
Abstract
Objective
To compare the safety and estimate the response profile of olanzapine, a second-generation antipsychotic, to haloperidol in the treatment of delirium in the critical care setting.
Design
Prospective randomized trial
Setting
Tertiary care university affiliated critical care unit.
Patients
All admissions to a medical and surgical intensive care unit with a diagnosis of delirium.
Interventions
Patients were randomized to receive either enteral olanzapine or haloperidol.
Measurements
Patient’s delirium severity and benzodiazepine use were monitored over 5 days after the diagnosis of delirium.
Main results
Delirium Index decreased over time in both groups, as did the administered dose of benzodiazepines. Clinical improvement was similar in both treatment arms. No side effects were noted in the olanzapine group, whereas the use of haloperidol was associated with extrapyramidal side effects.
Conclusions
Olanzapine is a safe alternative to haloperidol in delirious critical care patients, and may be of particular interest in patients in whom haloperidol is contraindicated.
Similar content being viewed by others


Introduction
Delirium in the intensive care unit (ICU) setting has generated interest recently. Its occurrence is associated with adverse outcomes: self-extubation, removal of indwelling catheters [1], prolonged ventilator dependence [2], and lengthened ICU and hospital stay [3, 4, 5]. Delirium is not associated with increased ICU mortality [1, 2] but seems an independent marker for increased 1-year mortality [6]. Recognizing delirium remains challenging [7, 8]. Recent tools have been developed to screen for [9] and aid in identification of [10] delirium in the ICU. Clinical management and pharmacologic treatment of delirium remain unexplored.
Published recommendations for delirium treatment in the ICU are empiric. Antipsychotic administration is broadly accepted, especially for agitated delirium [11]. The use of antipsychotics is based on the belief that such intervention will shorten symptom severity and duration [12]. Haloperidol is the medication most commonly used in critical care practice. Intravenous administration presumes that this route is more effective in emergency situations, with less extrapyramidal side effects [13]. This approach, with rapid dose escalation, is specifically recommended in textbooks [14] and recently published guidelines [15].
Despite its broad acceptance in clinical practice, haloperidol is not without adverse effects. Cognitive “numbness” and dysphoria are well recognized and occur in 40% of studied subjects [16]. Extrapyramidal side effects, such as akathisia and oropharyngeal dysfunction, have been described [16, 17]. Neuroleptic malignant syndrome and dystonic reactions, including laryngospasm and trismus, are also reported [18, 19].
Haloperidol causes ventricular arrhythmias, torsades de pointe, and cardiac arrest, especially in patients with cardiac disease both with and without preceding QT interval prolongation [20]. QT prolongation has been reported with low-dose haloperidol. Finally, some patients may be resistant to haloperidol. All patients thus require ongoing assessment of its therapeutic effect [21].
The severity of comorbid conditions commonly observed in the ICU raises concerns about haloperidol’s potential adverse effects. In some patients haloperidol is clearly contraindicated. An alternative medication which offers symptomatic control of delirium with less frequent and less severe adverse effects would be clinically useful in the delirious ICU patient. New second-generation antipsychotics with more favorable pharmacologic profiles have been introduced for the treatment of schizophrenia. Their potential benefit in delirium treatment has recently been explored [22, 23, 24, 25, 26]; one of these, olanzapine, has a reported oral bioavailability of 80% and no active metabolites [27].
Because of early encouraging reports [22, 23, 24, 25, 26], we conducted a prospective randomized controlled trial to evaluate the safety and clinical utility of one such agent, olanzapine, as an alternative to haloperidol for treatment of delirium in the intensive care setting.
Materials and methods
Subjects
From July 2000 to September 2001, patients aged 18–75 years admitted to a 16-bed medical-surgical ICU (Maisonneuve-Rosemont Hospital, Montreal,) for more than 24 h were screened three times daily for delirium utilizing the ICU Delirium Screening Checklist, ICU-DSC, as previously described [9]. In screened patients with an ICU DSC of ≥4 or with clinical manifestations delirium, the diagnosis was confirmed by a physician using DSM-IV criteria [28]. All patients with delirium were considered eligible for the study.
