
Abstract
Aims/hypothesis
Our aim was to determine the incidence of Type 1 diabetes in children who were 0 to 14 years of age in Western Australia from 1985 to 2002, and to analyse the trends in incidence rate over the same period.
Methods
Primary case ascertainment was from a prospective population-based diabetes register that was established in 1987, and secondary case ascertainment was from the Western Australia Hospital Morbidity Data System. Denominator data were obtained from the Australian Bureau of Statistics. Poisson regression was used to analyse the incidence rates by calendar year, sex and age at diagnosis.
Results
There was a total of 1144 cases (560 boys, 584 girls). Using the capture–recapture method, case ascertainment was estimated to be 99.8% complete. The mean age standardised incidence from 1985 to 2002 was 16.5 per 100 000 person years (95% CI 14.7–18.2), ranging from 11.3 per 100 000 in 1985 to 23.2 per 100 000 in 2002. The incidence increased on average by 3.1% (95% CI 1.9%–4.2%) a year over the period (p<0.001). No significant difference was found between boys and girls. A significant increase in incidence was found in all age groups, with no disproportionate increase found in the 0 to 4-year-olds.
Conclusions/interpretation
The incidence of childhood-onset Type 1 diabetes in Western Australia has increased significantly over the past 18 years and shows no signs of abating. In contrast to other studies, a higher rate of increase was not found in the youngest children.
Similar content being viewed by others

Introduction
The changing epidemiology of childhood-onset Type 1 diabetes has been reported in many countries and remains unexplained. A significant increase in the incidence of Type 1 diabetes over the past few decades has been reported worldwide [1, 2, 3, 4]. More recently, several studies in Europe have found that the highest rate of increase is occurring in children younger than 5 years of age [5, 6, 7].
Worldwide, the incidence of childhood-onset Type 1 diabetes varies by more than 350-fold [8], ranging from 0.1 per 100 000 per year in China to 45 per 100 000 per year in Finland [9]. Epidemiological studies of Type 1 diabetes are important in identifying possible aetiological factors that might explain the large geographical variation and changing epidemiology of the disease.
Western Australia presents a unique opportunity to characterise every child diagnosed with Type 1 diabetes under the age of 15 years, enabling the epidemiology of childhood-onset Type 1 diabetes in this state to be described accurately.
Western Australia is the largest state in Australia with a land area of over 2.5 million square kilometres and an estimated population of 1.9 million. Aboriginal people account for 3.5% of the state’s total population [10] and the remainder are mainly people of European descent.
Princess Margaret Hospital for Children is the only tertiary paediatric hospital in the state and the only referral centre for children diagnosed with diabetes. In Australia, children with diabetes are usually treated by hospital-based paediatricians and endocrinologists. This enables case ascertainment levels of over 99% to be achieved consistently and the complete population-based data set can be used to describe the characteristics of newly diagnosed patients accurately.
The epidemiology of Type 1 diabetes in 0 to 14-year-olds in Western Australia has been described from 1985 to 1992, when it was found to have increased significantly in both sexes and across all age groups [11]. Therefore, the aims of this study were to determine the incidence of Type 1 diabetes in Western Australia in children who were 0 to 14 years of age from 1985 to 2002, and to analyse the trends in incidence rate over the same period.
Subjects and methods
The primary source of cases was the Western Australia Children’s Diabetes database, which was established at Princess Margaret Hospital in 1987 [12]. This prospective population-based register satisfies the criteria of the Diabetes Epidemiology International Group [13], enabling an international comparison of incidence rates. The database also contains retrospective data, obtained using multiple sources, on children diagnosed with Type 1 diabetes from 1985 to 1987. All patients seen at Princess Margaret Hospital with newly diagnosed Type 1 diabetes are registered on the database. As Princess Margaret Hospital is the only referral centre for children diagnosed with diabetes in Western Australia, the case ascertainment level of this database is over 99% [11, 12].
