
Abstract
Background
The purpose of this study was to examine if Red Bull® Energy Drink can counteract sleepiness and driving impairment during prolonged driving.
Methods
Twenty-four healthy volunteers participated in this double-blind placebo-controlled crossover study. After 2 h of highway driving in the STISIM driving simulator, subjects had a 15-min break and consumed Red Bull® Energy Drink (250 ml) or placebo (Red Bull® Energy Drink without the functional ingredients: caffeine, taurine, glucuronolactone, B vitamins (niacin, pantothenic acid, B6, B12), and inositol) before driving for two additional hours. A third condition comprised 4 h of uninterrupted driving. Primary parameter was the standard deviation of lateral position (SDLP), i.e., the weaving of the car. Secondary parameters included SD speed, subjective driving quality, sleepiness, and mental effort to perform the test.
Results
No significant differences were observed during the first 2 h of driving. Red Bull® Energy Drink significantly improved driving relative to placebo: SDLP was significantly reduced during the 3rd (p < 0.046) and 4th hour of driving (p < 0.011). Red Bull® Energy Drink significantly reduced the standard deviation of speed (p < 0.004), improved subjective driving quality (p < 0.0001), and reduced mental effort to perform the test (p < 0.024) during the 3rd hour of driving. Subjective sleepiness was significantly decreased during both the 3rd and 4th hour of driving after Red Bull® Energy Drink (p < 0.001 and p < 0.009, respectively). Relative to uninterrupted driving, Red Bull® Energy Drink significantly improved each parameter.
Conclusion
Red Bull® Energy Drink significantly improves driving performance and reduces driver sleepiness during prolonged highway driving.
Similar content being viewed by others

Introduction
Sleepiness and fatigue can compromise the ability to drive a car. In several studies, 14.5% to 20% of drivers reported falling asleep while driving (Beirness et al. 2005; National Sleep Foundation 2002; Van Laar et al. 2008). Causal factors of driver sleepiness include sleep restriction, sleep disorders, and circadian factors, but also driving-related factors such as a monotonous environment or low traffic density may contribute to driver sleepiness. A highway is an example of a monotonous driving environment that can increase the likelihood of accidents (Stutts et al. 1999). Studies estimate that sleepiness accounts for 15–23% of all motor vehicle accidents on highways (Horne and Reyner 1995; Maycock 1996).
Highway driving involves two important factors that can lead to driver sleepiness. First, highway driving is associated with monotony: The driving environment is relatively uneventful, predictable, and repetitive. While safe handling of a vehicle requires sustained attention, monotony leads to the opposite: Arousal levels decline and are replaced by inattention and sleepiness resulting in driving impairment (Thiffault and Bergeron 2003). Second, time-of-task effects, i.e., increased time spent behind the wheel, progressively impair driving performance, and may lead to an increase in accident risk (Connor et al. 2001). How these and other factors play a role in highway driving is described in several concepts such as “passive task-related-fatigue”, “highway hypnosis”, or “driving without attention mode”. Situations of mental underload may lead to the driving task become automated. Drivers rely less on feedback from the environment which leads to a reduction of effort to perform the driving task. This leads to a decrease in arousal and alertness and possibly a failure to notice errors and react to sudden changes in traffic (Gimeno et al. 2006; May and Baldwin 2009; Kerr 1991; Wertheim 1991).
To prevent sleep-related vehicle accidents, public campaigns recommend scheduled breaks in between driving sessions. The message of these campaigns is to limit driving time to 2 h followed by a break of at least 15 min before continuing driving. It can be questioned if a 15-min break is sufficient to restore baseline performance. Driving simulator data showed that a 30-min break after an hour of driving was insufficient to normalize driving performance (Horne and Reyner 1996), while an on-the-road study demonstrated that rested individuals could drive for 10 h without a noteworthy increase in lane crossings when 15-min breaks (prolonged to 30 min at lunchtime) were applied after every 1.75 h of driving (Philip et al. 2005a). Therefore, the general recommendation is always to stop driving if one feels impaired or sleepy. Unfortunately, drivers differ greatly in their ability to sustain attention in monotonous situations (Nilsson et al. 1997). Moreover, recognizing sleepiness and judging its possible impact on one’s own driving performance is hard (Schmidt et al. 2009). Therefore, applying suitable countermeasures of driver sleepiness may be an important tool to prevent driving impairment.
