
Abstract
IRX-2, a natural cytokine biological with multiple components, has been used in preclinical and clinical studies to promote antitumor activity of T lymphocytes. To define cellular mechanisms responsible for antitumor effects of IRX-2, its ability to induce effector T cells (Teff) was examined in a model simulating the tumor microenvironment. An in vitro model containing conventional CD4+CD25− cells co-cultured with autologous immature dendritic cells, irradiated tumor cells, and cytokines was used to study differentiation and expansion of regulatory T cells (Treg) and Teff in the presence and absence of IRX-2. Phenotype, suppressor function, signaling, and cytokine production were serially measured using flow cytometry, Western blots, CFSE-based suppressor assays, and Luminex-based analyses. The presence of IRX-2 in the co-cultures promoted the induction and expansion of IFN-γ+Tbet+ Teff and significantly (p < 0.01) decreased the induction of inducible IL-10+TGF-β+ Treg. The responsible mechanism involved IFN-γ-driven T cell polarization towards Teff and suppression of Treg differentiation. In an in vitro model simulating the human tumor microenvironment, IRX-2 promoted Teff expansion and antitumor activity without inducing Treg. Thus, IRX-2 could be considered as a promising component of future antitumor therapies.
Similar content being viewed by others

Introduction
IRX-2 is a novel biologic containing low doses of cytokines. It is produced by stimulating human peripheral blood mononuclear cells (PBMC) with phytohaemagglutinin (PHA). IRX-2 has been used in clinical trials for the treatment of head and neck cancer (HNC) patients with encouraging results and tolerable side effects [1]. The delivery of IRX-2 to tumor-draining lymph nodes (LN) of HNC patients reduced pain and dysphagia, decreased tumor size and, in some patients, prolonged disease-free and overall survival [1, 2]. IRX-2 also increased the number of circulating naive and memory T cells [3], enriched T cells in tumor-draining LN [4], and promoted lymphocyte infiltrations into the tumors [5]. In addition, in vitro studies showed that IRX-2 enhanced dendritic cell (DC) maturation [6] and protected cytotoxic T lymphocytes from tumor-induced apoptosis [7]. Delivering of IRX-2 to tumor-draining LN or into the tumor microenvironment was based on the rationale that IRX-2 might alter local cell-to-cell interactions, promote antitumor responses, and reduce tumor-induced immunosuppression. Human tumors create and maintain an environment enriched in immunosuppressive cytokines, IL-10 and/or TGF-β, immunosuppressive factors PGE2 or adenosine, and in regulatory T cells (Treg) [8]. Thus, tumor-infiltrating immune cells are dysfunctional and prone to apoptosis [8]. It has been suggested that accumulations of Treg in the tumor microenvironment contribute to the dysfunction of effector T cells [8].
While the available in vitro and in vivo data suggest that IRX-2 enhances immune activation [5], the molecular mechanisms responsible for IRX-2-mediated effects in the tumor microenvironment are unknown. To evaluate IRX-2-mediated effects on Teff and Treg, we used a previously described in vitro model [9], in which human conventional CD4+CD25− T cells are co-cultured with autologous immature DC and with irradiated tumor cells in the presence of low doses of recombinant human (rh) IL-2, IL-10, and IL-15. This model mimics the tumor microenvironment and favors the generation of Treg from conventional CD4+CD25− T cells [9]. The addition of IRX-2 to this system allowed us to explore the cellular and molecular mechanisms responsible for its ability to activate immune cells in the tumor microenvironment.
Material and methods
IRX-2
To date, more than 40 patients have been treated with IRX-2 in several Food and Drug Administration (FDA)-approved clinical trials [2, 5]. IRX-2 is produced under current good manufacturing practice (cGMP) conditions by stimulation of human PBMCs with PHA for 24 h. PBMCs are obtained from pretested leukocyte buffy coats purchased from FDA-licensed blood banks. PHA and all cellular elements are removed by centrifugation and washing. DNA is removed by anion exchange chromatography. The cell-free supernatant is nanofiltered for viral clearance, filter sterilized, and formulated to defined specifications for IL-2 and other cytokine levels. Stringent QC testing including bioassays and ELISA for cytokine levels assures the consistency of the IRX-2. As part of the release criteria for clinical use of IRX-2, four cytokines (IL-1β, IL-2, TNF-α, and IFN-γ) are routinely measured in ELISA assays standardized against World Health Organization (WHO) international standards. Testing for sterility, DNA, mycoplasma, endotoxin, and viral nucleic acid for cytomegalovirus and Epstein–Barr virus are also part of the cGMP process. The IRX-2 lot used for our experiments contains several cytokines at the concentrations listed in Table 1.