Data collected include name, date of birth, date of diagnosis, age at diagnosis, sex, address at diagnosis, results from autoantibody assays and family history. Patients are seen every 3 months at the diabetes clinic, and the database is updated regularly with results from investigations. Therefore, the records of any patients found to have been diagnosed incorrectly with Type 1 diabetes, or to have diabetes secondary to other causes, are changed to include this information.
Secondary case ascertainment was from the Western Australian Hospital Morbidity Data System, which contains name-identified information on discharges from all public and private sector acute-care hospitals in the state. A list of all patients whose diagnosis at discharge included any reference to Type 1 diabetes, and whose age at admission was less than 15 years, was obtained and then cross-checked with cases in the diabetes database. The capture-recapture method was used to estimate completeness of ascertainment [14].
All patients diagnosed with Type 1 diabetes by a physician and who started insulin therapy before the age of 15 years and were resident in Western Australia at the time of diagnosis were included in the study. Patients with diabetes secondary to other causes, such as cystic fibrosis, were excluded. Type 1 diabetes was diagnosed according to the definition of the World Health Organization [15] and the date of diagnosis was defined as the date when insulin therapy was initiated.
Population estimates based on census data were obtained from the Australian Bureau of Statistics.
Ethics approval for this study was obtained from the Princess Margaret Hospital Ethics Committee and the Western Australia Department of Health’s Confidentiality of Health Information Committee. Informed consent was obtained from all patients prior to their data being stored on the diabetes database at Princess Margaret Hospital.
Statistical analysis
Incidence rates were calculated using cases from both sources as the numerator and annual population estimates from the Australian Bureau of Statistics as the denominator [16, 17]. Age-standardised rates were calculated using the direct method with the developed world population, which has equal numbers in each subgroup defined by age (0–4, 5–9 and 10–14 years) and sex, as the standard [18]. Confidence intervals were estimated assuming a Poisson distribution of cases.
Poisson regression models were used to analyse the incidence rates by calendar year, sex and age group at diagnosis (0–4, 5–9 and 10–14 years), and to estimate the temporal trends. Models were fitted to test for differences in the incidence rate trends between the sexes and between the three age groups.
To analyse the incidence for seasonal variation, sine and cosine functions in a logistic regression analysis were used [19]. This method also allows for covariate adjustment.
Annual incidence rates were calculated from 1985 to 2002. The rates calculated from 1985 to 1992 were found to be almost identical to those previously published [11]. However, for consistency, we present the most recently obtained data to analyse the incidence rate trends over the study period.
A p value of less than 0.05 was considered statistically significant. Data were analysed by using the STATA statistical software package (version 8.0, Stata Corporation, College Station, Tex., USA).
Results
Ascertainment.
From 1985 to 2002, there was a total of 1144 cases (560 boys, 584 girls). Case ascertainment for 1985 to 1992 has been estimated as 99.6% [11]. From 1992 to 2002, of the 801 cases in total, 786 were ascertained from both the register at Princess Margaret Hospital and the Hospital Morbidity Data System, ten cases were ascertained only from the Hospital Morbidity Data System and 15 cases were ascertained only from the register at Princess Margaret Hospital. Using the capture–recapture method, the case ascertainment from 1992 to 2002 was estimated to be 99.98%. Therefore, the case ascertainment for the whole study period was estimated to be 99.8% complete.
Overall incidence
The mean age standardised incidence rate from 1985 to 2002 was 16.5 per 100 000 person years (95% CI: 14.7–18.2). The incidence ranged from 11.3 per 100 000 person years in 1985, to 23.2 per 100 000 person years in 2002 (Fig. 1). The incidence has increased significantly (p<0.001) by an average of 3.1% (95% CI: 1.9%–4.2%) a year since 1985.