Countermeasures, such as taking a nap and caffeine, have been proven effective, especially when driving in the early morning, at night, or when sleep-deprived (Biggs et al. 2007; Philip et al. 2006; Reyner and Horne 1997, 2000). In addition, energy drinks are popular to overcome driver fatigue. Worldwide, the most popular energy drink is Red Bull® Energy Drink. Red Bull® Energy Drink contains several ingredients including caffeine, taurine, glucuronolactone, B vitamins, and inositol. The combination of these ingredients is believed to account for the positive effects on cognitive performance, attention, and driving performance. In laboratory tests of mental performance, Red Bull® Energy Drink improved (choice) reaction time, energetic arousal, subjective alertness, concentration, and memory (Alford et al. 2001; Warburton et al. 2001), as well as attention capacity in a stressful situation (Seidl et al. 2000). Driving was improved in all previous studies examining Red Bull® Energy Drink, or drinks with similar ingredients (Gershon et al. 2009; Horne and Reyner 2001; Reyner and Horne 2002). In subjects who were sleep restricted to 5 h, Red Bull® Energy Drink (500 ml) reduced the number of lateral lane crossings and decreased reaction time in a secondary task (Horne and Reyner 2001). Subjects drove for 30 min, had a 30-min break, and then drove for two additional hours. The effects lasted from 0 to 90 min after the break. Similar results were obtained in a subsequent study in which 250 ml was administered (Reyner and Horne 2002): Lateral lane crossings and Karolinska Sleepiness Scale (KSS) sleepiness scores were decreased until 90 min after the break. A similar energy drink (500 ml) led to a more stable lane position (RMS of the standard deviation of lateral position (SDLP)) during 2 h of driving in non-sleep-deprived individuals. Steering wheel variations, fatigue, and reaction time in a simultaneous reaction time task were also improved (Gershon et al. 2009).
The characteristics of these studies include that subjects were sleep-deprived before taking part in the driving test (Horne and Reyner 2001; Reyner and Horne 2002), consumed 500 ml of Red Bull® Energy Drink (Horne and Reyner 2001), and drove only for half an hour (Horne and Reyner 2001; Reyner and Horne 2002) before Red Bull® Energy Drink was consumed.
To test the impact of Red Bull® Energy Drink on prolonged highway driving of non-sleep-deprived individuals, a paradigm was developed in which subjects drove in an advanced driving simulator for 2 h, had a 15-min break in which 250 ml of energy drink or placebo was consumed, followed by two more hours of highway driving. In a third condition, they drove for 4 h without a break and without any treatment (in the text referred to as uninterrupted driving or “no brake” condition). Based on previous research discussed above, it is hypothesized that after drinking Red Bull® Energy Drink, driving will be significantly improved when compared to placebo or driving without a break.
Materials and methods
This study was a double-blind, randomized, placebo-controlled, crossover study. No formal ethical approval was required by the Medical Ethical Committee of the University Medical Center Utrecht. The study was conducted according to the ICH Guidelines for “Good Clinical Practice” and the Declaration of Helsinki and its latest amendments. Written informed consent was obtained from the participants before taking part in the study.
Subjects
Twenty-four adult healthy volunteers (12 males and 12 females) were recruited by means of public advertisements at and around Utrecht University campus. Subjects were included if they were aged between 21 and 35 years, were regular drivers (>5,000 km/year), had been in the possession of a drivers license for at least 3 years, had a normal body mass index (21 < BMI < 30; 55–85 kg), were non-smokers, had regular sleeping hours, and were otherwise healthy. Sleep disturbances were assessed with the SLEEP-50 questionnaire (Spoormaker et al. 2005). The Epworth Sleepiness Scale (ESS) was administered to assess general levels of daytime sleepiness (Johns 1991). Subjects with ESS scores above 10 were excluded from participation. Other inclusion criteria were moderate caffeine consumption (two to four glasses of caffeine-containing beverages per day) and infrequent energy drink consumers (<1 drink per month). On each visit, urine samples were collected to test for drugs of abuse (amphetamines (including 3,4-methylenedioxymethamphetamine), barbiturates, cannabinoids, benzodiazepines, cocaine, and opiates) and a pregnancy test in female subjects (β-human chorionic gonadotropin test). In addition, alcohol use was tested using the Dräger Alcotest 7410 Breath Analyzer. Alcohol consumption was not permitted from 24 h before the start of the test day and on test days. From awakening until the end of the tests, caffeinated beverages and smoking were not allowed.
