
Abstract
Converging lines of evidence suggest that AKT1 is a major mediator of the responses to insulin, insulin-like growth factor 1 (IGF1), and glucose. AKT1 also plays a key role in the regulation of both muscle cell hypertrophy and atrophy. We hypothesized that AKT1 variants may play a role in the endophenotypes that make up metabolic syndrome. We studied a 12-kb region including the first exon of the AKT1 gene for association with metabolic syndrome-related phenotypes in four study populations [FAMUSS cohort (n = 574; age 23.7 ± 5.7 years), Strong Heart Study (SHS) (n = 2,134; age 55.5 ± 7.9 years), Dynamics of Health, Aging and Body Composition (Health ABC) (n = 3,075; age 73.6 ± 2.9 years), and Studies of a Targeted Risk Reduction Intervention through Defined Exercise (STRRIDE) (n = 175; age 40–65 years)]. We identified a three SNP haplotype that we call H1, which represents the ancestral alleles at the three loci and H2, which represents the derived alleles at the three loci. In young adult European Americans (FAMUSS), H1 was associated with higher fasting glucose levels in females. In middle age Native Americans (SHS), H1 carriers showed higher fasting insulin and HOMA in males, and higher BMI in females. In older African-American and European American subjects (Health ABC) H1 carriers showed a higher incidence of metabolic syndrome. Homozygotes for the H1 haplotype showed about twice the risk of metabolic syndrome in both males and females (p < 0.001). In middle-aged European Americans with insulin resistance (STRRIDE) studied by intravenous glucose tolerance test (IVGTT), H1 carriers showed increased insulin resistance due to the Sg component (p = 0.021). The 12-kb haplotype is a risk factor for metabolic syndrome and insulin resistance that needs to be explored in further populations.
Similar content being viewed by others

Introduction
AKT1 [also called protein kinase B (PKB)] is involved in two major signaling pathways: the regulation of muscle hypertrophy and atrophy (Nader 2005) and AKT1 is mediator of the biological functions of insulin and augments glucose uptake in muscle, adipocytes and liver along with a host of other tissues (Elghazi et al. 2006; Zdychova and Komers 2005). AKT1 mediates glucose uptake by inducing translocation of vesicles containing GLUT4 from intracellular stores to the plasma membrane (Hajduch et al. 1998). Briefly, upon insulin stimulation, AKT1 agonists activate receptor kinase functions that result in the stimulation of tyrosine phosphorylation of substrates such as IRS1 (Sun et al. 1991) and IRS2 (Sun et al. 1995). Tyrosyl phosphorylation of the IRSs provides binding sites for specific proteins containing Src-homology 2 (SH2) domains such as PI3K. PI3K is responsible for the insulin stimulation of GLUT4, the major insulin-regulated glucose transporter from intracellular vesicles to the plasma membrane in insulin-sensitive cells (Frevert et al. 1998).
In order to look at the function of AKT1 in pancreatic beta cells, researchers over-expressed constitutively active AKT1 in the β-cells of mice resulting in augmented β-cell mass by an increase in proliferation and cell size (Bernal-Mizrachi et al. 2001; Tuttle et al. 2001), and resistance to streptozotocin-induced diabetes (Bernal-Mizrachi et al. 2001; Tuttle et al. 2001). Mice with reduced Akt/Pkb activity in β-cells exhibited normal β-cell mass but defective insulin secretion (Bernal-Mizrachi et al. 2004), and increased susceptibility to developing glucose intolerance and diabetes following fat feeding (Bernal-Mizrachi et al. 2004). The roles of AKT1 as a key mediator in both muscle hypertrophy and atrophy and insulin signaling and glucose uptake indicate that this gene may play a role in a metabolic phenotypes, specifically the endophenotypes that together lead to metabolic syndrome.
Thus, we studied the AKT1 gene as a candidate for metabolic syndrome features. We hypothesized that the use of a young adult population would increase sensitivity for detection of these phenotypes, as all are well-documented to be age-related. Further, each phenotype has many potential environmental influences (lifestyle, training, diet), thus we hypothesize that a college-age population might have fewer potential confounders (Thompson et al. 2004; Uthurralt et al. 2007; Zoeller et al. 2007).
Here, we report the AKT1 haplotype structure, including a relatively small region of 12 kb with two predominant haplotypes (H1 and H2) upstream and inclusive of the first exon of the AKT1 gene. We evaluated a hap-tag SNP (rs1130214) in three population-based cohorts (FAMUSS, SHS, Health ABC), and one cohort focused on insulin resistance and response to training (STRRIDE) (Harris et al. 2005; Lee et al. 1990; Slentz et al. 2007; Thompson et al. 2004). We show that the H1 12 kb AKT1 haplotype is significantly associated with higher fasting serum glucose levels, and an increased risk for developing metabolic syndrome.
