
Abstract
Purpose
AGS-1C4D4 is a human monoclonal antibody against prostate stem cell antigen (PSCA), a cell-surface protein expressed by most prostate cancers. AGS-1C4D4 is produced in Chinese hamster ovary (CHO) cells and has an identical sequence to AGS-PSCA, an anti-PSCA antibody produced in mouse hybridoma cells that has completed Phase I testing. Preclinical studies demonstrated comparability of AGS-1C4D4 to AGS-PSCA with respect to pharmacokinetics (PK) and tumor inhibition. However, because of differences in antibody-dependent cellular cytotoxicity between AGS-PSCA and AGS-1C4D4, a limited Phase I trial using AGS-1C4D4 was performed evaluating safety and PK.
Patients and methods
Thirteen patients with metastatic castration-resistant prostate cancer were enrolled. AGS-1C4D4 was administered intravenously every 3 weeks for four planned doses at 6, 12, 24, or 48 mg/kg. Primary endpoints were safety and PK. Secondary endpoints were immunogenicity and clinical activity. Disease assessments were conducted every 12 weeks and included radiographic and PSA evaluations. Patients with stable disease could receive extended treatment beyond four infusions.
Results
Adverse events were primarily grade 1–2, without any grade 3–4 drug-related toxicities or infusion reactions. Anti-AGS-1C4D4 antibodies were not detected. Similar to AGS-PSCA, serum AGS-1C4D4 concentrations declined biphasically and elimination was characterized by slow clearance (CL) and a long terminal half-life (t 1/2). Median CL for the four dose levels ranged from 0.10 to 0.14 ml/h kg, and t 1/2 ranged from 2.2 to 2.9 weeks. No PSA reductions ≥50% were observed. Six patients (46%) had radiographically stable disease, lasting a median of 24 weeks.
Conclusion
AGS-1C4D4 was well-tolerated and demonstrated linear PK. Despite preclinical differences in antibody-dependent cellular cytotoxicity, AGS-1C4D4 and AGS-PSCA have similar safety and PK profiles. The recommended Phase II dose is 48 mg/kg.
Similar content being viewed by others

Introduction
The recent clinical success of therapeutic monoclonal antibodies has made them one of the most rapidly expanding classes of antineoplastic agents. Prostate cancer is particularly well suited for antibody-based therapy because it possesses several tumor-associated antigens, and because of the lack of necessity to avoid targeting the normal prostate (a non-essential organ). These properties have helped fuel the development of a number of therapeutic monoclonal antibodies directed against multiple prostate cancer-associated target antigens [1]. To this end, an ideal therapeutic target would be one that demonstrated strong homogeneous expression in advanced and metastatic disease, was minimally expressed in normal tissues, and was implicated in disease pathogenesis and progression. One such tumor target is prostate stem cell antigen (PSCA).
PSCA is a glycosylphosphatidylinositol (GPI)-linked cell-surface protein that was cloned in lymph node-derived prostate cancer xenografts [2]. The literature suggests that it is expressed in >80% of prostate cancers [3–5], as well as in the normal genitourinary tract and stomach. Although PSCA expression has been detected in all stages of prostate cancer, increased levels have been associated with higher Gleason score and advanced stage [3], biochemical recurrence [4], metastatic progression [5], and transition to the castration-resistant state [3]. In preclinical experiments, administration of murine anti-PSCA monoclonal antibodies to mice bearing human prostate cancers led to inhibition of tumor growth and metastasis formation as well as prolonged survival in these animals [6]. This was true both for bone metastasis-derived and lymph node-derived xenografts, and for non-castrate as well as castration-resistant tumors.