Study design
The study comprised one training day and three test days. On the training day, participants were screened and familiarized with the test procedures. If subjects met all inclusion and exclusion criteria, a practice session in the STISIM driving simulator was performed. Thereafter, subjects completed the Simulator Sickness Questionnaire (Kennedy et al. 1993) to determine possible simulator sickness. Included subjects were randomly assigned to a treatment order comprising three conditions: (1) Red Bull® Energy Drink + break, (2) placebo + break, and (3) no break + no treatment condition (see Fig. 1).

Overview of the test days
On test days, drug or alcohol use, pregnancy, illness, and medication use were checked after arrival. In addition, quality of sleep was assessed using the 14-item Groningen Sleep Quality Scale (Mulder-Hajonides van der Meulen et al. 1980), in which 0 indicates high quality sleep and 14 indicates very poor sleep. When subjects met all criteria, they performed a two times 60-min driving session in the STISIM driving simulator. On two test days, a 15-min break was scheduled in which subjects received either of the double-blind treatments. After the break, another driving session of two times 60 min was performed. In the “no break” condition, participants drove for a total of 4 h without a break. In each condition, every 60-min driving session was followed by subjective assessments on driving quality, driving style, mental effort to perform the test, and sleepiness. Test sessions were performed either in the morning (0800–1300 hours) or in the afternoon (1300–1700 hours) in a balanced manner. Each subject started each test day at the same time.
Treatments
Treatments were 250 ml of Red Bull® Energy Drink or placebo, administered during the break. Per 250-ml Red Bull® Energy Drink contains 21 g sucrose, 5 g glucose, 1 g taurine, 80 mg caffeine, 60 mg glucuronolactone, 50 mg inositol, and B vitamins (niacin, pantothenic acid, vitamin B6, vitamin B12). The placebo drink was Red Bull® Energy Drink without taurine, caffeine, glucuronolactone, inositol, and vitamin B complex. The blinded Red Bull® Energy Drink and placebo beverage samples were provided by Red Bull GmbH. Treatment appearance (bottle and color of the beverage) was double-blinded, and a nose clip was worn to enhance treatment blinding. Drinks were consumed within 5 min, starting from 5 min after onset of the break. Subject randomization was conducted at Utrecht University. The treatment code was revealed by Red Bull GmbH after the study was completed and data were analyzed.
STISIM highway driving test
Driving tests were performed using STISIM Drive™ (version M300, Systems Technology, Inc., Hawthorne, CA, USA). The simulator consists of a car unit with adjustable car seats and a dashboard and includes a steering wheel, turn sign indicators, gear lever, clutch, brake, and gas pedals for vehicle control. The system generates a realistic roadway scenery which is projected on a screen (2.10 × 1.58 m), placed 1.90 m in front of the center of the steering wheel. Speed and gear number are displayed on the dashboard and the screen. Auditory feedback is provided by speakers and included sound of the engine, braking, speeding in curves, and driving off-road. Whenever a collision occurs, a broken windshield and the sound of braking glass are presented. Subsequently, the car is placed back in the middle of the right traffic lane and the test continues.
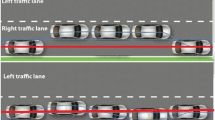
A 100-km highway driving test scenario was developed by EyeOctopus B.V., tailored to Dutch traffic situations (e.g., Dutch traffic signs, vehicles, buildings, and sceneries). The test scenario aims to resemble the on-the-road driving test in real traffic. The scenario consists of a two-lane highway in each direction with a lane width of 3.5 m. The environment is monotonous and comprised trees, occasional bridges, and hills as well as other traffic (see Fig. 2).

Highway scenery of the STISIM driving simulator
Subjects were instructed to drive with a steady lateral position in the right (slower) traffic lane while maintaining a steady speed of 95 km/h. Overtaking maneuvers were allowed whenever a subject approached a slower moving car. These events were removed from the data before analysis. Weaving of the car, expressed by the SDLP (centimeters), was the primary outcome measure of this test (see Fig. 3).