Participants and methods
Subject populations
FAMUSS population
The study design of the FAMUSS Study has been reported (Thompson et al. 2004). Briefly, 574 volunteers (18–41 years; mean 23.7 ± 5.7) were enrolled into a unilateral supervised 12-week resistance training intervention of the non-dominant arm. Quantified phenotypes included baseline blood pressure, height and weight and serum measurements including HDL, total cholesterol, fasting glucose, fasting insulin, and triglycerides. A dichotomous characterization of metabolic syndrome was defined as fulfilling at least three of the five criteria proposed by NCEP (2001). These criteria include an elevated waist circumference, triglycerides, blood pressure, fasting glucose and reduced HDL cholesterol. Because the FAMUSS Study did not collect waist circumference measurements, an elevated BMI (>25) was used as a surrogate.
Strong Heart Study
The SHS is a study of CVD and its risk factors among American Indian men and women (Lee et al. 1990). Briefly, DNA and serum measurements were collected on 2,134 volunteers (45–75 years; mean 55.5 ± 7.9). Quantified phenotypes included baseline blood pressure, height and weight and serum measurements including HDL, total cholesterol, fasting glucose, fasting insulin, triglycerides and incidence of metabolic syndrome.
Health ABC Study
Health ABC is a longitudinal study of body composition in older men and women with goals of identifying the clinical conditions that accelerate changes in and examining the health impact of these changes on the diseases of old age (Visser et al. 1999). Briefly, DNA and serum measurements were collected on 3,075 volunteers (68–80 years; mean 73.6 ± 2.9). Quantified phenotypes included baseline blood pressure, height and weight and serum measurements including HDL, total cholesterol, fasting glucose and fasting insulin. Triglycerides and incidence of metabolic syndrome and diabetes were classified as dichotomous phenotypes using NCEP ATP III criteria.
STRRIDE Study
The STRRIDE Study is a controlled study designed to measure the effect of exercise on abdominal fat. Briefly, 175 overweight individuals, male and female, aged 40–65 years were assigned an 8-month exercise regimen. All participants had mild to moderate lipid abnormalities. They were randomly assigned to one of three exercise groups: (1) high amount/vigorous intensity (65–80% of peak oxygen consumption), (2) low amount/vigorous intensity (65–80% of peak oxygen consumption), and (3) low amount/moderate intensity (40–55% of peak oxygen consumption). Quantified phenotypes included tomography scans of abdominal fat, BMI measures, Sg (glucose-stimulated glucose-release), insulin sensitivity index (ISI) and acute insulin response to glucose (AIRg).
Phenotype measures for FAMUSS Study
Serum measurements were made from stored fasting sera and plasma from each subject (baseline). Measurements: fasting glucose, fasting insulin, C-reactive protein and lipid panel (triglycerides and HDL). All measurements were made by Quest Diagnostics (Chantilly VA).
SNP discovery
SNPs for each exon, exon/intron boundaries, and 10 kb upstream (5′) to the AKT1 gene were identified by screening a panel of 96 ethnically diverse genomic DNA samples with denaturing high performance liquid chromatography (Transgenomic WAVE system, Transgenomic, USA) and automated sequencing (Applied Biosystems 3100 Genetic Analyzer). Polymorphisms were tested for allele frequency, and cross-referenced to dbSNP (http://www.dbSNP.org) and HapMap (http://www.hapmap.org) data resources. Twelve SNPs were studied in depth, selected based upon allele frequency and linkage disequilibrium testing. The published sensitivity of DHPLC for SNP detection is 96% (Jones et al. 1999). However, to reach that level of SNP detection requires optimal temperature selection and possibly primer redesign (Jones et al. 1999). For this publication, we cannot be certain that we did not miss additional variation in the AKT1 regions that we scanned due to the level of sensitivity of this technique. In addition, DHPLC suffers from the inability to discover homozygote changes and would require mixing of a sample with a known sequence to all scanned samples for the discovery of homozygous changes (Mogensen et al. 2003). DHPLC Novel SNPs not in dbSNP or HapMap databases were submitted to dbSNP. A list of the SNPs studied and their respective dbSNP identifiers (including those submitted to dbSNP) can be found in Table 1.
Genotyping
Genotyping was done using a novel TaqMan allele discrimination assay that employs the 5′ nuclease activity of Taq polymerase to detect a fluorescent reporter signal generated during PCR reactions (see Supplemental Table 1). Both alleles were detected simultaneously using allele-specific oligonucleotides labeled with different fluorophores, and genotypes determined by the ratio of the two fluorophores used. Allele-specific PCR reactions for each SNP included 10 ng genomic DNA, 900 nM forward and reverse PCR primers, 200 nM fluorescent allele discrimination probes (common allele FAM labeled; rare allele VIC labeled) and TaqMan® Universal PCR Master Mix, No AmpErase® UNG [Applied Biosystems (ABI), Foster City, CA, USA] in a final volume of 10 μl. The PCR and fluorescent ratio profile was done using 10 min at 95°C (denaturation), and 44 cycles of 15 s at 92°C and 1 min at an annealing temperature of 60°C. Reactions were set up using a MWG robot, and fluorescence ratios and allele calling done using an ABI 7900.