Generation of immature DC and isolation of CD4+CD25− cells
PBMCs were isolated by Ficoll-Hypaque (GE Healthcare, Uppsala, Sweden) gradient centrifugation from buffy coats purchased from the Central Blood Bank of Pittsburgh. Monocytes were isolated by plastic adherence at 37°C for 2 h. Non-adherent cells were removed by washing. Adherent cells were cultured in AIM V medium (Gibco Invitrogen, Carlsbad, CA) containing 1,000 IU/mL IL-4 (Cellgenix, Freiburg, Germany) and 1,000 IU/mL GM-CSF (Bayer, Seattle, WA). Immature monocyte-derived DC (iDC) were harvested on day 6. CD4+CD25− T cells were isolated from the remaining non-adherent cells by magnetic bead separation using Treg isolation kits (Miltenyi, Auburn, CA) as recommended by the manufacturer and cryopreserved.
Cell culture
PCI-13, an HNC cell line, established and maintained in our laboratory [10] was cultured in RPMI 1640 medium (Lonza) supplemented with 10% (v/v) heat-inactivated fetal bovine serum (FBS), l-glutamine 2 mmol/l, 100 IU/mL penicillin, and 100 μg/mL streptomycin in an atmosphere of 5% CO2 in air at 37°C. K562, a human leukemic cell line, was purchased from ATCC and cultured in RPMI 1640 supplemented with 10% heat-inactivated FBS, l-glutamine, penicillin, and streptomycin. The cells were routinely tested for Mycoplasma and endotoxin levels and were found to be negative.
The co-culture model system
The in vitro model simulating the human tumor microenvironment contained 5 × 105 iDC co-cultured with 5 × 105 irradiated (3,000 rad) PCI-13 cells and autologous CD4+CD25− T cells (5 × 106) in six-well plates [9]. Each well contained 2.5 mL complete AIM V medium. Plates were cultured in an atmosphere of 5% CO2 in air at 37°C for 10 days. In addition, 2.5 mL aliquots of IRX-2 or X-Vivo 10 medium (control) were added to each well as well as rhIL-2 (10 IU/mL), IL-10 (20 IU/mL), and IL-15 (20 IU/mL) (Peprotech, Rocky Hill, NJ). On days 3, 6, and 9, half of the medium was removed and replaced with fresh cytokine-containing medium mixed 1:1 with medium or IRX-2. For cytokine assays, cells were stimulated for 16 h with anti-CD3/CD28-coated beads (Miltenyi) at the bead:cell ratio of 1:1 in complete AIM V medium without exogenous cytokines or IRX-2. For intracellular cytokine staining, Brefeldin A (2 μg/mL, Sigma-Aldrich, St. Louis, MO) was added to the cells.
Flow cytometry staining and antibodies
The following anti-human flourochrome-conjugated antibodies were purchased from Beckman Coulter: anti-CD4-ECD, anti-CD3-PeCy5, anti-CD25-FITC, anti-CD25-PE, and anti-CTLA4-PE. In addition, anti-IL-10-FITC was purchased from R&D Systems. Anti-CD122-PE and anti-CD132-PE were obtained from BD Pharmigen and anti-TGF-β1 (clone TB21) from IQ products (Groningen, Netherlands). Anti-FOXP3-FITC (clone PCH101), anti-IL-17-PE, and anti-T-bet-PE were from eBioscience. A PE-conjugated anti-phospho-Akt (Ser473) was purchased from Cell Signaling as was an unconjugated mouse anti-Akt antibody. A PE-conjugated donkey anti-mouse Fab was purchased from eBioscience.
For staining, cells were harvested, washed, and incubated with human Fc-block (eBioscience, San Diego, CA) according to the manufacturer’s instructions. Antibodies were added, and staining was performed for 20 min on ice. Cells were washed and fixed with phosphate-buffered saline (PBS) containing paraformaldehyde 2% (w/v in PBS) prior to analysis. For intracellular staining, cells were permeabilized using a Fix/Perm Kit from eBioscience. For FOXP3 and T-bet detection, a staining kit from eBioscience was used. Incubations were performed on ice for 30 min, and washed cells were acquired on the same day. Incubations with a labeled secondary antibody were performed for 30 min on ice. For intracellular staining of Akt and phospho-Akt, cells were fixed with 2% paraformaldehyde (w/v) in PBS and permeabilized with ice-cold methanol. Incubations with primary antibodies were performed for 1 h at room temperature.
Luminex
Cytokine levels in cell supernatants were measured using the Luminex© technology according to the manufacturer’s instructions (Invitrogen, Carlsbad, CA).