The trend in the incidence of Type 1 diabetes in 0 to 14-year-olds in Western Australia from 1985 to 2002. Solid line and filled symbols: annual age-standardised incidence (error bars show 95% CI); dotted line: estimated trend
Sex
From 1985 to 2002, the mean age-standardised incidence was 15.6 per 100 000 person years (95% CI: 13.7–17.5) in boys and 17.3 per 100 000 person years (95% CI: 15.3–19.4) in girls. The incidence has increased significantly in both sexes, with an average annual increase of 3.9% (95% CI: 2.2%–5.6%, p<0.001) in boys and 2.3% (95% CI: 0.6%–3.9%, p=0.005) in girls. There was no significant difference between the age-standardised incidence (incidence rate ratio = 1.10, 95% CI: 0.98–1.24, p=0.10) or incidence rate trends in boys compared with girls (p=0.18).
Age group
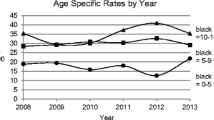
The mean incidence in 0 to 4-year-olds, from 1985 to 2002, was 11.0 per 100 000 person years (95% CI: 9.2–12.8). This was significantly lower than the mean incidence in 5 to 9 and 10 to 14-year-olds (Table 1). There was no significant difference between the overall incidence of 18.8 per 100 000 person years (95% CI: 16.3–21.3) in 5 to 9-year-olds and 19.6 per 100 000 person years in (95% CI: 17.6–21.6) in 10 to 14-year-olds. The incidence has increased significantly in all age groups since 1985 (Fig. 2). The incidence increased by an average of 3.3% a year (95% CI: 0.9%–5.9%) in 0 to 4-year-olds, 3.7% a year (95% CI: 1.8%–5.7%) in 5 to 9-year-olds and 2.2% a year (95% CI: 0.4%–4.0%) in 10 to 14-year-olds. There was no significant difference in the incidence rate trends between the age groups, and a disproportionate rate of increase in the youngest age group was not found.

Trends in the age-specific annual incidence of Type 1 diabetes in 0 to 14-year-olds in Western Australia from 1985 to 2002. Observed rates in 0 to 4-year-olds (circles), 5 to 9-year-olds (squares), 10 to 14-year-olds (triangles) and estimated trends (dotted lines)
Seasonal variation
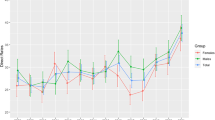
There was significant seasonal variation in the incidence of Type 1 diabetes. A seasonal pattern with one maximum and one minimum level per year was highly significant (p<0.001). A higher number of cases was diagnosed from April to September, the autumn and winter months in Australia (Fig. 3). A non-significant pattern was found when investigating two minimum and maximum levels per year (p=0.398). There was no significant effect of sex (p=0.098); however, there was a highly significant effect of age (p<0.001). When analysing the individual age groups, a significant seasonal pattern was only found in the 0 to 4-year-olds (p=0.046).

Seasonal variation in incidence of Type 1 diabetes in 0 to 14-year-olds in Western Australia
Discussion
The incidence of childhood-onset Type 1 diabetes in Western Australia is increasing at a rate comparable to that reported in another state of Australia, New South Wales [20], and in many European countries (3.2% a year) [2, 3]. This increase in incidence cannot be explained by increased ascertainment levels as the completeness of the population-based diabetes database in Western Australia has been estimated to be over 99% since its establishment in 1987, and case ascertainment methods have remained unchanged since that time.
The overall incidence in Western Australia is similar to that in New South Wales [20] and it is in the high-incidence category compared to other countries [8].
There has been a significant increase in the incidence in both boys and girls. No significant difference was found in the overall incidence or incidence rate trends in boys compared with girls. There are inconsistent findings on the difference in incidence of Type 1 diabetes by sex. In general, a male excess has been found in countries with a high incidence and a female excess in countries with a low incidence of Type 1 diabetes [18, 21, 22]. However, a higher incidence in girls was recently reported in New South Wales [20] and similar to our findings, some studies have found no difference in incidence between boys and girls [23, 24], although both these studies had ascertainment levels of 85%.