Pregnant patients, those who received antipsychotic medication within 10 days prior to hospital or ICU admission, or in whom either haloperidol or olanzapine was contraindicated were excluded. Contraindications to drug administration were Parkinson’s disease, oropharyngeal dysfunction, prolonged QT interval, and hepatic or renal dysfunction.
Individuals with gastrointestinal dysfunction, precluding oral/enteral drug administration, or whose neurological status did not permit an adequate neuropsychiatric evaluation (e.g., stupor or coma), were also excluded from the study. Patients who developed agitation during the study were permitted intravenous haloperidol administration (recorded as “rescue haloperidol”).
The research protocol was approved by the institutional scientific and ethics committee. Written informed consent as well as agreement from the attending physician were obtained prior to study enrollment.
Interventions
After randomization on an even/odd day basis for haloperidol or olanzapine, the intensivist prescribed the antipsychotic orally or via enteral tube within 2 h of the diagnosis of delirium. Haloperidol was initiated at 2.5–5 mg every 8 h, and olanzapine was begun at 5 mg daily. Patients over 60 years received a lower initial dosage (haloperidol 0.5–1 mg, or olanzapine 2.5 mg). Subsequent titration was based on clinical judgment. All administered doses of medication were recorded. We noted the use of benzodiazepines as adjuvant treatment. Clinicians and nurses titrated sedative dosage with the Ramsay scale. Intravenous haloperidol administration was left to the treating intensivist’s discretion.
Study measures
Demographic information, type of admission, and Acute Physiology and Chronic Health Evaluation (APACHE II) scores were collected when delirium was diagnosed. Objective evaluations were performed on a daily basis by a clinician or research nurse blinded to the dispensed medication. The measures obtained at baseline and daily up to a maximum of 5 days in the ICU were:
-
1.
Vital signs.
-
2.
Liver function tests.
-
3.
Daily dose of antipsychotic study medication.
-
4.
Daily dose “rescue haloperidol.”
-
5.
Daily dose of sedatives if used specifically for sedation. Benzodiazepines doses were converted to lorazepam equivalents [29].
-
6.
Daily dose of antiparkinsonian medication prescribed for extrapyramidal side effects.
-
7.
Delirium index (DI), as previously described [30], administered by one of three individuals (two research nurses, one physician) trained its use. This delirium severity scale is based on seven items associated with delirium, each rated on a four-point scale for a maximum score of 21. The evaluator was blinded to the patient’s treatment.
-
8.
Daily worst Ramsay score [31] obtained at least once every 8-h shift.
-
9.
Extrapyramidal signs assessed with Ross-Chouinard [32] and Angus-Simpson scales [33] by a physician.
Statistics
Comparisons of medical and demographic characteristics were performed with Fisher’s exact test and Student’s t test. Analysis of variance for repeated measures was used for group comparisons on the DI severity scores, and total daily benzodiazepine dose, based on a 2×5 mixed model, (i.e., two groups measured at five time points). When indicated, Greenhouse-Geisser correction was applied to adjust for unstable between-measures correlation. All simple main effects were calculated, in order to assess group differences at each time point and study patterns of change within each of the two groups. Sidaks multiple comparisons procedure was used for post-hoc time-point comparisons.
Inter-rater reliability was evaluated with the intra-class correlation coefficient, using a two-way random-effects model. Since delirium is a fluctuating disorder, intra-rater reliability was not tested.