Western blots
Cells were washed, centrifuged at 4°C, and lysed in equal volumes of ice-cold lysis buffer [50 mM Tris–HCl (pH 7.5), 150 mM NaCl, 0.5% Nonidet P-40] and protease inhibitor cocktail (Pierce Chemical Co., Rockford, IL, USA). Homogenates were clarified by centrifugation. Supernatants were boiled for 5 min in Laemmli sample buffer (Bio-Rad, Hercules, CA). Equivalent protein quantities, as determined by Lowry, were loaded on each gel. Proteins were separated by SDS-PAGE electrophoresis and electrotransferred to polyvinylidene difluoride membranes. The membranes were developed as previously described [7]. Primary antibodies against human STAT molecules were purchased from Cell Signaling, and a horseradish peroxidase-conjugated secondary antibody from Pierce Chemical Company.
CFSE-based suppression assay
Suppression of proliferation of CD4+CD25− T cells was performed as previously described [11]. Briefly, CD4+CD25− responder cells (RC) labeled with 1.5 μM carboxyfluorescein succinimidyl ester (CFSE, Invitrogen, Carlsbad, CA) were cultured in complete AIM V medium in the presence of 150 IU/mL rhIL-2 and 1 μg/mL anti-CD28 mAb (Miltanyi) in wells of 96-well plates (105/well) coated with anti-CD3 mAb (1 μg/mL, eBioscience). T cells harvested from the IVA co-cultures were added to the RC at different ratios and cultures were incubated in 5% CO2 in air at 37°C. Flow cytometry analyses were performed on day 4, the ModFit LT software provided by Verity Software House Inc. was used for data processing (Topsham, ME).
Statistical analysis
Data were analyzed using paired Student’s t tests. The p values <0.05 were considered significant.
Results
IRX-2 promotes expansion of Teff
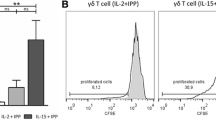
CD4+CD25− T cells in the co-cultured in our in vitro system proliferate and differentiate into adaptive Treg (Tr1) with a distinctive phenotype [9]. The addition of IRX-2 to co-cultures had no impact on cell proliferation or their viability (Fig. 1a). T cells placed in culture (day 0) were CD3+CD4+CD25−CD122−CD132−CD152−FOXP3−. On day 0, co-cultures contained few (0.4 ± 0.1 × 106) IFN-γ+ Teff and no Tr1 (Fig. 1b). The cells become CD25+, CD122+, CD132+, CD152+, and FOXP3+ (Fig. 2a, b), and the frequency of T cells expressing IL-10, TGF-β1, and IFN-γ is significantly increased by day 10 (Fig. 2c, d). In the course of the co-culture, the starting population gradually acquires the Tr1 phenotype in the absence of IRX-2 (Fig. 1b, gray lines), and the number of Teff increases only slightly to 1.1 ± 0.2 × 106 on day 10. In contrast, upon IRX-2 addition, the number of outgrowing Tr1 decreases while that of Teff increases (Fig. 1b, black lines). The addition of IRX-2 to the co-culture resulted in a dose-dependent change in the phenotype of proliferating T cells and in a significant decrease in the proportion of T cells with the Tr1 phenotype (Fig. 1b). The maximal effects were observed with IRX-2 used at the 1:1 dilution. As shown in Fig. 2a, b, the mean percentages of CD3+CD4+ cells expressing CD25 (53% vs. 24%), CD122 (55% vs. 20%), CD132 (57% vs. 25%), CD152 (57% vs. 29%), and FOXP3 [49% vs. 28%, mean fluorescence intensity (MFI) 12.6 vs. 6.3] were lower (p < 0.01 for all) when the cells were cultured in the presence of IRX-2. In addition, as shown in Fig. 2c, d, in the presence of IRX-2, the percentage of IL-10+ and TGF-β1+ T cells decreased, while that of IFN-γ+ cells increased. In the absence of IRX-2, the mean percentage of IL-10+ cells within the CD3+CD4+ T cells was 57%, and 62% were TGF-β1+, while only 10% were IFN-γ+. In the presence of IRX-2, only 22% cells were IL-10+ (p < 0.01) and 34% were TGF-β1+ (p < 0.01), while T cells expressing INF-γ increased to 34% (p < 0.01). IL-17 was not detectable in any of these co-cultures (Fig. 2d).