These in vivo data provided the stimulus for the generation of AGS-PSCA, a high-affinity fully human IgG-κ monoclonal antibody against PSCA produced in mouse hybridoma cell culture [1]. In mouse models, AGS-PSCA was shown to inhibit the growth of non-castrate as well as castration-resistant prostate tumors grown subcutaneously or orthotopically, while synergism was demonstrated when this agent was combined with docetaxel in patient-derived murine prostate tumor xenografts [7]. Mechanistically, AGS-PSCA was found to induce antibody-dependent cell-mediated cytotoxicity in PSCA-expressing tumor cells but not in cancer cells lacking PSCA expression. In addition, AGS-PSCA was able to mediate complement-dependent cytotoxicity in PSCA-expressing cancer cells. These antitumor effects of AGS-PSCA led to the initiation of a Phase I clinical trial evaluating this agent as monotherapy in 47 men with advanced castration-resistant prostate cancer [8]. In that dose-escalation study, AGS-PSCA was administered by intravenous infusion over 1–2 h every 3 weeks for four doses in cohorts of 3–6 patients at 1, 3, 5, 10, 20, and 40 mg/kg and a final expanded cohort (n = 18) of a loading dose of 40 mg/kg followed by repeated doses of 20 mg/kg. AGS-PSCA was shown to be safe and was not associated with any grade ≥3 drug-related adverse events or dose-limiting toxicities. However, hybridoma-derived AGS-PSCA did not yield sufficient drug quantities to enable large-scale clinical trials or allow drug commercialization; therefore, an alternative production method was sought.
AGS-1C4D4 is a fully human IgG-κ anti-PSCA monoclonal antibody produced in Chinese hamster ovary (CHO) cells, containing the same amino acid sequence as the hybridoma-derived AGS-PSCA. Comparability data encompassing in vivo antitumor activity in orthotopic mouse models, tissue cross-reactivity analyses, as well as toxicological and pharmacokinetic studies in cynomolgus monkeys have all demonstrated the equivalence of AGS-1C4D4 and AGS-PSCA. However, because of differences in glycosylation patterns and in vitro antibody-dependent cellular cytotoxicity between the two agents, the US FDA requested that a limited rapid dose-escalation Phase I study of intravenous AGS-1C4D4 be conducted in men with metastatic castration-resistant prostate cancer, to confirm the safety and PK results observed in the larger Phase I trial of AGS-PSCA. Thus, a small rapid dose-escalation study was conducted. The overall objectives of the current study were to characterize the safety, tolerability, and pharmacokinetic profile of AGS-1C4D4 in this patient population and to define the recommended Phase II dose of this agent.
Patients and methods
Patients
Subjects were recruited from the outpatient medical oncology clinics of the Johns Hopkins Sidney Kimmel Comprehensive Cancer Center (Baltimore, MD) and the Memorial Sloan-Kettering Cancer Center (New York, NY). Participants were required to have histologically confirmed prostate adenocarcinoma, with metastatic castration-resistant disease, and demonstration of disease progression after receipt of all available standard therapies (or after declining or not being suitable for standard therapy). Other eligibility criteria included age ≥18, Eastern Cooperative Oncology Group performance status <2, and adequate bone marrow, renal, hepatic, and coagulation parameters. Exclusion criteria included receipt of any anticancer therapy within 4 weeks of study entry, administration of an investigational drug or device within 30 days of study entry, use of an anti-androgen within 6 weeks of study entry, known hypersensitivity to components of the study drug or its analogs, active central nervous system involvement, current evidence of major medical illness including clinically significant cardiac disease, known psychiatric or substance abuse disorder, and active infectious illness (including HIV and hepatitis B/C). Eligible participants were required to provide written informed consent, and the protocol and consent form were approved by the institutional review boards at each center.
