
Abstract
Background
Abdominal gas gangrene caused by clostridia species is rare and usually associated with organ perforation, immune suppression, or advanced malignoma.
Case report
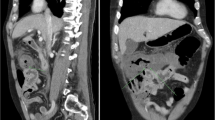
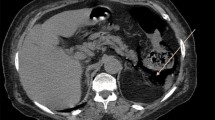
A 61-year-old man was admitted with severe back pain 1 day after uncomplicated colonoscopic polypectomy. With the exception of preexisting minor depression, the patient had been previously in excellent health. The computed tomography scan showed retroperitoneal emphysema in the left psoas muscle. During exploratory laparotomy, a spreading retroperitoneal phlegmon with pneumoretroperitoneum and a secondary peritonitis were found. A macroscopic perforation of the gut, particularly at the polypectomy sites was excluded. After the operation, the patient evolved in a septic shock condition and had pulmonary failure. Before hyperbaric oxygen therapy could be employed, the patient died. The autopsy showed a massive gas gangrene of the retroperitoneum caused by Clostridium perfringens, but no macroscopic bowel perforation was detected.
Results
This is the first report of a case of gas gangrene after uncomplicated polypectomy without macroscopic perforation in an otherwise healthy individual. A microperforation due to mucosal defect after polypectomy was most likely the entry point for the bacteria.
Conclusion
We conclude that clostridial myonecrosis should be considered in unclear abdominal infections, even if the patient’s history is not typical as in the present case.



Similar content being viewed by others

References
Pailler JL, Labeeu F (1986) Gas gangrene: a military disease? Acta Chir Belg 86(2):63–71 Mar–Apr
Sasaki T, Nanjo H, Takahashi M, Sugiyama T, Ono I, Masuda H (2000) Non-traumatic gas gangrene in the abdomen: report of six cases. J Gastroenterol 35(5):382–390
Bodey GP, Rodriguez S, Fainstein V, Elting LS (1991) Clostridial bacteremia in cancer patients. A 12-year experience. Cancer 67(7):1928–1942 (Apr 1)
Elliott D, Kufera JA, Myers RA (2000) The microbiology of necrotizing soft tissue infections. Am J Surg 179(5):361–366 (May)
Bennion RS, Thompson JE, Baron EJ, Finegold SM (1990) Gangrenous and perforated appendicitis with peritonitis: treatment and bacteriology. Clin Ther 12 [Suppl C]:31–44
Low DE, Shoenut JP, Kennedy JK, Sharma GP, Harding GK, Den Boer B, Micflikier AB (1987) Prospective assessment of risk of bacteremia with colonoscopy and polypectomy. Dig Dis Sci 32(11):1239–1243 (Nov)
Jamieson NF, Willoughby CP (2001) Gas gangrene after colonoscopy. Postgrad Med J 77(903):47–49 (Jan)
Anderson CM, Kerby JD, Perry WB, Sorrells DL (2004) Pneumoretroperitoneum in two patients with Clostridium perfringens necrotizing pancreatitis. Am Surgeon 70(3):268–271 (Mar)
Vellar DJ, Vellar ID, Pianta RM (1976) Traumatic retroperitoneal rupture of the duodenum. Aust N Z J Surg 46(3):206–208 (Aug)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Boenicke, L., Maier, M., Merger, M. et al. Retroperitoneal gas gangrene after colonoscopic polypectomy without bowel perforation in an otherwise healthy individual: report of a case. Langenbecks Arch Surg 391, 157–160 (2006). https://doi.org/10.1007/s00423-005-0019-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-005-0019-z