IRX-2 effects on Tr1 and Teff cells in the co-culture model. a Proliferation and viability of cells cultured in the presence or absence of IRX-2. Mean number of cells ± SD and mean viability from four independent experiments are shown. b The outgrowth of Teff and Tr1 in 10-day co-cultures: Cells were cultured in the presence (black lines) or absence of IRX-2 (gray lines). Cells were sampled, counted, and phenotyped by flow cytometry at the indicated time points. IRX-2 decreased the number of outgrowing Tr1 (p < 0.01) and increased the number of Teff as compared to co-cultures in the absence of IRX-2. The data are mean numbers of cells ± SD established in three independent experiments

Phenotype of CD4+CD25− T cells after 10-day co-culture ±IRX-2. a Representative histograms of T cells cultured for 10 days in the presence or absence of IRX-2. b Cells cultured in the presence of IRX-2 (black bars) expressed significantly lower levels of the Tr1-associated markers: CD25, CD122, CD132, CD152, and FOXP3 (*p < 0.01). c Representative histograms for intracellular cytokine staining on day 10 of co-culture. d The percentages of IL-10+ and TGF-β+ cells were lower when T cells were cultured in the presence of IRX-2, while the percentages of IFN-γ+ were higher relative to those cultured in the absence of IRX-2 (*p < 0.01). The cultured cells were phenotyped on day 10. The data obtained from five independent experiments are shown as mean percentages ± SD of positive cells in the CD3+CD4+ gate
T cells cultured in the presence of IRX-2 predominantly produce Teff cytokines
The cytokine profile of the T cells generated in the presence or absence of IRX-2 was analyzed in Luminex-based assays using culture supernatants. Luminex assays of IRX-2 mixed 1:1 with complete AIM V medium showed low levels of IL-4 (16 pg/mL), IL-10 (79 pg/mL), and IL-17 (25 pg/mL). As shown in Fig. 3, restimulation of T cells generated in the presence of IRX-2 with anti-CD3/CD28 Ab-coated beads for 24 h resulted in significantly higher levels of IFN-γ (3,129 vs. 975 pg/mL/106, p < 0.01) than restimulation of those cells generated in control cultures (medium alone). In contrast, T cells cultured in the absence of IRX-2 produced significantly higher levels of IL-10 (1,680 vs. 740.5 pg/mL/106, p < 0.01) and TGF-β1 (881 vs. 290 pg/mL/106, p < 0.01) (Fig. 3). These data show that the addition of IRX-2 favored the induction of IFN-γ-producing Teff, while in the absence of IRX-2, mainly IL-10- and TGF-β1-producing Tr1 were induced in the co-cultures.

Profile of cytokines secreted by cultured T cells ±IRX-2. T cells were harvested from co-cultures on day 9 and were stimulated with anti-CD3/CD28 Ab-coated beads for 24 h. The supernatants were analyzed for cytokine levels. In the presence of IRX-2 (black bars), T cells secreted significantly more IFN-γ (*p < 0.01) than those cultured in its absence (open bars), while IL-4 levels were not different (p > 0.05). In addition, supernatants from cells cultured in the presence of IRX-2 produced lower levels of IL-10 and TGF-β (*p < 0.01). The data are mean concentrations of cytokines ± SD from five independent experiments
T cells polarized in the presence of IRX-2 show low suppressor function
Next, in CFSE-based proliferation assays, we measured suppression of the proliferation of autologous RC by T cells generated in the presence or absence of IRX-2. Figure 4 shows that T cells induced in the absence of IRX-2 mediate significantly stronger suppression of RC proliferation than T cells generated in the presence of IRX-2 (67% vs. 35% suppression, p < 0.05). Consistent with the phenotype and the cytokine profile of T cells generated in the presence of IRX-2, their suppressor function was significantly reduced relative to that of T cells cultured without IRX-2.

Suppression mediated by T cells generated in co-cultures ±IRX-2. Cells harvested from co-cultures on day 10 were added to CFSE-labeled autologous responder cells at different ratios as described in the “Materials and methods” section. A cell–dose-dependent suppression of RC proliferation by T cells generated ±IRX-2 is presented. T cells cultured in the presence of IRX-2 showed lower suppression of proliferation (*p < 0.05). The data are mean percentages of suppression ± SD from four independent experiments
IRX-2 upregulates T-bet and pAkt but downregulates pSTAT5 in T cells
To identify molecular pathways responsible for the effects mediated by IRX-2, induction of T-bet, the transcription factor which is critical for the development of Th1 cells [12], was examined in T cells generated ±IRX-2 in the co-culture system. As shown in Fig. 5a, b, intracellular staining revealed significantly higher levels of T-bet in T cells cultured in the presence of IRX-2 as compared to those cultured in media alone (mean MFI 0.93 vs. 2.7, p < 0.01). Next, we observed that IRX-2 induced greater Akt phosphorylation in T cells as compared to controls (mean MFI 9.4 vs. 13, p < 0.01) (Fig. 5c, d), while total Akt levels were not significantly different (mean MFI 6.8 vs. 7, p > 0.05). Western Blot analyses for STAT signaling in T cells demonstrated lower levels of phosphorylated STAT5 (pSTAT5) in T cells cultured in the presence of IRX-2 than those cultured in its absence, while the total STAT5 levels were unchanged (Fig. 5f).