Meaning of the standard deviation of lateral position (SDLP)
SDLP has been used as primary parameter in standardized on-the-road tests. SDLP showed to be sensitive to dose-dependent impairment after administration of a variety of psychoactive drugs including hypnotics, antidepressants, and antihistamines (Verster and Mets 2009). On-the-road, SDLP increments corresponding to the most common legal limits for driving were +2.4 cm (0.05%), +4.1 cm (0.08%), and +5.3 cm (0.10%; Louwerens et al. 1987). Recent research showed that the highway driving test scenario and its primary parameter SDLP in the STISIM driving simulator also differentiate between impairment produced after consumption of different dosages of alcohol (Mets et al., submitted for publication).
The second outcome measure was the standard deviation of speed (kilometers per hour). Mean lateral position (centimeters) and mean speed (kilometers per hour) were control variables.
Subjective assessments
After each hour of driving, participants made subjective assessments on driving and sleepiness causing a 2-min interruption of the driving task. Subjects indicated their perceived driving quality on a visual analog scale, ranging from 0 (“I drove exceptionally poorly”) to 20 (“I drove exceptionally well”). In addition, mental effort exerted during the driving test was rated on an interval scale (15 cm) ranging from “almost no effort” to “very great effort”. Furthermore, subjects completed a driving style questionnaire (McCormick et al. 1987), which consisted of different bipolar differential scales (10 cm) including foolish-wise, unpredictable–predictable, dangerous-safe, tense-relaxed, inconsiderate–considerate, and irresponsible–responsible. Finally, the KSS was used to rate sleepiness on a scale of 1 to 9, ranging from 1 (very alert) to 9 (very sleepy, an effort to stay awake, fighting sleep; Åkerstedt and Gillberg 1990). Completion of the subjective assessments took approximately 2 min. Driving was resumed right thereafter.
Statistical analysis
Data were analyzed using ANOVA general linear model for repeated measures (two-tailed, p ≤ 0.05). For the STISIM driving simulator test, the primary parameter was the SDLP.
Results
Twenty-four healthy subjects participated in the study. Three male subjects were excluded due to protocol violations and resulting statistical outliers. A total of 21 subjects were included in the analysis (nine men and 12 women; age (mean (SD) 22.8 (1.4) years)). They were of normal weight range for height (BMI mean = 23.6, SD = 2.4), had their driver’s license at least 3 years (mean = 57.8 months, SD = 17.2 months), and were regular drivers (minimum 5,000 km/year, mean = 11,976 km/year, SD = 10,569 km/year). Overall, subjects reported a normal sleep quality and duration the night before testing, and no significant differences were found between the test days or conditions. Results from the study are summarized in Table 1.
Driving test
For the primary parameter (SDLP), the results are shown in Fig. 4. In the first 2 h, driving test parameters did not differ significantly between the treatment conditions. When compared to placebo, Red Bull® Energy Drink significantly reduced SDLP during the 3rd (p < 0.046) and 4th (p < 0.011) hour of driving. Similarly, compared to the uninterrupted driving condition, Red Bull significantly reduced SDLP in hour 3 (p < 0.003) and hour 4 (p < 0.013).

Standard deviation of lateral position (SDLP). *p < 0.05, significant difference compared to placebo
Although in the placebo condition driving improvement (i.e., reduced SDLP) is seen after the break, there were no significant differences between the placebo and the “no break” condition. Gender and time-of-day effects were not significant.
A post hoc analysis of the effects per 50 km, or approximately 30 min, showed that SDLP values in the Red Bull® condition were significant lower compared to placebo. This effect was seen from half an hour after the break, until the end of the test (250–300 km: p < 0.028; 300–350 km: p < 0.010; 350–400 km: p < 0.024). Prolonged driving compared to placebo gave no significant results.
Figure 5 shows that Red Bull® Energy Drink significantly reduced speed variability compared to placebo and uninterrupted driving in the 3rd hour (p < 0.004 and p < 0.0001, respectively). In the 4th hour, standard deviation of speed differed significantly between Red Bull® Energy Drink and uninterrupted driving (p < 0.003).
No effects were found on the mean lateral position and mean speed, confirming that subjects performed the driving test according to the instructions.