Results
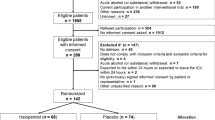
Of 1009 patients admitted to the ICU during the study period, 214 patients were diagnosed with delirium. Of those, 103 were considered eligible for the study (exclusions were due primarily to gastrointestinal dysfunction). Informed consent was obtained in 80 patients; of these, the treating physician withdrew 3 patients, status changed to “no active treatment” in 2, drug interaction was suspected in 1, and data was lost in 1 patient. Seventy-three patients were included in the final analysis. Sixty-one patients remained alive and in the hospital for 3 days or more, accounting for the difference between the randomized and 3-day analysis. Patient characteristics are shown in Table 1. Gender distribution (p=0.43) and APACHE II scores (p=0.14) were comparable, as were patient weights (p=0.9). The study population was predominantly surgical. The difference between the urgent/elective surgical patient ratio did not reach statistical significance (p=0.057). The mean age of patients receiving haloperidol (63.26±11.66 years) was lower than the age of the group receiving olanzapine (67.50±6.04 years, p=0.046). Other clinical characteristics related to reasons for ICU admission, as well as co-morbidities, were no different between the groups.
Patients in the haloperidol group received were given a mean enteral daily dose of 6.5 mg of drug (range 1–28 mg) compared with 4.54 mg for the olanzapine group (range 2.5–13.5 mg). Rescue intravenous haloperidol was used primarily on the first day (10 of 28 in the olanzapine group, range 1–5 mg, 2.32±1.32 mg; vs 19 of 45 in the haloperidol group, range 1–5 mg, 2.92±1.56 mg). From day 2 onwards, 5 patients received rescue haloperidol in doses ranging from 1 to 3 mg. Only one olanzapine patient required one rescue haloperidol dose on day 3. The proportion of patients requiring intravenous haloperidol (p=0.63) and the amount of IV haloperidol required in each group (Z=0.97, p=0.35) were similar.
The results of the daily DI scores are summarized in Fig. 1. A comparable reduction in DI was noted over time in both groups, with no difference between patients treated with haloperidol vs olanzapine (ANOVA time effect p=0.02, group effect p=0.83, interaction effect p=0.64). Inclusion of patients present for only 3 or 4 days did not modify the results. Overall agreement between observers regarding the DI score was excellent (CCI=0.96).

Delirium index scores were performed daily and are shown over time. Overall delirium indices decreased over time (7.08 for all patients on day 1 decreasing to 5.05 on day 5). There are no differences between the two groups
Figure 2 depicts the benzodiazepine dose requirements over time, expressed in lorazepam equivalents [29]. The square root of benzodiazepine doses was used to correct for non-normal distributions as well as the withdrawal of one subject (no. 64) from the analysis because benzodiazepine values on days 4 and 5 were atypical (24 and 26 mg, respectively). Analysis of variance did not identify any differences between the two groups, at any of the five measurement times (interaction effect p=0.94, group effect p=0.9). There was, however, a time effect (p=0.02) reflecting the decrease in dosages required over time in both groups.

Benzodiazepine mean daily dose doses were calculated per 24 h per patient and are shown over time. There are no differences between the groups
The dose of rescue haloperidol, opiates, sedatives other than benzodiazepines, Ramsay scores, vital signs, and liver function tests were no different between groups. Most patients received continuous infusions of fentanyl, the preferred opiate analgesic in our ICU, in doses ranging from 50 to 100 μg/h. Propofol was not used. Ramsay scores ranged from 1 to 3 in both groups with the exception of the first 24 h, during which approximately a third of the patients, evenly distributed among the groups, had mild agitation. Extrapyramidal symptoms were carefully recorded. Among the patients receiving haloperidol, 6 rated low scores on extrapyramidal symptom testing (1 for the Ross Chouinard, 1–4 for the Simpson-Angus scale). Patients on olanzapine had no extrapyramidal manifestations. No patient in either group received prophylactic or therapeutic antiparkinsonian therapy. There were no adverse effects (specific or otherwise) attributable to olanzapine.
Discussion
Management of delirium in ICU patients whose co-morbidities render the physician reluctant to administer haloperidol can be problematic. Recent studies have explored the safety and efficacy of novel antipsychotics in the management of delirium outside the ICU [22, 23, 24, 25, 26].