Effects of IRX-2 on T cell signaling. T cells were cultured for 10 days, harvested, and tested for the expression of intracellular T-bet, Akt, and pAkt by flow cytometry. a, c, and e show representative histograms gated on CD3+CD4+ cells cultured in the presence (closed line) or absence (open line) of IRX-2. Isotype controls are shown in gray. Cells cultured in the presence of IRX-2 express higher levels of T-bet (a, b, *p < 0.01) and pAkt (c, d, *p < 0.01) while expression of total Akt did not differ between IRX-2 and control (e, p > 0.05). The data in bar plots are mean MFI ± SD of cells gated on CD3+CD4+ from four independent experiments harvested on day 10. f A representative Western blot of three experiments performed shows data obtained with lysates of cells prepared on day 10. Total STAT5 expression (middle row) was similar after a co-culture ±IRX-2. T cells cultured +IRX-2 contained a lower level of pSTAT5 level (upper row). K562 cell line constitutively expressing pSTAT5 served as a positive control. Freshly isolated PBMC also expressed pSTAT5
IRX-2 treatment does not increase Treg numbers in the patients’ peripheral blood
Since IRX-2 contains IL-2, we expected it to increase the frequency of circulating Treg when given to patients with cancer as previously reported for rhIL-2 or antitumor vaccines [13]. We were able to study peripheral blood specimens obtained from the HNC patients treated with the IRX-2 as part of the recently completed phase II trial with IRX-2 [Berinstein et al., submitted]. Twenty-five patients with HNC received neoadjuvant therapy with IRX-2 prior to surgery. IRX-2 was delivered perilymphatically each day for 10 days starting on day 4 and following an infusion of low dose cyclophosphamide on day 1 and daily oral indomethacin and zinc in multivitamins [Berinstein et al., submitted]. Peripheral blood specimens were obtained from each patient pre- (day 1) and post- (day 21) IRX-2 therapy, and the frequency as well the absolute numbers of CD3+CD4+CD25hi T cells were determined. Consistent with our previous reports [14], the Treg frequency was increased in HNC patients prior to therapy (12 ± 3% mean ± SEM in the CD3+CD4+ gate) as compared to normal controls (2 ± 1.5%). The percentage of Treg remained unchanged after IRX-2 therapy (pre 6.7 ± 0.6% vs. post 7.5 ± 0.8%), and so did their absolute number (pre, 53 ± 6/ μL vs. post, 52 ± 7/μL, mean ± SEM). The ratio of CD8+ Teff cells to Treg remained unchanged at 6.6 in the patients’ peripheral blood. These data indicated that unlike rhIL-2, IRX-2 did not increase the frequency of Treg in the patients’ peripheral blood.
Discussion
This study evaluated the effects of a novel immunotherapeutic, IRX-2, on T cell polarization in an in vitro model simulating the human tumor microenvironment. In this model, IRX-2 prevented the induction of inducible Treg (Tr1) and favored the differentiation of Teff.
We previously reported the increased frequency of Treg in the peripheral blood and within tumor-infiltrating lymphocytes (TIL) of HNC patients [14, 15]. The prognostic impact of Treg accumulations in HNC is unknown [14, 16], although in other human solid tumors, the increased Treg frequency among TIL has been variously linked to better or worse prognosis [17–20]. In HNC, infiltrations of primary tumors with activated CD4+ T cells have been reported to correlate with improved overall survival [21]. This suggests that therapies increasing Teff within TIL could be beneficial in HNC and that alterations in the tumor microenvironment could benefit antitumor immunity.
CD4+ T cells are characterized by plasticity [12]. CD4+ T cells cultured in the absence of IRX-2 acquired the Treg phenotype and immunosuppressive cytokine profile. In contrast, in the presence of IRX-2 CD4+ T cells had a phenotype characteristic of Teff and produced IFN-γ rather than TGF-β1 and IL-10. Thus, IRX-2 favored CD4+ T cell differentiation into Teff rather than Tr1. Functionally, T cells cultured in the absence of IRX-2 were strongly suppressive, while T cells polarized by IRX-2 mediated significantly reduced suppression. IRX-2 did not completely prevent the induction of Tr1 but rather shifted the ratio of Treg/Teff towards Teff. Specifically, the average TGF-β1/IFN-γ ratio was 6:1 without IRX-2 vs. 1:1.2 with IRX-2. IRX-2 did not affect T cell proliferation or their viability, suggesting that it does not eliminate any T cells but rather expands Teff.