Standard deviation of speed (SDS). *p < 0.05, significant difference compared to placebo
Subjective driving assessments
Relative to placebo and uninterrupted driving, Red Bull® Energy Drink significantly improved subjective driving quality during the 3rd hour of driving (p < 0.0001). Similarly, mental effort during driving was decreased after the intake of Red Bull® Energy Drink after 3 h of driving compared to placebo (p < 0.024) and uninterrupted driving (p < 0.005). In accordance with these results, after 3 h, each aspect of driving style was found to be improved in the Red Bull® Energy Drink condition when compared to the other conditions (p < 0.05). That is, subjects rated their driving as more wise, safe, responsible, relaxed, predictable, and considerate in the first hour after the intake of Red Bull® Energy Drink. In the 4th hour of driving, no significant differences were reported except for the fact that subjects judged their driving as significantly more safe after intake of Red Bull® Energy Drink when compared to uninterrupted driving (p < 0.026).
To confirm if drivers were aware of changes in driving performance, we computed the correlation between difference scores for SDLP and subjective driving quality (3rd hour scores − 2nd hour scores). In the Red Bull condition, the correlation was significant (r = −0.548, p < 0.010) as well as in placebo condition (r = −0.517, p < 0.016), but not in the prolonged driving condition. This indicates that whereas subjects acknowledged objective driving improvement after having a break (with or without Red Bull), they were not aware of driving impairment in the prolonged driving condition.
Subjective sleepiness
After the third and fourth hour, sleepiness scores were significantly lower in the Red Bull® Energy Drink condition when compared to placebo (p < 0.001 and p < 0.009, respectively) and uninterrupted driving (p < 0.0001 and p < 0.026, respectively). Surprisingly, a break without Red Bull® Energy Drink did not significantly reduce sleepiness levels when compared to uninterrupted driving (see Fig. 6).

Karolinska Sleepiness Scale. *p < 0.05, significant difference compared to placebo
Discussion
This study shows that Red Bull® Energy Drink significantly improves driving performance and reduced subjective sleepiness during subsequent driving. The effects of Red Bull® Energy Drink were supported by assessments of subjective driving quality and driving style and were in accordance with the effects observed in previous studies (Horne and Reyner 2001; Reyner and Horne 2002; Gershon et al. 2009). In addition to previous studies, the present study demonstrates that Red Bull® Energy Drink improves driving ability in healthy non-sleep-deprived individuals when consuming a standard 250-ml can of Red Bull® Energy Drink.
Interestingly, while rested individuals would be expected to benefit from breaks, the 15-min break in our design did not lead to significantly lower SDLP values in hours 3 and 4 when compared to the uninterrupted driving condition, nor did it lead to a decrease in sleepiness levels. We have no clear explanation for this finding, and it is in contrast to previous studies (e.g., Philip et al. 2005a; Sagaspe et al. 2008). Further studies should be conducted into the effectiveness of scheduling breaks during prolonged highway driving.
The average difference in SDLP between the placebo and Red Bull condition was 2.3 cm in the third hour and 3.1 cm in the fourth hour. This difference is comparable to the effect observed for blood alcohol concentrations higher than 0.05% (Mets et al., submitted for publication), i.e., above the legal limit for driving in most European countries.
It has been suggested that the combination of ingredients produce the beneficial effects of Red Bull® Energy Drink (Reyner and Horne 2002). A post hoc analysis, based on the results per 30 min, showed that Red Bull® Energy Drink significantly reduced SDLP starting from 30 min after the break until 2 h after intake. This is in accordance with the pharmacokinetics of caffeine showing peak plasma concentrations after 30 to 60 min (Roehrs and Roth 2008; Lorist and Tops 2003) and a half-life of 2 to 10 h (Sawyer et al. 1982; Smith 2002). Although higher dosages of caffeine (100–300 mg) have been shown to improve driving performance (Brice and Smith 2001; Regina et al. 1974; Reyner and Horne 2000; Biggs et al. 2007; De Valck and Cluydts 2001; Sagaspe et al. 2007; Philip et al. 2006; Reyner and Horne 1997), it is surprising that the effect of lower caffeine on driving (e.g., one cup of coffee) has not been examined. Some studies did, however, report positive effects of low dosages of caffeine (−75 mg) on driving-related skills such as reaction time, performance, and mood (Childs and De Wit 2006; Durlach 1998; Haskell et al. 2005; Quinlan et al. 2000; Smit and Rogers 2000; Smith et al. 1999).
