patients. J Neurosurg 1996; 84: 860–6.
Tal M, Bennet GJ. Dextrorphan relieves neuropathic heat-evoked hyperalgesia in the rat. Neurosci Lett 1993; 151: 107–10.
Sugimoto T, Bennett GJ, Kajander KC Transsynaptic degeneration in the superficial dorsal horn after sciatic nerve injury: effects of chronic constriction injury, transection, and strychnine. Pain 1990; 42: 205–13.
Author information
Authors and Affiliations
Corresponding author
Additional information
This review was facilitated by aid from the “Anonymous Italian Family Foundation”, Milan, Italy.
Rights and permissions
About this article
Cite this article
Weinbroum, A.A., Rudick, V., Paret, G. et al. The role of dextromethorphan in pain control. Can J Anesth 47, 585–596 (2000). https://doi.org/10.1007/BF03018952
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018952