We and others have reported that inhibition of the mammalian target of rapamycin (mTOR) pathway with rapamycin promotes Treg expansion [22, 23], while activation of the Akt–mTor pathway antagonizes the induction of FOXP3+ cells [24]. A significant increase in the level of pAkt is observed when T cells are cultured in the presence of IRX-2. In human Treg, the restoration of Akt activity reduces Treg-mediated suppression [25]. Thus, enhanced Akt phosphorylation by IRX-2, leading to activation of the Akt–mTOR pathway, is a likely mechanism responsible for shifting the balance toward Teff differentiation and reduction of FOXP3 expression in the co-culture system. Also, IRX-2-mediated Akt activation was shown to protect CD4+ and CD8+ T cells from tumor-induced apoptosis [7].
The differentiation of Teff is known to be influenced by IFN-γ, which stabilizes T-bet expression [26]. Also, IFN-γ facilitates the conversion of CD4+CD25− cells into functional CD4+CD25+FOXP3+ Treg in humans and mice [27]. Thus, its presence in the co-culture could influence differentiation of Teff as well as Treg. IRX-2 contains considerable levels of IFN-γ (e.g., 2.2 ng/mL). Thus, T-bet expression and thereby Teff induction in the presence of IRX-2 might be driven by IFN-γ. IRX-2 contains multiple naturally occurring cytokines, and it is possible that more than one cytokine contributes to a shift in the phenotype and function of cultured T cells.
IL-2 is known to promote T cell-mediated antitumor immunity in patients with cancer [28]. It is also required for Treg expansion and activity [29]. In renal cell carcinoma and melanoma patients treated with a high dose of rhIL-2, significant increases of Treg in the peripheral circulation were reported [13]. In contrast, we did not observe increases in numbers or frequency of Treg in HNC patients treated with neoadjuvant IRX-2 in the phase II trial, although IRX-2 contained ∼6 ng (i.e., 125 IU/mL) of IL-2. Furthermore, an increase in lymphocytic infiltrates in tumor samples obtained from HNC patients before and after the neoadjuvant IRX-2 treatment was associated with improved survival [Berinstein et al., submitted].
In vivo, Treg survival critically depends on the activation of the IL-2 receptor and STAT5 signaling [29, 30]. CD25- or CD122-deficient mice lack Treg and STAT5-deficient mice show dramatically decreased Treg frequency because Foxp3 expression is directly controlled by activation of STAT5 [31]. It has also been suggested that the inhibition of Akt/mTOR pathway in the presence of IL-2 leads to persistent activation of STAT5 and Treg expansion [23]. Limiting STAT5 phosphorylation decreases Treg suppressor function [32]. IL-2-induced STAT5 activation provides an explanation for the increased Treg frequency in cancer patients treated with rhIL-2 [13]. The observed lower pSTAT5 levels in T cells cultured with IRX-2 suggests that IRX-2 favors Teff differentiation rather than Treg expansion. Further, IRX-2 did not increase the Treg frequency or numbers in the peripheral circulation of patients treated with IRX-2 in the recent phase II clinical trial [Berinstein et al., submitted].
In tumor-bearing hosts, the induction of robust antitumor responses is desirable. The ability to manipulate the tumor microenvironment so that it favors the differentiation of Teff cells rather than Treg represents a promising immunotherapeutic strategy. While many current therapies aim at eliminating or silencing Treg, the alternative approach of protecting and augmenting functions of Teff is equally important. In this study, using an in vitro model simulating the tumor microenvironment, we show that IRX-2 promotes Teff differentiation and helper functions without inducing Treg. In the clinic, IRX-2 administered to the vicinity of tumor-draining LN in HNC patients exerted multiple effects on immune cells and prolonged survival [Berinstein et al., submitted]. Thus, IRX-2 might be a promising component of future cancer therapies.
