
Abstract
Objective
To estimate the usefulness of 2-h creatinine clearance (CrCl) in the ICU and define variables that may reduce agreement.
Design
Prospective study.
Setting
Polyvalent ICU of a university hospital.
Patients
359 patients.
Interventions
We compared 24-h CrCl (CrCl-24h), as the standard measure, with 2-h CrCl (CrCl-2h) (at the start of the period) and the Cockroft–Gault equation (Ck-G).
Measurements and results
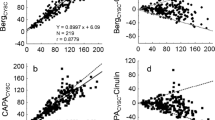
The 2-h sample was lost in two patients (0.6%) and the 24-h sample was lost in 50 patients (13.9%). The mean Ck-G was 87.4 ± 3.05, with CrCl-2h 109.2 ± 4.46 and CrCl-24h 100.9 ± 4.21 ml/min/1.73 m2 (r 2 of 0.88 for CrCl-2h and 0.84 for Ck-G). The differences from ClCr-24h were 21.8 ± 3.3 ( p < 0.001) for the Ck-G and 8.3 ± 2.6 ( p < 0.05) for CrCl-2h ( p < 0.05). In the subgroup of patients with CrCl-24h < 100 ml/min/1.73 m2, the CrCl-24h value was 52.9 ± 2.71 vs. 51.6 ± 2.14 for CrCl-2h ( p = ns) and 57.6 ± 2.56 ( p < 0.001) for the Ck-G. Patients with CrCl < 100 ml/min only showed variability in hyperglycemia during the 24-h period.
Conclusions
In intensive care patients, 24-h CrCl results in a large proportion of non-valid determinations, even under conditions of close monitoring. Two-hour CrCl is an adequate substitute, even in patients who are unstable or who have irregular diuresis where a 24-h collection is impossible. The Cockroft–Gault equation seems less useful in this setting.



Similar content being viewed by others


References
Liaño F, Junco E, Pascual J, Madero R, Verde E, Madrid Acute Renal Failure Study Group (1988) The spectrum of acute renal failure in intensive care unit compared with that seen in other settings. Kidney International 53:S16–S24
Herrera-Gutiérrez ME, Seller-Pérez G, Maynar-Moliner J, Sanchez-Izquierdo-Riera JA, grupo FRAMI de la SEMICYUC (2006) Epidemiología del FRA en las UCI españolas: estudio prospectivo multicéntrico FRAMI. Med Intensiva 30:260–267
Bellomo R, Ronco C, Kellum JA, Metha RL, Palevsky P, ADQI workgroup (2004) Acute renal failure: definition, outcome, measures, animal models, fluid therapy and information technology needs: the second international consensus conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care 8:204–212
Bellomo R, Kellum JA, Ronco C (2004) Defining acute renal failure: physiological principles. Intensive Care Med 30:33–37
Seller-Pérez G, Herrera-Gutiérrez ME, Banderas-Bravo E, Muñoz-Bono J, Fernández-Ortega J, Lebrón-Gallardo M (2005) Validation of 2 hours sampling creatinine clearance in ICU population, included unstable patients. Intensive Care Med (Suppl) 31(1):S146
Levey AS, Bosh JP, Lewis JB, Green T, Rogers N, Roth D (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 130:461–470
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG (1996) The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med 22:707–710
Menitz PG, Krenn CG, Steltzer H, Lang T, Ploder J, Lenz K, Le Gall JR, Drum WL (2002) Effect of acute renal failure requiring renal replacement therapy on outcome in critically ill patients. Crit Care Med 30:2051–2058
Ahlström A, Tallgren M, Peltonen S, Räsänen P, Pettilä V (2005) Survival and quality of life of patients requiring acute renal replacement therapy. Intensive Care Med 31:1222–1228
Andrews P, Azoulay E, Antonelli M, Brochard L, Brun-Buisson C, de Backer D, Dobb G, Fagon JY, Gerlach H, Groeneveld J, Mancebo J, Metnitz P, Nava S, Pugin J, Pinsky M, Radermacher P, Richard C, Tasker R (2006) Year in review in intensive care medicine. 2005. I. Acute respiratory failure and acute lung injury, ventilation, hemodynamics, education, renal failure. Intensive Care Med DOI 10.1007/s00134-005-0027-z
Hewitt SM, Dear J, Star RA (2004) Discovery of protein biomarkers for renal disease. J Am Soc Nephrol 15:1677–1689
Han WK, Bonventre JV (2004) Biologic markers for the early detection of acute kidney injury. Curr Opin Crit Care 10:476–482
Schrier RW, Wang W, Poole B, Mitra A (2004) Acute renal failure: definitions, diagnosis, pathogenesis, and therapy. J Clin Invest 114:5–14
Moran SM, Meyers BD (1985) Course of acute renal failure studied by a model of creatinine kinetics. Kidney Int 27:928–937