Study design
This was a first-in-human, Phase I, open-label, rapid dose-escalation study conducted at two member institutions of the Department of Defense (DOD)/Prostate Cancer Foundation (PCF)—Prostate Cancer Clinical Trials Consortium (PCCTC). AGS-1C4D4 was administered as a single intravenous infusion every 3 weeks for four planned doses (over 12 weeks). Subjects were enrolled sequentially to receive AGS-1C4D4 at doses of 6, 12, 24, and 48 mg/kg (cohorts 1–4). Drug infusions lasted 60 min (dose cohorts 1–3) or 120 min (dose cohort 4, with the exception of one patient who received a 60-min infusion). If a subject had a dose-limiting toxicity (DLT) at any time during the study, AGS-1C4D4 treatment would be discontinued in that subject. A DLT was defined as any grade ≥3 adverse event considered to be related to the study drug, any infusion reaction necessitating drug discontinuation, any other drug-related adverse event leading to study drug discontinuation, or any toxicity lasting ≥3 weeks. Adverse events were graded according to the NCI Common Toxicity Criteria version 3.0. After the 12-week planned treatment period, patients who demonstrated stable disease or objective tumor responses could continue AGS-1C4D4 at the same dose and schedule until disease progression, unmanageable drug-related toxicity, or withdrawal of consent.
Dose-escalation parameters were as follows. At dose levels 1 and 2 (6 and 12 mg/kg), a minimum of one and two patients were required to enroll, respectively. At either of these dose levels, if a grade ≥2 drug-related toxicity occurred, that dose level would be expanded to a minimum of three patients and all subsequent dose levels would enroll a minimum of three patients each. At dose levels 3 and 4 (24 and 48 mg/kg), a minimum of three patients were required to enroll in each. At a given dose level, rules for dose advancement were as follows. If there were no DLTs at that dose level, advancement to the next dose level would be permitted. If one DLT was observed, at least three more subjects would be enrolled to that dose level; if none of these three new subjects experienced a DLT, then the next dose cohort would be opened, but if ≥1 DLT was observed then dose escalation would be stopped. In any dose cohort, the occurrence of ≥2 DLTs would necessitate halting further dose escalation. Intra-patient dose escalation was not permitted.
In light of structural similarities between AGS-PSCA and AGS-1C4D4 and based on preclinical data from both agents, as well as safety and pharmacokinetic data from the Phase I study with AGS-PSCA, it was felt that the dose-escalation schema for AGS-1C4D4 should closely approximate that used in the AGS-PSCA Phase I study [8]. However, a notable difference between AGS-PSCA and AGS-1C4D4 is an approximate 2- to 3-fold increase in antibody-dependent cellular cytotoxicity. Considering this observation, the starting dose of AGS-1C4D4 in the current trial was chosen to be less than one-third of the well-tolerated AGS-PSCA dose of 48 mg/kg given every 3 weeks. Therefore, in the present study, AGS-1C4D4 was administered every 3 weeks at doses ranging from 6 to 48 mg/kg. The exact accelerated titration design and starting dose and schedule were also pursued after recommendation and agreement from the FDA.
The maximum tolerated dose (MTD) of AGS-1C4D4 would be defined as the dose level immediately below the dose level at which ≥2 subjects experienced a DLT. In the absence of a readily identifiable MTD, dose escalation would be allowed to proceed until dose cohort 4 had enrolled to completion. If cohort 4 was found to be safe and well tolerated, dose escalation would stop and a dose at or below this level would be selected for future use in Phase II trials.
Patient evaluation
At baseline, participants underwent a history and physical examination, an electrocardiogram (ECG), a complete blood count, routine serum chemistries, coagulation studies, and serum prostate specific antigen (PSA) measurement. Safety assessments were performed at weeks 1, 2, 3, 7, 14, and 21 and every 3 weeks thereafter. These safety evaluations consisted of history and physical examination, vital signs, serum chemistries and hematology, ECG (weeks 1 and 14 only), and urinalysis (weeks 1, 7, and 14 only). In addition, 4 weeks after the last infusion of the study drug, all subjects had a safety follow-up visit. PSA measurements were obtained every 3 weeks while on study. Disease assessments were conducted approximately every 12 weeks and included review of clinical symptoms as well as radiographic (CT and bone scan) evaluations.