References
Wolf GT, Fee WE, Jr., Dolan RW, Moyer JS, Kaplan MJ, Spring PM, Suen J, Kenady DE, Newman JG, Carroll WR et al. (2011) Novel neoadjuvant immunotherapy regimen safety and survival in head and neck squamous cell cancer. Head Neck. doi:10.1002/hed.21660
Freeman SM, Franco JL, Kenady DE, Baltzer L, Roth Z, Brandwein HJ, Hadden JW (2011) A phase 1 safety study of an irx-2 regimen in patients with squamous cell carcinoma of the head and neck. Am J Clin Oncol 34(2):173–178. doi:10.1097/COC.0b013e3181dbb9d8
Hadden JW, Verastegui E, Hadden E (2007) IRX-2 and thymosin alpha1 (Zadaxin) increase T lymphocytes in T lymphocytopenic mice and humans. Ann N Y Acad Sci 1112:245–255. doi:10.1196/annals.1415.032
Meneses A, Verastegui E, Barrera JL, de la Garza J, Hadden JW (2003) Lymph node histology in head and neck cancer: impact of immunotherapy with IRX-2. Int Immunopharmacol 3:1083–1091. doi:10.1016/S1567-5769(03)00017-1
Hadden J, Verastegui E, Barrera JL, Kurman M, Meneses A, Zinser JW, de la Garza J, Hadden E (2003) A trial of IRX-2 in patients with squamous cell carcinomas of the head and neck. Int Immunopharmacol 3:1073–1081. doi:10.1016/S1567-5769(03)00029-8
Egan JE, Quadrini KJ, Santiago-Schwarz F, Hadden JW, Brandwein HJ, Signorelli KL (2007) IRX-2, a novel in vivo immunotherapeutic, induces maturation and activation of human dendritic cells in vitro. J Immunother 30:624–633. doi:10.1097/CJI.0b013e3180691593
Czystowska M, Han J, Szczepanski MJ, Szajnik M, Quadrini K, Brandwein H, Hadden JW, Signorelli K, Whiteside TL (2009) IRX-2, a novel immunotherapeutic, protects human T cells from tumor-induced cell death. Cell Death Differ 16:708–718. doi:10.1038/cdd.2008.197
Whiteside TL (2008) The tumor microenvironment and its role in promoting tumor growth. Oncogene 27:5904–5912. doi:10.1038/onc.2008.271
Bergmann C, Strauss L, Zeidler R, Lang S, Whiteside TL (2007) Expansion and characteristics of human T regulatory type 1 cells in co-cultures simulating tumor microenvironment. Cancer Immunol Immunother 56:1429–1442. doi:10.1007/s00262-007-0280-9
Heo DS, Snyderman C, Gollin SM, Pan S, Walker E, Deka R, Barnes EL, Johnson JT, Herberman RB, Whiteside TL (1989) Biology, cytogenetics, and sensitivity to immunological effector cells of new head and neck squamous cell carcinoma lines. Cancer Res 49:5167–5175
Bergmann C, Strauss L, Zeidler R, Lang S, Whiteside TL (2007) Expansion of human T regulatory type 1 cells in the microenvironment of cyclooxygenase 2 overexpressing head and neck squamous cell carcinoma. Cancer Res 67:8865–8873. doi:10.1158/0008-5472.CAN-07-0767
Zhou J, Paul WE (2009) Heterogeneity and plasticity of T helper cells. Cell Res 20:4–12. doi:10.1038/cr.2009.138
Ahmadzadeh M, Rosenberg SA (2006) IL-2 administration increases CD4+ CD25(hi) Foxp3+ regulatory T cells in cancer patients. Blood 107:2409–2414. doi:10.1182/blood-2005-06-2399
Strauss L, Bergmann C, Gooding W, Johnson JT, Whiteside TL (2007) The frequency and suppressor function of CD4+ CD25highFoxp3+ T cells in the circulation of patients with squamous cell carcinoma of the head and neck. Clin Cancer Res 13:6301–6311. doi:10.1158/1078-0432.CCR-07-1403
Bergmann C, Strauss L, Wang Y, Szczepanski MJ, Lang S, Johnson JT, Whiteside TL (2008) T regulatory type 1 cells in squamous cell carcinoma of the head and neck: mechanisms of suppression and expansion in advanced disease. Clin Cancer Res 14:3706–3715. doi:10.1158/1078-0432.CCR-07-5126
Alhamarneh O, Agada F, Madden L, Stafford N, Greenman J (2011) Serum IL10 and circulating CD4(+) CD25(high) regulatory T cell numbers as predictors of clinical outcome and survival in patients with head and neck squamous cell carcinoma. Head Neck 33:415–423. doi:10.1002/hed.21464
Sinicrope FA, Rego RL, Ansell SM, Knutson KL, Foster NR, Sargent DJ (2009) Intraepithelial effector (CD3+)/regulatory (FoxP3+) T-cell ratio predicts a clinical outcome of human colon carcinoma. Gastroenterology 137:1270–1279. doi:10.1053/j.gastro.2009.06.053
Salama P, Phillips M, Grieu F, Morris M, Zeps N, Joseph D, Platell C, Iacopetta B (2009) Tumor-infiltrating FOXP3+ T regulatory cells show strong prognostic significance in colorectal cancer. J Clin Oncol 27:186–192. doi:10.1200/JCO.2008.18.7229