Taurine’s effects on driving have not been studied, but research did show that taurine can alleviate visual fatigue (Zhang et al. 2004). Taurine’s peak plasma concentration is reached after about 90 min, and concentrations then decline within 180–270 min (Trautwein and Hayes 1995). The role of taurine in CNS effects is unclear, as animal experiments could not demonstrate effects on brain taurine levels (Sved et al. 2007). Although B vitamins play a role in cognitive functioning (Calvaresi and Bryan 2001; Franchi et al. 1998; Huskisson et al. 2007), their effects on driving are unknown. As Red Bull® Energy Drink contains relatively low levels of vitamins and was administered only once in this study, it is unlikely that these ingredients play a major role in driving improvement. No scientific evidence is available on the contribution of glucuronolactone (Kim 2003). Finally, glucose is unlikely to produce the beneficial effects of Red Bull® Energy Drink as both the drink and the placebo contained sugar. In conclusion, further studies on the ingredients of Red Bull® Energy Drink are important to elucidate their specific effects on cognitive performance and driving.
One of the limitations of this study was that each hour of driving was followed by subjective assessments, causing a 2-min interruption of the driving task. Although subjects remained seated in the car and were occupied with completing the VAS scales, this may have had an effect. On the other hand, a 2-min break is also seen in real-life driving, for example in conditions such as being stopped by traffic lights or traffic jams. Another limitation is that we did not control previous-night sleep quality using objective measures such as EEG or actigraphy but used a questionnaire. In addition, the development of sleepiness and experiencing monotony may differ between simulated and actual driving. It was suggested that sleepiness develops sooner and is more pronounced in a driving simulator (Anund et al. 2009; Philip et al. 2005b). The absence of actual risk in the driving simulator also differs from on-the-road driving. Preferably, the effect of Red Bull® Energy Drink on driving performance should therefore be replicated in on-the-road studies in normal traffic. Finally, with a mean age of 23, the population of drivers was relatively young. Although energy drinks are popular among this age group, it may be interesting to examine the effects of Red bull Energy Drink in older, more experienced drivers.
In conclusion, Red Bull® Energy Drink significantly improved driving ability relative to placebo and uninterrupted driving. For the primary parameter (SDLP), this effect was significant for 2 h after drinking Red Bull® Energy Drink. Subjective assessments consistently confirmed these findings.
References
Åkerstedt T, Gillberg M (1990) Subjective and objective sleepiness in the active individual. Int J Neurosci 52:29–37
Alford C, Cox H, Wescott R (2001) The effects of Red Bull Energy Drink on human performance and mood. Amino Acids 21:139–150
Anund A, Kecklund G, Kircher A, Tapani A, Akerstedt T (2009) The effects of driving situation on sleepiness indicators after sleep loss: a driving simulator study. Ind Health 47:393–401
Beirness DJ, Simpson HM, Desmond K (2005) The Road Safety Monitor 2004, drowsy driving. Traffic Injury Research Foundation, Ottawa
Biggs SN, Smith A, Dorrian J, Reid K, Dawson D, Van den Heuvel C, Baulk S (2007) Perception of simulated driving performance after sleep restriction and caffeine. J Psychosom Res 63:573–577
Brice C, Smith A (2001) The effects of caffeine on simulated driving, subjective alertness and sustained attention. Hum Psychopharmacol Clin Exp 16:523–531
Calvaresi E, Bryan J (2001) B vitamins, cognition, and aging: a review. J Gerontol Ser B Psychol Sci Soc Sci 56:P327–P339
Childs E, De Wit H (2006) Subjective, behavioral, and physiological effects of acute caffeine in light, nondependent caffeine users. Psychopharmacol 185:514–523
Connor J, Norton R, Ameratunga S, Robinson E, Wigmore B, Jackson R (2001) Prevalence of driver sleepiness in a random population-based sample of car driving. Sleep 24:688–694
De Valck E, Cluydts R (2001) Slow-release caffeine as a countermeasure to driver sleepiness induced by partial sleep deprivation. J Sleep Res 10:203–209
Durlach PJ (1998) The effects of a low dose of caffeine on cognitive performance. Psychopharmacol 140:116–119
Franchi F, Baio G, Bolognesi AG, Braghieri C, Luchetti L, Anzivino F (1998) A review on the relations between the vitamin status and cognitive performances. Arch Gerontol Geriatr 26(Supplement 1):207–214
Gershon P, Shinar D, Ronen A (2009) Evaluation of experience-based fatigue countermeasures. Accident Anal Prev 41:969–975
Gimeno PT, Cerezuela GP, Montanes MC (2006) On the concept and measurement of driver drowsiness, fatigue and inattention: implications for countermeasures. Int J Vehicle Design 42: 67–86.