To assess for anti-AGS-1C4D4 antibodies, serum samples were collected at baseline, every 3 weeks for the first 12 weeks on study, and at the safety follow-up visit. Antibody titers were determined using a screening electrochemiluminescence assay followed by a confirmatory immunodepletion assay.
Pharmacokinetics
Pharmacokinetic (PK) analysis involved measurement of serum levels of the therapeutic monoclonal antibody (AGS-1C4D4) using a quantitative sandwich enzyme-linked immunosorbent assay (Alta Analytical Laboratory, San Diego, CA). PK sampling was performed at baseline and at 2, 4, 6, 8, 24, 48, and 72 h after the first study drug infusion, and at 7, 14, and 21 days after first drug infusion. Thereafter, PK measurements were conducted every 3 weeks (pre-dose, i.e., trough levels), and also at the safety follow-up visit. The PK variables of interest included minimum and maximum observed serum concentrations (C min, C max) of AGS-1C4D4, time to maximum serum concentration (T max), area under the serum concentration–time curve (AUC), systemic clearance (CL), volume of distribution at steady state (V ss), and serum half-life within dosing interval (t 1/2).
The PK time points were selected based on PK data obtained from preclinical studies with AGS-PSCA and AGS-1C4D4, and the Phase I dose-escalation study with AGS-PSCA [8]. The primary purpose of obtaining PK in the present study was to ensure there were no notable differences in the PK of AGS-1C4D4 compared to AGS-PSCA.
Statistical analysis
The primary endpoint of this study was to characterize the safety and tolerability of AGS-1C4D4 in men with metastatic castration-resistant prostate cancer, as assessed by incidence and severity of adverse events (including serious adverse events and DLTs). Secondary endpoints were to determine the pharmacokinetic features of intravenously administered AGS-1C4D4 and to assess for human anti-human antibody responses against AGS-1C4D4.
Up to 18 subjects could have been enrolled in the study. The exact number of subjects was dependent upon the number of dose levels tested before the MTD was established. With six subjects treated at the identified MTD level or in the absence of a readily identifiable MTD at dose level 4, the upper bound of the 80% confidence interval for the DLT rate at that dose level would exclude a rate of 33% if no patients developed DLTs. If there were no DLTs in the six subjects that were treated at dose levels 1–3, the upper bound of the 80% confidence interval for the DLT rate at those dose levels would exclude a rate of 25%.
Patient demographics and other baseline characteristics were summarized using conventional descriptive statistics (mean, standard deviation, standard error, median, range). Descriptive statistics were also used to summarize adverse events; this was done separately by dose cohort and overall. Adverse events were assigned a grade, as well as their potential relationship to the study drug. Serious adverse events, DLTs, those leading to treatment discontinuation, and those resulting in death were considered separately. Pharmacokinetic parameters were analyzed using non-compartmental models. Descriptive statistics were generated for C min, C max, AUC, and t 1/2. The number and percentage of subjects developing anti-AGS-1C4D4 antibodies were tabulated.
Tumor assessments based on CT scans were summarized according to RECIST [9] using the following categories: complete response, partial response, stable disease, and progressive disease. Bone scan assessments were categorized as disease regression, stable disease, and progressive disease. For PSA measurements, descriptive statistics were used to summarize baseline values and changes from baseline at each study visit. The maximum percent change in PSA was calculated for each patient. The percentage of subjects with a 25 or 50% decline in PSA from baseline was also tabulated. PSA doubling time (PSADT) and PSA velocity were estimated for each patient before and during treatment with the study drug. PSADT was defined as the natural log of 2 divided by the slope of the linear regression line of the natural log of PSA against time (in months) [10]. PSA velocity was defined as the slope of the linear regression line of PSA (in the natural scale) against time (in months) [11]. Differences in within-subject changes in PSADT and PSA velocity (before and during treatment) were assessed using paired Student’s t tests.