Many studies report an increase in incidence with increasing age, with the highest incidence occurring in the 10 to 14-year-old age group [8]. In this study, the incidence of Type 1 diabetes in the youngest age group was found to be significantly lower than that in 5 to 9 and 10 to 14- year-olds. However, there was no significant difference in the incidence between 5 to 9 and 10 to 14-year-olds.
In contrast to reports from Europe [2], Oxford, UK [5] and Finland [6], in which higher rates of increase in the youngest age group have been documented, a disproportionate rate of increase in 0 to 4-year-olds was not found in Western Australia. There was no significant difference in the incidence rate trends between the age groups, which is similar to the findings in other countries, including Scotland [25, 26]. Although a trend towards a higher rate of increase in the youngest age group was found in New South Wales, no statistically significant difference was found in the trend between the age groups.
Significant seasonal variation in incidence was found with a higher number of cases being diagnosed in the autumn and winter months. This is consistent with the findings from many studies that have found a lower incidence of Type 1 diabetes occurring in the warmer months [3]. Studies examining seasonal variation by sex and age group have not had consistent findings. Some studies have found significant seasonal variation occurring only in boys [27] and varying with age, with some studies showing a seasonal effect in all age groups [3] and others, only in 10 to 14-year-olds [28]. Seasonal variation in incidence may reflect the role of environmental factors such as increased exposure to infections, lower physical activity and dietary intake in the aetiology of Type 1 diabetes.
The rapid increase in incidence of Type 1 diabetes around the world is likely to be the result of increased exposure to environmental risk factors in genetically susceptible individuals. The non-differential increase in incidence in both sexes and all age groups, found in Western Australia, suggests that the increased exposure to risk factors affects all of these groups.
The 18 years of complete population-based data on incident cases of Type 1 diabetes in Western Australia mean that our results are an accurate description of the epidemiology of Type 1 diabetes in this state. Continued monitoring of the incidence of diabetes in Western Australia should increase our understanding of the global patterns of this disease and help generate hypotheses concerning potential aetiological factors.
References
Onkamo P, Vaananen S, Karvonen M, Tuomilehto J (1999) Worldwide increase in incidence of Type 1 diabetes—the analysis of the data on published incidence trends. Diabetologia 42:1395–1403
EURODIAB ACE Study Group (2000) Variation and trends in incidence of childhood diabetes in Europe. Lancet 355:873–876
Green A, Patterson C, on behalf of the EURODIAB TIGER Study Group (2001) Trends in the incidence of childhood-onset diabetes in Europe 1989–1998. Diabetologia 44 [Suppl 3]:B3–B8
Gale EA (2002) The rise of childhood type 1 diabetes in the 20th century. Diabetes 51:3353–3361
Gardner SG, Bingley PJ, Sawtell PA, Weeks S, Gale EA, the Bart’s-Oxford Study Group (1997) Rising incidence of insulin dependent diabetes in children aged under 5 years in the Oxford region: time trend analysis. BMJ 315:713–717
Karvonen M, Pitkaniemi J, Tuomilehto J, The Finnish Childhood Type 1 Diabetes Registry Group (1999) The onset of Type 1 diabetes in Finnish children has become younger. Diabetes Care 22:1066–1070
Schoenle E, Lang-Muritano M, Gschwend S et al. (2001) Epidemiology of type 1 diabetes mellitus in Switzerland: steep rise in incidence in under 5 year old children in the past decade. Diabetologia 44:286–289
Karvonen M, Viik-Kajander M, Moltchanova E et al. (2000) Incidence of childhood type 1 diabetes worldwide. Diabetes Care 23:1516–1526
