
Abstract
Summary
Using national Medicare data from 1999–2006, we evaluated the relationship between travel distance and receipt of dual-energy X-ray absorptiometry (DXA). After adjusting for potentially confounding factors, travel distance was strongly associated with DXA testing. Rural residents were most strongly dependent on the availability of DXAs performed in physician offices.
Introduction
Medicare reimbursement for DXAs performed in non-facility settings (e.g., physician offices) decreased in 2007. With declining reimbursement, some DXA providers may cease providing this service, which would increase travel distance for some people. The impact of travel distance on access to DXA is unclear.
Methods
Using national Medicare data, we identified claims for DXA to evaluate trends in the number and locations of DXAs performed. Travel distance was the distance from beneficiaries’ residence and the nearest DXA provider. Binomial regression evaluated the relationship between travel distance and receipt of DXA.
Results
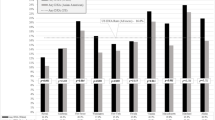
In 2006, 2.9 million DXAs were performed, a 103% increase since 1999. In 2005–2006, 8.0% of persons were tested at non-facility sites versus 4.2% at facility sites. The remainder (88%) had no DXA. Persons traveling 5–9, 10–24, 25–39, and 40–54, and ≥55 miles were less likely to receive DXA (adjusted risk ratios = 0.92, 0.79, 0.43, 0.32, and 0.26, respectively, <5 miles referent). Rural residents were more dependent than urban residents on the availability of DXA from non-facility providers.
Conclusion
Approximately two-thirds of DXAs in 2005–2006 were performed in non-facility settings (e.g., physician offices). Rural residents would have preferentially reduced access to DXA if there were fewer non-facility sites.


Similar content being viewed by others


References
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 22(3):465–475
Lewiecki EM, Watts NB, McClung MR et al (2004) Official positions of the international society for clinical densitometry. J Clin Endocrinol Metab 89(8):3651–3655
Black DM, Cummings SR, Karpf DB et al (1996) Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Lancet 348:1535–1541
Black DM, Delmas PD, Eastell R et al (2007) Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med 356(18):1809–1822
Harris ST, Watts NB, Genant HK et al (1999) Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. JAMA 282:1344–1352
Ettinger B, Black D, Mitlak B, Knickerbocker R, Nickelsen T, Genant HK, Christiansen C, Delmas PD, Zanchetta JR, Stakkestad J, Gluer CC, Krueger K, Cohen FJ, Eckert S, Ensrud KE, Avioli LV, Lips P, Cummings SR (1999) Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. JAMA 282(7):637–645
Curtis JR, Carbone L, Cheng H et al (2008) Longitudinal trends in use of bone mass measurement among older americans, 1999–2005. J Bone Miner Res 23(7):1061–1067
Cadarette SM, Gignac MA, Jaglal SB, Beaton DE, Hawker GA (2007) Access to osteoporosis treatment is critically linked to access to dual-energy X-ray absorptiometry testing. Med Care 45(9):896–901
Watts NB (1999) Understanding the bone mass measurement act. J Clin Densitometry 2:211–217
National Osteoporosis Foundation (2008) Clinician’s Guide to prevention and treatment of osteoporosis
The Lewin Group (2007) Assessing the total cost of providing DXA in the office-based setting and scoring a reimbursement alternative. Presented to CMS August 28
http://www.resdac.umn.edu/CCW/CCWFAQ.asp, accessed April 25th, 2008
Curtis JR, Laster A, Becker D et al (2008) Regional variation in the denial of reimbursement for bone mineral density testing among U.S. Medicare beneficiaries. J Clin Densitom 11:568–574
Deyo RA, Cherkin DC, Ciol MA (1992) Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 45(6):613–619
Andersen RM (1995) Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav 36(1):1–10
Aday LA, Andersen R (1974) A framework for the study of access to medical care. Health Serv Res 9(3):208–220
Kern LM, Powe NR, Levine MA et al (2005) Association between screening for osteoporosis and the incidence of hip fracture. Ann Intern Med 142(3):173–181
Federal Register: CMS 1321-FC. November 2006. “Medicare Program: Revisions to Payment Policies Five Year Review of Work Relative Value Units, Changes to the Practice Expense Methodology Under the Physician Fee Schedule and other Changes to Payment Under Part B; Revisions to the Payment Policies of Ambulance Services Under the Fee Schedule for Ambulance Services; and Ambulance Inflation Factor Update for CY 2007
Federal Register: CMS 1385-FC. November 2007. Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule, and Other Part B Payment Policies for CY 2008; Revisions to the Payment Policies of Ambulance Services Under the Ambulance Fee Schedule for CY 2008; and the Amendment of the E-Prescribing Exemption for Computer-Generated Facsimile Transmissions
McClellan M, McNeil BJ, Newhouse JP (1994) Does more intensive treatment of acute myocardial infarction in the elderly reduce mortality? Analysis using instrumental variables. Jama 272(11):859–866
Solomon DH, Polinski JM, Truppo C et al (2006) Access to bone mineral density testing in patients at risk for osteoporosis. Osteoporos Int 17(12):1749–1754
Shea AM, Curtis LH, Hammill BG, DiMartino LD, Abernethy AP, Schulman KA (2008) Association between the Medicare modernization act of 2003 and patient wait times and travel distance for chemotherapy. JAMA 300(2):189–196
Phibbs CS, Luft HS (1995) Correlation of travel time on roads versus straight line distance. Med Care Res Rev 52(4):532–542
Acknowledgments
This research was supported by a contract between UAB and Amgen, Inc. Only the authors from UAB had access to the Medicare data used. The analysis, presentation and interpretation of the results were solely the responsibility of the authors. Some of the investigators (J.R.C., K.G.S.) also receive salary support from the National Institutes of Health (AR053351, AR052361), the Agency for Healthcare Research and Quality (U18 HS016956), and the Arthritis Foundation (J.R.C.).
Conflicts of interest
J.R.C.: Consulting: Roche, UCB, Procter & Gamble; speakers bureau: Merck, Procter & Gamble, Eli Lilly, Roche, Novartis; research grants: Merck, Procter & Gamble, Eli Lilly, Amgen, Novartis
A.L.: Speakers bureau: Eli Lily, Novartis, Roche, GSK
D.J.B.: Research grants: Amgen
L.C.: Consulting and speaker’s bureau: Merck, Procter & Gamble, Aventis, Novartis
L.G.: Research grants: Amgen
M.L.K.: Consulting and Research grants: Amgen, Eli Lilly
R.M.: Research grants: Amgen
M.M.: Research grants: Amgen
K.G.S.: Consulting: Merck, Novartis; speakers bureau: Merck, Procter & Gamble, Aventis, Eli Lilly, Roche, Novartis, Amgen; research grants: Novartis, Amgen, Eli Lilly, Roche
S.B.T.: Consulting and research grants: Merck, Procter & Gamble, Eli Lilly, Roche, GSK, Novartis, Wyeth, Amgen
E.D.: Research grants: Amgen
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
About this article
Cite this article
Curtis, J.R., Laster, A., Becker, D.J. et al. The geographic availability and associated utilization of dual-energy X-ray absorptiometry (DXA) testing among older persons in the United States. Osteoporos Int 20, 1553–1561 (2009). https://doi.org/10.1007/s00198-008-0821-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-008-0821-x