Statistical analyses were performed using SAS version 9.1 (SAS Institute Inc, Cary, North Carolina, USA). All P values were two-sided, and statistical significance was set at P < 0.05.
Results
Patient characteristics
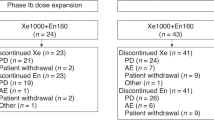
Between March 2008 and September 2009, thirteen patients were enrolled in the study: five at the Johns Hopkins Sidney Kimmel Comprehensive Cancer Center and eight at the Memorial Sloan-Kettering Cancer Center. All 13 subjects received at least one dose of AGS-1C4D4 and all were evaluable for safety and efficacy (Fig. 1). One patient was treated at the first dose level (6 mg/kg), two patients were treated at the second dose level (12 mg/kg), three patients were treated at the third dose level (24 mg/kg), and seven patients were treated at the fourth dose level (48 mg/kg). Nine subjects (69%) completed all four planned infusions of AGS-1C4D4 over 12 weeks, while four subjects (31%) did not achieve the full duration of treatment. Of those that came off study early, three discontinued therapy due to disease progression and one discontinued due to physician discretion. Five men extended treatment beyond four cycles, as permitted per protocol. Of these, four subjects eventually discontinued therapy due to disease progression and one subject withdrew consent. Overall, the median number of AGS-1C4D infusions was four (range, 3–12). No subject discontinued treatment due to an adverse event.

CONSORT diagram
Baseline demographic and clinical characteristics are summarized in Table 1. All subjects were white, and more than half were over the age of 75. Most patients had a Gleason sum of seven or less, and the type of primary therapy was divided evenly between prostatectomy and radiation. Two-thirds of participants had both bone metastases and soft tissue involvement. All subjects had developed castration resistance at the time of study entry and had received androgen suppression for a median of 4.3 years (range, 0.4–11.0 years). Over half of subjects had previously been treated with chemotherapy for metastatic disease; all but one had received docetaxel. The median time interval between the last chemotherapy dose and study entry was 2.2 months (range, 0.9–35.9 months).
Safety
All subjects experienced at least one on-study adverse event. These are listed in Table 2, stratified by dose cohort, and summarized overall. The most common adverse events (occurring in >15% of patients) were fatigue, arthralgia, constipation, abdominal pain/discomfort, chest pain, diarrhea, musculoskeletal pain, and nausea. All except for one of these events (an occurrence of chest pain) were grade-1/2 toxicities. Only five adverse events were considered to be related to AGS-1C4D4: four cases of fatigue and one case of fever. Four grade-3 toxicities were reported: these included chest pain, cellulitis of the scrotum/perineum, acute gallstone pancreatitis, and generalized rash. None of these grade-3 adverse events were considered to be related to AGS-1C4D4. There were no grade-4 toxicities, no dose-limiting toxicities, no infusion-related reactions, and no fatal events.
AGS-1C4D4 antibodies
Serum samples from all 13 participants were analyzed for the presence of anti-AGS-1C4D4 antibodies. Although three patients tested positive by the electrochemiluminescence assay (the screening test), confirmation using the immunodepletion assay was not achieved in any of these patients. Therefore, none of the study subjects had measurable antibody titers against AGS-1C4D4.
Pharmacokinetic results
Serum AGS-1C4D4 pharmacokinetic analyses were performed on all 13 subjects (Table 3). The results of these studies can be summarized as follows. Linear PK were observed across all examined doses (6, 12, 24, and 48 mg/kg). The peak serum AGS-1C4D4 concentration (C max) was attained at the end of each intravenous infusion and declined biphasically thereafter (Fig. 2). The final elimination phase was characterized by a slow clearance rate (CL) and a long terminal half-life (t 1/2). Median CL values for the four dose levels ranged from 0.10 to 0.15 ml/h-kg, and the t 1/2 ranged from 1.9 to 2.9 weeks.