We compared enteral haloperidol and olanzapine, in consecutively admitted eligible ICU patients with delirium. The DI, a tool specifically designed to measure changes in the severity of the symptoms of delirium, was chosen because it was easy to perform in an intensive care setting (in contrast to the widely used Delirium Rating Scale or the Memorial Delirium Assessment Scale). Both olanzapine and haloperidol were effective in reducing delirium symptoms. The clinical course in both treatment arms was unmarred by severe agitation. Olanzapine patients had no adverse effects attributable to the drug, whereas 6 patients receiving haloperidol developed extrapyramidal signs.
Intravenous (IV) administration of haloperidol has gained acceptability in the ICU based on a single, unblinded, non-randomized study in which IV administration produced fewer extrapyramidal side effects (compared with enteral haloperidol) in 10 patients [13]. Although clinical experience and textbook recommendations have resulted in the universal use of intravenous haloperidol in this setting, few authors mention its drawbacks and potential for therapeutic failure [34, 35]. Enteral haloperidol was compared with olanzapine because olanzapine was not available in parenteral form; we wished to exclude differences attributable to administration route. Bioavailability of either drug may have been slow as a result, although absorption or bioavailability should have been similar for the two medications. This is indirectly supported by the fact that neither measures of clinical outcomes nor the use of rescue or adjunctive medication differed between the two treatment arms. Despite unreliable systemic absorption of enteral medications in the critical care setting, correction of a “low cholinergic excess dopaminergic state” (one of the mechanisms by which antipsychotics are felt to affect delirium) may have occurred with relatively low dose of either antipsychotic [36].
Intravenous rescue haloperidol, used in the first 24 h in both groups, may have contaminated the early DI evaluation between the groups. Given the reported half-life of intravenous haloperidol, however, and the small number of patients who required it beyond the first day, it is unlikely the overall beneficial evolution of the olanzapine group over time is attributable to the rescue haloperidol received on the first day.
The population studied included a greater proportion of surgical than medical patients. Surgical vs medical disease is not recognized [1] as influencing the incidence or severity of delirium.
Delirium subtypes [8, 37] were not explicitly described because of previous work suggesting that “quiet,” non-agitated delirium is just as morbid as delirium accompanied by agitation [1]. Independently, agitation in the ICU may be ascribed to a number of factors other than delirium. The ICU in which the study was performed has a clinical expertise in delirium screening. This may account for the low delirium scores on diagnosis and throughout the study. No patients were identified with severe initial psychomotor agitation and delirium requiring immediate intravenous haloperidol administration prior to study entry. Patients seldom reach this state in our unit, we believe, because of systematic screening for thought content as part of an ICU Delirium Screening Checklist [9] which is used routinely in all patients. The relatively low daily dose of benzodiazepines utilized further support this hypothesis. Almost all patients also received opiate analgesics, which may have decreased the overall use of anxiolytics such as benzodiazepines.
This study’s main limitation is the uneven distribution between the two treatment groups. Drug allocation sequences should ideally be completely random and concealed. The odd/even day randomization, chosen for convenience, was not corrected for the slightly more frequent occurrence of odd days on which patients were randomized to receive haloperidol in this study. Although not explicit, the research nurse’s or physician’s randomization based on odd/even days may have inadvertently led to bias on their part, or on the part of the treating team who may have guessed the randomization sequence. The treating physicians and nurses were not blinded to the assigned drug. Reporting bias (with regard to the day delirium developed) may have influenced subsequent administration of the study or other medications.
Haloperidol and olanzapine dosages were within ranges described for treating delirium in other settings [24, 25, 26]. The severity of delirium and the clinical response suggested a 20–30% drop in DI ratings with sizeable standard deviation variability, precluding comparative statements about the therapeutic effectiveness of either medication.