Liotta F, Gacci M, Frosali F, Querci V, Vittori G, Lapini A, Santarlasci V, Serni S, Cosmi L, Maggi L et al (2011) Frequency of regulatory T cells in peripheral blood and in tumour-infiltrating lymphocytes correlates with poor prognosis in renal cell carcinoma. BJU Int 107(9):1500–1506. doi:10.1111/j.1464-410X.2010.09555.x
Shimizu K, Nakata M, Hirami Y, Yukawa T, Maeda A, Tanemoto K (2010) Tumor-infiltrating Foxp3+ regulatory T cells are correlated with cyclooxygenase-2 expression and are associated with recurrence in resected non-small cell lung cancer. J Thorac Oncol 5:585–590. doi:10.1097/JTO.0b013e3181d60fd7
Badoual C, Hans S, Rodriguez J, Peyrard S, Klein C, Agueznay Nel H, Mosseri V, Laccourreye O, Bruneval P, Fridman WH et al (2006) Prognostic value of tumor-infiltrating CD4+ T-cell subpopulations in head and neck cancers. Clin Cancer Res 12:465–472. doi:10.1158/1078-0432.CCR-05-1886
Strauss L, Whiteside TL, Knights A, Bergmann C, Knuth A, Zippelius A (2007) Selective survival of naturally occurring human CD4+CD25+Foxp3+ regulatory T cells cultured with rapamycin. J Immunol 178:320–329
Zeiser R, Leveson-Gower DB, Zambricki EA, Kambham N, Beilhack A, Loh J, Hou JZ, Negrin RS (2008) Differential impact of mammalian target of rapamycin inhibition on CD4+CD25+Foxp3+ regulatory T cells compared with conventional CD4+ T cells. Blood 111:453–462. doi:10.1182/blood-2007-06-094482
Haxhinasto S, Mathis D, Benoist C (2008) The AKT–mTOR axis regulates de novo differentiation of CD4+Foxp3+ cells. J Exp Med 205:565–574. doi:10.1084/jem.20071477
Crellin NK, Garcia RV, Levings MK (2007) Altered activation of AKT is required for the suppressive function of human CD4+CD25+ T regulatory cells. Blood 109:2014–2022. doi:10.1182/blood-2006-07-035279
Zhang Y, Apilado R, Coleman J, Ben-Sasson S, Tsang S, Hu-Li J, Paul WE, Huang H (2001) Interferon gamma stabilizes the T helper cell type 1 phenotype. J Exp Med 194:165–172
Wang Z, Hong J, Sun W, Xu G, Li N, Chen X, Liu A, Xu L, Sun B, Zhang JZ (2006) Role of IFN-gamma in induction of Foxp3 and conversion of CD4+ CD25- T cells to CD4+ Tregs. J Clin Invest 116:2434–2441. doi:10.1172/JCI25826
de Vivar R, Chavez A, de Vera ME, Liang X, Lotze MT (2009) The biology of interleukin-2 efficacy in the treatment of patients with renal cell carcinoma. Med Oncol 26(Suppl 1):3–12. doi:10.1007/s12032-008-9162-z
Malek TR, Bayer AL (2004) Tolerance, not immunity, crucially depends on IL-2. Nat Rev Immunol 4:665–674. doi:10.1038/nri1435
Burchill MA, Yang J, Vogtenhuber C, Blazar BR, Farrar MA (2007) IL-2 receptor beta-dependent STAT5 activation is required for the development of Foxp3+ regulatory T cells. J Immunol 178:280–290
Yao Z, Kanno Y, Kerenyi M, Stephens G, Durant L, Watford WT, Laurence A, Robinson GW, Shevach EM, Moriggl R et al (2007) Nonredundant roles for Stat5a/b in directly regulating Foxp3. Blood 109:4368–4375. doi:10.1182/blood-2006-11-055756
Franceschini D, Paroli M, Francavilla V, Videtta M, Morrone S, Labbadia G, Cerino A, Mondelli MU, Barnaba V (2009) PD-L1 negatively regulates CD4+CD25+Foxp3+ Tregs by limiting STAT-5 phosphorylation in patients chronically infected with HCV. J Clin Invest 119:551–564. doi:10.1172/JCI36604
Acknowledgments
This study was supported in part by National Institutes of Health (NIH) grant PO-1 CA 109688 to TLW. Support for BS was provided by IRX Therapeutics Inc.
Disclosures
All authors have read the manuscript and concur with its content. Dr. Schilling was supported by IRX Therapeutics Inc. Dr. Egan is employed by IRX Therapeutics Inc. The other co-authors do not have any financial/commercial conflict of interest that could be considered to have influenced the content of this paper.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Schilling, B., Harasymczuk, M., Schuler, P. et al. IRX-2, a novel biologic, favors the expansion of T effector over T regulatory cells in a human tumor microenvironment model. J Mol Med 90, 139–147 (2012). https://doi.org/10.1007/s00109-011-0813-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00109-011-0813-8