Serum concentration–time curves after intravenous administration of AGS-1C4D4 at each dose level. Data are shown as means ± one standard error. The y-axis is in the log scale
The volume of distribution of AGS-1C4D4 at steady state (V ss) was approximately the same as the plasma volume, suggesting that the therapeutic monoclonal antibody was not widely distributed outside the systemic circulation. Median V ss ranged from 48 to 74 ml/kg. Systemic exposure of AGS-1C4D4, as indicated by AUC(0−∞) and C max, increased proportionally with dose: a doubling in dose resulted in a 2-fold increase in AUC and a 2-fold increase in C max. An every-3-week dose schedule resulted in systemic accumulation of AGS-1C4D4. Steady state levels were attained by around week 10 to week 19, with an approximate accumulation ratio at steady state ranging from 2 to 3. The observed time-to-steady-state was about five times the t 1/2 of AGS-1C4D4.
Clinical responses
A waterfall plot showing best PSA response (maximum decrease in PSA from baseline or minimum increase if no decrease was observed) is depicted in Fig. 3. Five subjects (38%) demonstrated PSA reductions on study, but only two of these (15%) were substantial declines (one was a 47% PSA reduction and the other was a 44% decline). Interestingly, both of these patients were treated on the 12 mg/kg cohort. No subject achieved a ≥50% PSA reduction at any time during the study. Across all cohorts, the median time to best PSA response was 6.1 weeks (range, 3.1–16.1 weeks), and by 24 weeks after study entry all patients had experienced PSA elevations.

Waterfall plot showing best PSA response at any time compared to baseline. *24 mg/kg dose cohort, †48 mg/kg dose cohort
The effect of the study drug on PSA kinetic parameters measured before and after study entry was also assessed. Median pre-treatment PSADT was 2.4 months, while post-treatment PSADT was 6.8 months. This change was not statistically significant (difference: +4.4 months, P = 0.15). Median pre-treatment log PSA velocity was 0.0010 ng/ml/month, while post-treatment log PSA velocity was 0.0042 ng/ml/month. This change was also not statistically significant (difference: +0.0032 ng/ml/month, P = 0.79).
In terms of tumor evaluations, 11 subjects had bone metastases at baseline (although 1 patient never had a subsequent bone scan) and 10 subjects had soft tissue metastases at baseline. Among those with bone lesions, 5 patients (50%) had progressive disease and 5 patients (50%) had stable disease for ≥12 weeks. Among those with soft tissue lesions, 4 patients (40%) had progressive disease and 6 patients (60%) had stable disease for ≥12 weeks. No objective tumor responses were observed. Overall, 6/13 subjects (46%) had stable radiographic disease lasting ≥12 weeks and 7/13 subjects (54%) had tumor progression in bone and/or soft tissue lesions.
Discussion
AGS-1C4D4 is an anti-PSCA monoclonal antibody produced in Chinese hamster ovary (CHO) cells that harbors the same amino acid sequence as mouse hybridoma-derived AGS-PSCA. Although comparability data encompassing amino acid sequence, in vivo preclinical antitumor activity, tissue cross-reactivity, and a head-to-head comparison of pharmacokinetics in cynomolgus monkeys demonstrated that the two agents were similar, there were differences in glycosylation patterns and in vitro antibody-dependent cellular cytotoxicity between the two compounds. As such, there was a possibility that the behavior of the two agents in humans may have differed. For this reason, a separate rapid dose-escalation Phase I trial of AGS-1C4D4 was conducted as requested by the FDA to evaluate safety, tolerability, and pharmacokinetics. The results of the present study using AGS-1C4D4 confirmed that there are no notable differences in the safety, PK, or antitumor effects between the two therapeutic antibodies.
Our study demonstrated that AGS-1C4D4 is a safe and well-tolerated agent that was associated with only a few grade 1–2 drug-related adverse events (namely fatigue and fever), but no dose-limiting toxicities or infusion reactions. It did not result in production of detectable anti-AGS-1C4D4 antibodies. A maximum tolerated dose was not reached. The recommended Phase II dose for AGS-1C4D4 is 48 mg/kg, based on the established safety of this regimen. An alternative Phase II dosing regimen, based on the established safety in an expanded dose cohort in the Phase I AGS-PSCA [8], is a loading dose of 48 mg/kg followed by an every-3-weeks dose of 24 mg/kg.