Lameire N, Hoste E (2004) Reflections on the definition, classification, and diagnostic evaluation of acute renal failure. Curr Opin Crit Care 10:468–475
Han WK, Bailly V, Abichandani R, Thadhani R. Bonventre JV (2002) Kidney injury molecule-1 (KIM-1): a novel biomarker for human renal proximal tubule injury. Kidney Int 62:237–244
Hoste EA, Damen J, Vanholder RC, Lameire NH, Delanghe JR, Van den Hauwe KV, Colardyn FA (2005) Assessment of renal function in recently admitted critically ill patients with normal serum creatinine. Nephrol Dial Transplant 20:747–753
Liu KD (2003) Molecular mechanisms of recovery from acute renal failure. Crit Care Med 31:S572–S581
Bell M, Liljestam E, Granath F, Fryckstedt J, Ekbom A, Martling CR (2005) Optimal follow-up time alter continuous replacement therapy in actual renal failure patients stratified with the RIFLE criteria. Nephrol Dial Transplant 20:354–360
Jelliffe R (2002) Estimation of creatinine clearance in patients with unstable renal function, without a urine specimen. Am J Nephrol 22:320–324
Cockroft DW, Gault MH (1976) Prediction of creatinine clearance from serum creatinine. Nephron 16:31–41
Kim KE, Onesti G, Ramirez O (1969) Creatinine clearance in renal disease: a reappraisal. BMJ 4:11–19
O'Connell MB, Wong MO, Bannick SD, Dwinell AM (1993) Accuracy of 2 and 8 hour urine collections for measuring creatinine clearance in the hospitalized elderly. Pharmacotherapy 13:135–142
Baumann TJ, Staddon JS, Horst HM, Bivins BA (1987) Minimum urine collections periods for accurate determinations of creatinine clearance in critically ill patients. Clin Pharm 6:393–398
Wilson RF, Soullier G (1980) The validity of two hour creatinine clearance studies in critically ill patients. Crit Care Med 8:281–284
Herget-Rosenthal S, Kribben A, Pietruck F, Ross B, Philipp T (1999) Two by two hour creatinine clearance: repeatable and valid. Clin Nephrol 51:348–354
Uchino S, Doig G, Bellomo R, Motimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Nacedo E, Gibney N, Tolwani A, Ronco C, Kellum JA, the Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) investigators (2004) Diuretics and mortality in acute renal failure. Crit Care Med 32:1669–1677
Stevens LA, Coresh J, Greene T, Levey AS (2006) Assessing kidney function – measured and estimated glomerular filtration rate. N Engl J Med 354:2473–2483
Delanaye P, Lambermont B, Chapelle JP, Gielen J, Gerard P, Rorive G (2004) Plasmatic cystatin C for the estimation of glomerular filtration rate in intensive care units. Intensive Care Med 30:980–983
Villa P, Jiménez M, Soriano MC, Manzanares J, Casasnovas P (2005) Serum cystatin C concentration as a marker of acute renal dysfunction in critically ill patients. Critical Care 9:139–143
Herget-Rosenthal S, Marggaf G, Husing J, Goring F, Pietruck F, Janssen O, Philipp T, Kribben A (2004) Early detection of acute renal failure by serum cystatin C. Kidney Int 66:1115–1122
Filler G, Foster J, Acker A, Lepage N, Akbari A, Ehrich JHH (2005) The Cockroft–Gault equation should not be used in children. Kidney Int 75:2321–2324
Author information
Authors and Affiliations
Corresponding author
Additional information
All the authors participated actively in the present study. This is an original paper that has not been submitted for publication elsewhere, though partial results of the study were presented at the Annual Congress of the ESICM in Amsterdam (September 2005), and the final results were presented at the Annual Congress of the SEMICYUC (Pamplona, 2006).
The authors received no external financing for conduct of the study, and there are no conflicts of interest for any of them.
This article is discussed in the editorial available at: http://dx.doi.org/10.1007/s00134-007-0766-0.
Rights and permissions
About this article
Cite this article
Herrera-Gutiérrez, M.E., Seller-Pérez, G., Banderas-Bravo, E. et al. Replacement of 24-h creatinine clearance by 2-h creatinine clearance in intensive care unit patients: a single-center study. Intensive Care Med 33, 1900–1906 (2007). https://doi.org/10.1007/s00134-007-0745-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-007-0745-5