Tuomilehto J, Karvonen M, Pitkaniemi J et al. (1999) Record-high incidence of type 1 (insulin-dependent) diabetes mellitus in Finnish children. Diabetologia 42:655–660
Epidemiology Branch, HIC, Department of Health, Gov WA (2002) Population characteristics of residents of the State of Western Australia
Kelly HA, Russell MT, Jones TW, Byrne GC (1994) Dramatic increase in incidence of insulin dependent diabetes mellitus in Western Australia. Med J Aust 161:426–429
Kelly HA, Byrne GC (1992) Incidence of IDDM in Western Australia in children aged 0–14 yr from 1985 to 1989. Diabetes Care 15:515–517
LaPorte R, Tajima N, Akerblom H et al. (1985) Geographic differences in the risk of insulin-dependent diabetes mellitus: the importance of registries. Diabetes Care 8 [Suppl 1]:101–107
LaPorte R, McCarty D, Bruno G, Tajima N, Baba S (1993) Counting diabetes in the next millenium: application of capture-recapture technology. Diabetes Care 16:528–534
World Health Organization Department of Noncommunicable Disease Surveillance Geneva (1999) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus. Report of a WHO consultation. (http://www.who.int/ncd/dia/dia_publications.htm-accessed Dec 2003)
Australian Bureau of Statistics (1985–2001) Estimated resident population by age and sex in statistical local areas, Western Australia. Australian Government Publishing Service, Canberra, Catalog No. 3203.5
Australian Bureau of Statistics (2002) Population by age and sex, Western Australia. Australian Government Publishing Service, Canberra, Catalog No. 3235.5
Rewers M, LaPorte R, King H, Toumilheto J (1988) Trends in the prevalence and incidence of diabetes: insulin-dependent diabetes mellitus in childhood. World Health Stat Q 41:179–189
Stolwijk AM, Straatman H, Zielhuis GA (1999) Studying seasonality using sine and cosine functions in regression analysis. J Epidemiol Community Health 53:235–238
Craig M, Howard N, Silink M, Chan A (2000) The rising incidence of childhood type 1 diabetes in New South Wales, Australia. J Pediatr Endocrinol Metab 13:363–372
Karvonen M, Pitkaniemi M, Pitkaniemi J et al. (1997) Sex difference in the incidence of insulin-dependent diabetes mellitus: an analysis of the recent epidemiological data. Diabetes Metab Rev 13:275–291
Green A, Gale EA, Patterson C, for the EURODIAB ACE Study Group (1992) Incidence of childhood-onset insulin-dependent diabetes mellitus: the EURODIAB ACE study. Lancet 339:905–909
Toth E, Lee K, Couch R, Martin L (1997) High incidence of IDDM over 6 years in Edmonton, Alberta, Canada. Diabetes Care 20:311–313
Sebastiani L, Visalli N, Adorisio E et al. (1996) A 5-year (1989–1993) prospective study of the incidence of IDDM in Rome and the Lazio region in the age-group 0–14 years. Diabetes Care 19:70–73
Diabetes Epidemiology Research International Group (1990) Secular trends in incidence of childhood IDDM in 10 countries. Diabetes 39:858–864
Rangasami JJ, Greenwood DC, McSporran B, Smail PJ, Patterson CC, Waugh NR (1997) Rising incidence of type 1 diabetes in Scottish children, 1984–93. Arch Dis Child 77:210–213
Karvonen M, Tuomilehto J, Virtala E et al. (1996) Seasonality in the clinical onset of insulin-dependent diabetes mellitus in Finnish children. Am J Epidemiol 143:167–176
Verge C, Silink M, Howard N (1994) The incidence of childhood IDDM in New South Wales, Australia. Diabetes Care 17:693–696
Acknowledgements
We wish to thank Dr Jim Codde (Epidemiology Branch, Department of Health, Western Australia) for his invaluable advice and Dr Mark S. Pearce (School of Clinical Medical Sciences, University of Newcastle, England) for his advice on seasonality.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Haynes, A., Bower, C., Bulsara, M.K. et al. Continued increase in the incidence of childhood Type 1 diabetes in a population-based Australian sample (1985–2002). Diabetologia 47, 866–870 (2004). https://doi.org/10.1007/s00125-004-1385-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-004-1385-8