Intravenous infusion of AGS-1C4D4 given every 3 weeks was associated with linear pharmacokinetics and a long terminal half-life. Fifteen percent of patients (2/13) achieved ≥25% reductions in PSA compared to baseline, and on-study median PSA doubling time was non-significantly increased compared to pre-study values. Forty-six percent of men (6/13) had radiographic evidence of stable disease lasting ≥12 weeks. These results are comparable to those seen in the prior phase I study using AGS-PSCA in a similar patient population [8]. Importantly, despite preclinical differences in antibody-dependent cellular cytotoxicity, AGS-1C4D4 and AGS-PSCA have similar safety and PK profiles.
The use of PSCA-directed antibody-based therapies is a possible alternative for the treatment of advanced prostate cancer. Such therapies can either rely on inhibiting the function of the target antigen itself (in this case PSCA) using a naked antibody or may take advantage of a cell-surface antigen to deliver a payload by way of an antibody–drug conjugate. Evidence of the former is suggested by preclinical experiments showing that antitumor effects are still observed in preclinical systems when using anti-PSCA antibodies that are incapable of mediating complement-dependent or antibody-dependent cytotoxicity [12]. The payload approach (whereby an anti-PSCA monoclonal antibody would be conjugated to a chemotherapeutic or radiotherapeutic agent) would be most effective if the target antigen was preferentially expressed in tumor tissue over normal tissues and if the target was internalized after antibody binding. This strategy has not yet been tested in human clinical trials.
Because PCSA expression on tumor tissues may be required for the therapeutic effect of AGS-1C4D4, confirming the presence of PSCA on patient tumor samples through immunohistochemical staining or by other methods may optimize patient selection for future clinical trials. Indeed, such analyses may even be possible using circulating tumor cells, avoiding the need for tissue biopsies. In addition, pharmacodynamic studies to assay antigen-dependent cellular cytotoxicity may help to confirm whether the antitumor mechanism of this agent in humans mirrors that seen in animal models.
Therefore, one way to reasonably move forward with this agent could be to test AGS-1C4D4 as a monotherapy at the 48 mg/kg dose in a conventional single-arm phase II trial, but only in men with PSCA-expressing prostate cancers. Alternatively, a new phase I/II study to establish the optimal safe dosing of AGS-1C4D4 in combination with docetaxel chemotherapy in men with chemotherapy-naïve castration-resistant prostate cancer would also be a rational approach, borrowing from preclinical data showing synergism with this combination in mouse xenograft models [7]. However, it is sobering to note that, to date, no experimental drug has been shown to improve the efficacy of docetaxel in definitive randomized trials.
In addition to being found in prostate cancer, PSCA expression has also been reported in a substantial proportion of urothelial and pancreatic cancers [13, 14]. To this end, further development of AGS-1C4D4 either as monotherapy or in combination with conventional chemotherapy could also focus on these other tumor types. As proof of this concept, a Phase II study of AGS-1C4D4 in combination with gemcitabine is currently underway in patients with metastatic pancreatic cancer. However, a more rational drug development approach would focus only on patients whose tumors have been shown to express PSCA, in an attempt to enrich for patients that may derive the largest benefit from PSCA-directed therapies.
In conclusion, AGS-1C4D4 is a safe and well-tolerated agent and has a predictable pharmacokinetic profile. A dose of 48 mg/kg given by intravenous infusion every 3 weeks is recommended for future trials. Such trials do not need to be limited to prostate cancer patients, but confirmation of tumor PSCA expression is likely to increase the therapeutic yield of this agent. Using this platform to develop chemoimmunoconjugates or radioimmunoconjugates remains an exciting possibility for the future.