Haskell CF, Kennedy DO, Wesnes KA, Scholey AB (2005) Cognitive and mood improvements of caffeine in habitual consumers and habitual non-consumers of caffeine. Psychopharmacol 179:813–825
Horne JA, Reyner LA (1995) Sleep related vehicle accidents. BMJ 6979:565–567
Horne JA, Reyner LA (1996) Counteracting driver sleepiness: effects of napping, caffeine, and placebo. Psychophysiol 33:306–309
Horne JA, Reyner LA (2001) Beneficial effects of an “energy drink” given to sleepy drivers. Amino Acids 20:83–89
Huskisson E, Maggini S, Ruf M (2007) The influence of micronutrients on cognitive function and performance. J Int Med Res 35:1–19
Johns MW (1991) A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep 14:540–545
Kennedy RS, Lane NE, Berbaum KS, Lilienthal MG (1993) Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int J Aviat Psychol 3:203–220
Kerr JS (1991) Driving without attention mode (DWAM): a formalisation of inattentive states in driving. In: Gale AG, Brown ID, Haslegrave CM, Moorhead I, Taylor S (eds) Vision in vehicles—III. Elsevier, North Holland, pp 473–479
Kim W (2003) Debunking the effects of taurine in Red Bull Energy Drink. Nutr Bytes 9:1–7
Lorist MM, Tops M (2003) Caffeine, fatigue, and cognition. Brain Cogn 53:82–94
Louwerens JW, Gloerich ABM, De Vries G, Brookhuis KA, O’Hanlon JF (1987) The relationship between drivers’ blood alcohol concentration (BAC) and actual driving performance during high speed travel. In: Noordzij PC, Roszbach R (eds) Alcohol, drugs and traffic safety. Excerpta Medica, Amsterdam, pp 183–192
May JF, Baldwin CL (2009) Driver fatigue: the importance of identifying causal factors of fatigue when considering detection and countermeasure technologies. Transp Res 12:218–224
Maycock G (1996) Sleepiness and driving: the experience of UK car drivers. J Sleep Res 5:229–237
McCormick IA, Walkey FH, Green DE (1987) Comparative perceptions of driver ability—a confirmation and expansion. Accident Anal Prev 18:205–208
Mulder-Hajonides van der Meulen WREH, Wijnberg JR, Hollander JJ, De Diana IPF, van den Hoofdakker RH (1980) Measurement of subjective sleep quality. Eur Sleep Res Soc 5:98
National Sleep Foundation (2002) Sleep in America poll. National Sleep Foundation, Washington, DC
Nilsson T, Nelson TM, Carlson D (1997) Dev fatigue symptoms during simulated driving. Accident Anal Prev 79:479–488
Philip P, Sagaspe P, Moore N, Taillard J, Charles A, Guilleminault C, Bioulac B (2005a) Fatigue, sleep restriction and driving performance. Accident Anal Prev 37:473–478
Philip P, Sagaspe P, Taillard J, Valtat C, Moore N, Åkerstedt T, Charles A, Bioulac B (2005b) Fatigue, sleepiness, and performance in simulated versus real driving conditions. Sleep 28(12):1511–1516
Philip P, Taillard J, Moore N, Delord S, Valtat C, Sagaspe P et al (2006) The effects of coffee and napping on nighttime highway driving: a randomized trial. Ann Intern Med 144:785–791
Quinlan PT, Lane J, Moore KL, Aspen J, Rycroft JA, O’Brien DC (2000) The acute physiological and mood effects of tea and coffee: the role of caffeine level. Pharmacol Biochem Behav 66:19–28
Regina EG, Smith GM, Keiper CG, McKelvey RK (1974) Effects of caffeine on alertness in simulated automobile driving. J Appl Psychol 59:483–489
Reyner LA, Horne JA (1997) Suppression of sleepiness in drivers: combination of caffeine with a short nap. Psychophysiol 34:721–725
Reyner LA, Horne JA (2000) Early morning driver sleepiness: effectiveness of 200 mg caffeine. Psychophysiol 37:251–256
Reyner LA, Horne JA (2002) Efficacy of a ‘functional energy drink’ in counteracting driver sleepiness. Physiol Behav 75:331–335