Olanzapine seems a safe alternative to haloperidol for the treatment of acute delirium in ICU patients. Although the small sample size limits the statistical evaluation of side effects between groups, few adverse effects were noted in either group. The absence of extrapyramidal side effects in the olanzapine group is in keeping with the findings described by Breitbart et al. [26], and in favor of its use in ICU patients. Cardiac toxicity, including arrhythmias and QT prolongation, have not been described with olanzapine. Olanzapine is costlier than haloperidol; however, in view of the comparable efficacy in reducing delirium symptoms, olanzapine can perhaps be recommended for patients in whom cardiac disease, QT prolongation, or other features preclude haloperidol use.
This represents the first prospective randomized study of antipsychotic treatment for delirium in an ICU. The issue warrants further exploration in delirious ICU patients with higher APACHE scores. The availability of olanzapine in parenteral form may broaden its applicability. This preliminary work suggests olanzapine is safe and effective in reducing delirium symptoms.
Conclusion
In ICU delirium, olanzapine is a treatment alternative to haloperidol. Its use could benefit patients with underlying Parkinson’s disease, a prolonged QT interval, or oropharyngeal dysfunction, which preclude the safe administration of haloperidol. Its recommendation as treatment for delirium in the critical care setting is limited by its current availability only in enteral form.
References
Dubois MJ, Bergeron N, Dumont M, Dial S, Skrobik Y (2001) Delirium in an intensive care unit: a study of risk factors. Intensive Care Med 27:1297–1304
Dial S, Payne J (2002) Managing delirium in the intensive care unit. Clin Pulm Med 9:260–266
Kishi Y, Iwasaki Y, Takezawa K, Kurosawa H, Endo S (1995) Delirium in critical care unit patients admitted through an emergency room. Gen Hosp Psychiatry 17:371–379
Aldemir M, Ôzen S, Hara IH, Sir A, Baç B (2001) Predisposing factors for delirium in the surgical intensive care unit. Crit Care 5:265–270
Ely EW, Guatam S, Margolin R, Francis J, May L, Speroff T, Truman B, Dittus R, Bernard GR, Inouye SK (2001) The impact of delirium in the intensive care unit on hospital length of stay. Intensive Care Med 27:1892–1900
McCusker J, Cole M, Abrahamowicz M, Primeau F, Belzile E (2002) Delirium predicts 12-month mortality. Arch Intern Med 162:457–463
McGuire BE, Basten CJ, Ryan CJ, Gallagher J (2000) Intensive care unit syndrome: a dangerous misnomer. Arch Intern Med 160:906–909
Armstrong SC, Cozza KL, Watanabe KS (1997) The misdiagnosis of delirium. Psychosomatics 38:433–439
Bergeron N, Dubois MJ, Dumont M, Dial S, Skrobik Y (2001) Intensive care delirium screening checklist: evaluation of a new screening tool. Intensive Care Med 27:859–864
Ely EW, Inouye SK, Bernard GR, Gordon S, Francis J, May L, Truman B, Speroff T, Gautam S, Margolin R, Hart RP, Dittus R (2001) Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). J Am Med Assoc 286:2703–2710
American Psychiatric Association (1999) Practice guideline for the treatment of patients with delirium. Am J Psychiatry 156:1–20
Breitbart W, Gibson C, Tremblay A (2002) The delirium experience: delirium recall and delirium-related distress in hospitalized patients with cancer—their spouses/caregivers, and their nurses. Psychosomatics 43:183–194
Menza MA, Murray GB, Holmes VF, Rafuls WA (1987) Decreased extrapyramidal symptoms with intravenous haldol. J Clin Psychiatry 48:278–280
Wise MG, Cassem NH (1998) Behavioural disturbances in the ICU. In: Civetta JM, Taylor RW, Kirby RR (eds) Critical care. Lippincott, Philadelphia, pp 1595–1604