References
Jakobovits A (2008) Monoclonal antibody therapy for prostate cancer. Handb Exp Pharmacol 181:237–256
Reiter RE, Gu Z, Watabe T et al (1998) Prostate stem cell antigen: a cell surface marker overexpressed in prostate cancer. Proc Natl Acad Sci USA 95:1735–1740
Gu Z, Thomas G, Yamashiro J et al (2000) Prostate stem cell antigen (PSCA) expression increases with high Gleason score, advanced stage and bone metastases in prostate cancer. Oncogene 19:1288–1296
Han KR, Seligson DB, Liu X et al (2004) Prostate stem cell antigen expression is associated with Gleason score, seminal vesicle invasion and capsular penetration in prostate cancer. J Urol 171:1117–1121
Lam JS, Yamashiro J, Shintaku IP et al (2005) Prostate stem cell antigen is overexpressed in prostate cancer metastases. Clin Cancer Res 11:2591–2596
Saffran DC, Raitano AB, Hubert RS et al (2001) Anti-PSCA monoclonal antibodies inhibit tumor growth and metastasis formation and prolong the survival of mice bearing human prostate cancer xenografts. Proc Natl Acad Sci USA 98:2658–2663
Jakobovits A, Gudas JM, Jia X et al (2005) Therapeutic potential of AGS-PSCA: a fully human monoclonal antibody to prostate stem cell antigen (PSCA) for the treatment of prostate and pancreatic cancers. J Clin Oncol 23(Suppl): abstract 4722
Morris MJ, Eisenberger MA, Pili R et al (2009) Phase Ib study of AGS-PSCA, an anti-PSCA human antibody, in castration-resistant prostate cancer. Genitourinary Cancers Symposium: abstract 174
Therasse P, Arbuck SG, Eisenhauer EA et al (2000) New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst 92:205–216
Pound CR, Partin AW, Eisenberger MA et al (1999) Natural history of progression after PSA elevation following radical prostatectomy. JAMA 281:1591–1597
D’Amico AV, Chen MH, Roehl KA et al (2004) Preoperative PSA velocity and the risk of death from prostate cancer after radical prostatectomy. N Engl J Med 351:125–135
Gu Z, Yamashiro J, Kono E et al (2005) Anti-prostate stem cell antigen monoclonal antibody 1G8 induces cell death in vitro and inhibits tumor growth in vivo via a Fc-independent mechanism. Cancer Res 65:9495–9500
Amara N, Palapattu GS, Schrage M et al (2001) Prostate stem cell antigen is overexpressed in human transitional cell carcinoma. Cancer Res 61:4660–4665
Argani P, Rosty C, Reiter RE et al (2001) Discovery of new markers of cancer through serial analysis of gene expression: prostate stem cell antigen is overexpressed in pancreatic adenocarcinoma. Cancer Res 61:4320–4324
Acknowledgments
This work was supported by Agensys Inc., a wholly owned subsidiary of Astellas Pharmaceutical Inc. Additional support was provided by the Department of Defense Prostate Cancer Clinical Trials Consortium (grants PC051382, W81XWH-06-1-0241, W81XWH-08-PCRP-CCA) and by the National Cancer Institute (grants K23CA102544, 5P30CA006973).
Conflicts of interest
ESA, MAE, SRD, SFS, and HIS indicate no potential conflicts of interest. KJM and MEV are employees of Agensys Inc. MAC and MJM have received research funding from Agensys Inc.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Antonarakis, E.S., Carducci, M.A., Eisenberger, M.A. et al. Phase I rapid dose-escalation study of AGS-1C4D4, a human anti-PSCA (prostate stem cell antigen) monoclonal antibody, in patients with castration-resistant prostate cancer: a PCCTC trial. Cancer Chemother Pharmacol 69, 763–771 (2012). https://doi.org/10.1007/s00280-011-1759-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-011-1759-9