Roehrs T, Roth T (2008) Caffeine: sleep and daytime sleepiness. Sleep Med Rev 12:153–162
Sagaspe P, Taillard J, Chaumet G, Moore N, Bioulac B, Philip P (2007) Aging and nocturnal driving: better with coffee or a nap? A randomized study. Sleep 30:1808–1813
Sagaspe P, Taillard J, Åkerstedt T, Bayon V, Espie S, Chaumet G et al (2008) Extended driving impairs nocturnal driving performances. PLoS ONE 3:e3493. doi:10.1371/journal.pone.0003493
Sawyer DA, Julia HL, Turin AC (1982) Caffeine and human behavior: arousal, anxiety, and performance effects. J Behav Med 5:415–439
Schmidt EA, Schrauf M, Simon M, Fritzsche M, Buchner A, Kincses WE (2009) Drivers’ misjudgement of vigilance state during prolonged monotonous daytime driving. Accident Anal Prev 41:1087–1093
Seidl R, Peyrl A, Nicham R, Hauser E (2000) A taurine and caffeine-containing drink stimulates cognitive performance and well-being. Amino Acids 19:635–642
Smit HJ, Rogers PJ (2000) Effects of low doses of caffeine on cognitive performance, mood and thirst in low and higher caffeine consumers. Psychopharmacol 152:167–173
Smith A (2002) Effects of caffeine on human behavior. Food Chem Toxicol 40:1243–1255
Smith A, Sturgess W, Gallagher J (1999) Effects of a low dose of caffeine given in different drinks on mood and performance. Hum Psychopharmacol 14:473–482
Spoormaker VI, Verbeek I, Van den Bout J, Klip EC (2005) Initial validation of the SLEEP 50 Questionnaire. Behav Sleep Med 3:227–246
Stutts JC, Wilkins JW, Vaughn B (1999) Why do people have drowsy driving crashes? Input from drivers who just did. AAA Foundation for Traffic Safety, Washington, DC
Sved DW, Godsey JL, Ledyard SL, Mahoney AP, Stetson PL, Ho S et al (2007) Absorption, tissue distribution, metabolism and elimination of taurine given orally to rats. Amino Acids 32:459–466
Thiffault P, Bergeron J (2003) Monotony of road environment and driver fatigue: a simulator study. Accident Anal Prev 35:381–391
Trautwein EA, Hayes KC (1995) Plasma and whole blood taurine concentrations respond differently to taurine supplementation (humans) and depletion (cats). Z Ernährungswiss 34:137–142
Van Laar W, Simpson H, Mayhew D, Robertson R (2008) Fatigued and drowsy driving: a survey of attitudes, opinions and behaviors. J Safety Res 39:303–309
Verster JC, Mets MAJ (2009) Psychoactive medication & traffic safety. Int J Environ Res Public Health 6:1041–1054
Warburton DM, Bersellini E, Sweeney E (2001) An evaluation of a caffeinated taurine drink on mood, memory and information processing in healthy volunteers without caffeine abstinence. Psychopharmacol 158:322–328
Wertheim AH (1991) Highway hypnosis: a theoretical analysis. In: Gale AG, Brown ID, Haslegrave CM, Moorhead I, Taylor S (eds) Vision in vehicles—III. Elsevier, North Holland, pp 467–472
Zhang M, Bi LF, Ai YD, Yang LP, Wang HB, Liu ZY, Sekine M, Kagamimori S (2004) Effects of taurine supplementation on VDT work induced visual stress. Amino Acids 26:59–63
Disclosure/Conflicts of interests
The study was registered at www.clinicaltrials.gov, trial identifier: NCT01007877. The study was financially supported by Red Bull GmbH. Over the past 3 years, JV has received compensation from Takeda Pharmaceuticals and BO has received compensation from Psychogenic Inc.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Mets, M.A.J., Ketzer, S., Blom, C. et al. Positive effects of Red Bull® Energy Drink on driving performance during prolonged driving. Psychopharmacology 214, 737–745 (2011). https://doi.org/10.1007/s00213-010-2078-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-010-2078-2