Jacobi J, Fraser GL, Coursin DB, Riker RR, Fontaine D, Wittbrodt ET, Chalfin DB, Masica MF, Bjerke S, Coplin WM, Crippen DW, Fuchs BD, Kelleher RM, Marik PE, Nasraway SA, Murray MJ, Peruzzi WT, Lumb PD (2002) Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med 30:119–141
King DJ, Burke M, Lucas RA (1995) Antipsychotic drug-induced dysphoria. Br J Psychiatry 167:480–482
Bashford G, Bradd P (1996) Drug-induced Parkinsonism associated with dysphagia and aspiration: a brief report. J Geriatr Psychiatry Neurol 9:133
Caroff SN, Mann SC, Campbell EC (2001) Neuroleptic malignant syndrome. Adverse drug reaction bulletin, no. 209. Lippincott, Williams and Wilkins, London, pp 799–802
Ilchef R (1997) Neuroleptic-induced laryngeal dystonia can mimic anaphylaxis. Aust N Z J Psychiatry 31:877–879
Perrault LP, Denault AY, Carrier M, Cartier R, Belisle S (2000) Torsades de pointes secondary to intravenous haloperidol after coronary bypass surgery. Can J Anesth 47:251–254
Kapur S, Remington G, Jones C, Wilson A, DaSilva J, Houle S, Zipursky R (1996) High levels of dopamine D2 receptor occupancy with low-dose haloperidol treatment: a PET study. Am J Psychiatry 153:948–950
Sipahimalani A, Masand PS (1997) Use of risperidone in delirium: case reports. Ann Clin Psychiatry 9:105–107
Sipahimalani A, Sime RM, Masand PS (1997) Treatment of delirium with risperidone. Int J Geriatr Psychopharmacol 1:24–26
Sipahimalani A, Masand PS (1998) Olanzapine in the treatment of delirium. Psychosomatics 39:422–430
Kim K, Pae C, Chae J, Bahk W, Jun T (2001) An open pilot trial of olanzapine for delirium in the Korean population. Psychiatr Clin Neurosci 55:515–519
Breitbart W, Tremblay A, Gibson C (2002) An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics 43:175–182
Markowitz JS, Brown CS, Moore TR (1999) Atypical antipsychotics. Part I: Pharmacology, pharmacokinetics, and efficacy. Ann Pharmacother 33:73–85
American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders, 4th edn (DSM-IV). American Psychiatric Association, Washington, DC
Cammarano WB, Drasner K, Katz J (1998) Pain control, sedation, and use of muscle relaxants. In: Hall JB, Schmidt GA, Wood LD, (eds) Principles of critical care medicine. McGraw Hill, New York, pp 90–97
McCusker J, Cole M, Bellavance F, Primeau F (1998) Delirium: reliability and validity of a new measure of severity of delirium. Int Psychogeriatr 10:421–433
Ramsay MA, Savege TM, Simpson BR, Goodwin R (1974) Controlled sedation with aphaxalonealphadolone. Br Med J 2:656–659
Chouinard G, Ross-Chouinard A, Annable L, Jones B (1980) Extrapyramidal symptom rating scale. Can J Neurol Sci 7:233
Simpson GM, Angus JW (1970) A rating scale for extrapyramidal side effects. Acta Psychiatr Scand Suppl 212:11–19
Skrobik Y (2002) Haloperidol should be used sparingly. Crit Care Med 30:2613–2614
Caroff S, Rosenberg H, Mann S, Campbell E, Sullivan K (2002) Neuroleptic malignant syndrome in the critical care unit. Crit Care Med 30:2609–2610
Trzepacz P (2000) Semin Clin Neuropsychiatry 5:132–148
Ross CA, Peyser CE, Shapiro I, Folstein MF (1991) Delirium: phenomenologic and etiologic subtypes. Int Psychogeriatr 3:135–147
Liptzin B, Levkoff SE (1992) An empirical study of delirium subtypes. Br J Psychiatry 161:843–845
Acknowledgement
Support for this study was generously provided by a (peer-reviewed) grant from the Zyprexa fund, Eli-Lilly, North America.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Skrobik, Y.K., Bergeron, N., Dumont, M. et al. Olanzapine vs haloperidol: treating delirium in a critical care setting. Intensive Care Med 30, 444–449 (2004). https://doi.org/10.1007/s00134-003-2117-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-003-2117-0