
Abstract
Background and aims
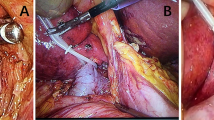
Bleeding from the hepatic vein is closely related to central venous pressure (CVP). To evaluate the effect of low central venous pressure during a hepatectomy, the infrahepatic inferior vena cava (IVC) was half clamped.
Patients and methods
Between 2006 and 2007, 20 patients undergoing major hepatectomy with the IVC half clamping (half-clamping group) were compared with 58 patients undergoing hepatectomy without IVC half clamping between 2003 and 2005 (control group). The types of liver resection, amount of blood loss during the hepatectomy, volume of blood transfusion, length of hospital stay, and complications were compared between the two groups.
Results
In the half-clamping group, blood loss was decreased in comparison to the control group (p = 0.041) and the suprahepatic CVP was low (2.4 ± 1.8 mmHg; p = 0.0002). The diameter at the root of the right hepatic vein was reduced in comparison to before clamping (5.8 ± 1.6 mm; p < 0.001). There were no complications of half clamping on any hemodynamic and blood electrolytic parameters.
Conclusion
Using the half clamping technique of the IVC, intra-operative CVP was maintained below 3 mmHg without any side effects, and the low CVP significantly reduced the bleeding from hepatic veins during a major hepatectomy.
Similar content being viewed by others

References
Azoulay D, Eshkenazy R, Andreani P, Castaing D, Adam R, Ichai P, Naili S, Vinet E, Saliba F, Lemoine A, Gillon MC, Bismuth H (2005) In situ hypothermic perfusion of the liver versus standard total vascular exclusion for complex liver resection. Ann Surg 241:277–285
Batignani G, Zuckermann M (2005) Inferior approach for the isolation of the left-middle hepatic veins in liver resections: a safe way. Arch Surg 140:68–971
Smyrniotis V, Arkadopoulos N, Kostopanagiotou G, Farantos C, Vassiliou J, Contis J, Karvouni E (2005) Sharp liver transection versus clamp crushing technique in liver resections: a prospective study. Surgery 137:306–311
Smyrniotis VE, Kostopanagiotou GG, Gamaletsos EL, Vassiliou JG, Voros DC, Fotopoulos AC, Contis JC (2002) Total versus selective hepatic vascular exclusion in major liver resections. Am J Surg 183:173–178
Melendez JA, Arslan V, Fischer ME, Wuest D, Jarnagin WR, Fong Y, Blumgart LH (1998) Perioperative outcomes of major hepatic resections under low central venous pressure anesthesia: blood loss, blood transfusion, and the risk of postoperative renal dysfunction. J Am Coll Surg 187:620–625
Wang WD, Liang LJ, Huang XQ, Yin XY (2006) Low central venous pressure reduces blood loss in hepatectomy. World J Gastroenterol 12:935–939
Jones RM, Moulton CE, Hardy KJ (1998) Central venous pressure and its effect on blood loss during liver resection. Br J Surg 85:1058–1060
Chen H, Merchant NB, Didolkar MS (2000) Hepatic resection using intermittent vascular inflow occlusion and low central venous pressure anesthesia improves morbidity and mortality. J Gastrointest Surg 4:162–167
Rees M, Plant G, Wells J, Bygrave S (1996) One hundred and fifty hepatic resections: evolution of technique towards bloodless surgery. Br J Surg 83:1526–1529
Hasegawa K, Takayama T, Orii R, Sano K, Sugawara Y, Imamura H, Kubota K, Makuuchi M (2002) Effect of hypoventilation on bleeding during hepatic resection: a randomized controlled trial. Arch Surg 137:311–315
Uchiyama K, Ueno M, Hama T, Kawai M, Tani M, Terasawa H, Ozawa S, Uemura R, Nakase T, Yamaue H (2005) Recurrence of primary hepatocellular carcinoma after hepatectomy—differences related to underlying hepatitis virus species. Hepatogastroenterology 52:591–595
Figueras J, Llado L, Ruiz D, Ramos E, Busquets J, Rafecas A, Torras J, Fabregat J (2005) Complete versus selective portal triad clamping for minor liver resections: a prospective randomized trial. Ann Surg 241:582–590
Chen H, Sitzmann JV, Marcucci C, Choti MA (1997) Acute isovolemic hemodilution during major hepatic resection—an initial report: does it safely reduce the blood transfusion requirement. J Gastrointest Surg 1:461–466
MacKenzie S, Dixon E, Bathe O, Sutherland F (2005) Intermittent hepatic vein—total vascular exclusion during liver resection: anatomic and clinical studies. J Gastrointest Surg 9:658–666
Yin ZY, Wang XM, Yu RX, Zhang BM, Yu KK, Li N, Li JS (2003) Total vascular exclusion technique for resection of hepatocellular carcinoma. World J Gastroenterol 9:2194–2197
Otsubo T, Takasaki K, Yamamoto M, Katsuragawa H, Katagiri S, Yoshitoshi K, Hamano M, Ariizumi S, Kotera Y (2004) Bleeding during hepatectomy can be reduced by clamping the inferior vena cava below the liver. Surgery 135:67–73
Fan ST, Lo CM, Liu CL, Lam CM, Yuen WK, Yeung C, Wong J (1999) Hepatectomy for hepatocellular carcinoma: toward zero hospital deaths. Ann Surg 229:322–330
Chau GY, Lui WY, King KL, Wu CW (2005) Evaluation of effect of hemihepatic vascular occlusion and the Pringle maneuver during hepatic resection for patients with hepatocellular carcinoma and impaired liver function. World J Surg 29:1374–1383
Haghighi KS, Wang F, King J, Daniel S, Morris DL (2005) In-line radiofrequency ablation to minimize blood loss in hepatic parenchymal transection. Am J Surg 190:43–47
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Uchiyama, K., Ueno, M., Ozawa, S. et al. Half clamping of the infrahepatic inferior vena cava reduces bleeding during a hepatectomy by decreasing the central venous pressure. Langenbecks Arch Surg 394, 243–247 (2009). https://doi.org/10.1007/s00423-008-0297-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-008-0297-3