Linkage disequilibrium
Pair-wise tests for linkage disequilibrium were done for all 12 AKT1 polymorphisms using the correlation coefficient (R) on each pair-wise combination in the 1,078 FAMUSS subjects. A haplotype minimization algorithm contained within the PHASE v 2.1 program (Stephens et al. 2001) was then used to establish haplotypes from these data.
Statistical methods
Hardy–Weinberg equilibrium was determined for each SNP using a χ 2 test to compare the observed genotype frequencies to those expected under H–W equilibrium. All genotyped SNPs were in H–W equilibrium.
All metabolic syndrome-related phenotypes were analyzed as either continuous quantitative traits (triglycerides, fasting glucose, etc.) or as dichotomous traits (metabolic syndrome and high/low triglyceride level). Normality of each quantitative trait was confirmed using the Shapiro–Wilk normality test.
Bivariate correlation analyses of each quantitative measurement showed several significant correlations with age and baseline mass; therefore, associations between each SNP and quantitative phenotype were assessed using analysis of covariance (ANCOVA) methods. Due to large gender differences all analyses were performed separately for males and females.
Each ANCOVA used a dominant genetic model statistically comparing the group of homozygous wild-type individuals to the group of heterozygous and homozygous mutant individuals.
Linear regression analysis, including likelihood ratio tests between full (containing genotype and covariates) and constrained (containing covariates only) models, were performed to estimate the proportion of variance in volumetric measurements attributable to each SNP’s genotype. For dichotomous traits, logistic regression models adjusted for age and baseline body mass were used. A nominal p value of 0.05 was defined as significant and all statistical analyses were performed using Stata V.8 (StataCorp, College Park, TX).
Results
SNP discovery and haplotypes of AKT1
SNPs for each exon, exon/intron boundaries, and 10 kb upstream (5′) to the AKT1 gene (Genbank NM_001014431.1) were identified by screening a panel of 96 ethnically diverse genomic DNA samples with denaturing high performance liquid chromatography and automated sequencing. We identified 12 SNPs in AKT1, 7 of which were intragenic and 5 of which were upstream of the gene. A list of the SNPs studied and their respective dbSNP identifiers (including three novel SNPs submitted to dbSNP) can be found in Table 1.
The SNPs were genotyped in the FAMUSS population (Table 2) to identify regions that showed strong linkage disequilibrium to test in additional populations. Two major haplotype blocks were identified, one including most of the coding region of the gene and one 12 kb haplotype upstream of AKT1 inclusive of the first exon, haplotype H1/H2. The H1/H2 haplotype is composed of SNPs: rs1130214, rs10141867 and rs33925946. The H1 haplotype alleles are GCC for those three SNPs; the H2 haplotype alleles are TTA for those three SNPs (on the plus strand DNA). LD plots were generated showing the extent of LD between the SNPs listed in Table 1. The SNPs of haplotype H1/H2 are shown in red text. The amount of LD between any two SNPs (plotted on the X and Y axis) as determined by the correlation coefficient R is shown on a color scale from blue to red. Blue equals r 2 of zero, or no LD; red equals r 2 of 1 or perfect LD (Fig. 1). SNP rs10138227 shows some LD with the other three but it is not strong enough to include as part of the haplotype. From this work, we chose to analyze rs1130214 as a hap-tag SNP representing a 12 kb haplotype covering the first intron/10 kb upstream.

Linkage disequilibrium among AKT1 SNPs within the FAMUSS population and SHS. Linkage disequilibrium is plotted for African-Americans, Asians and European Americans of the FMS cohort. The LD was calculated between each pair of SNPs using the r 2 measurement and haplotype frequencies were estimated using the online program PHASE, which uses genotype data to determine the phase of the chromosomes and thus haplotype structure and frequency. The SNPs from Table 1 are plotted on the X and Y axes. A color scale is then used to plot the LD between any two SNPs. Blue equals an r 2 of zero, red equals an r 2 of 1.0. The SNPs of H1/H2 are in red text. All three of the SNPs are in high LD with each other as shown by the red blocks
Associations between AKT1 and the FAMUSS, Strong Heart Study, Health ABC and STRRIDE studies
We used the young adult FAMUSS population to screen for associations between the AKT1 gene polymorphisms of the H1/H2 haplotype and metabolic syndrome endophenotypes: increased adiposity, increased blood pressure, low serum HDL, insulin resistance and fasting glucose levels, with subsequent validation of associations in additional population-based cohorts (SHS, Health ABC) and in the insulin resistant population STRRIDE (demographics of these four populations are shown in Tables 2, 3, 4, 5).
The SNP association analyses were done with both heterozygotes (GT) and homozygotes for the T allele (TT) in the same group because the number of TT individuals was too low in some groups to see an effect. Therefore, the analyses are interpreted as associations with at least one copy of the T allele (H2) versus homozygotes for the G allele (H1).
The H1/H2 hap-tag SNP rs1130214 was associated with fasting glucose only in females and this SNP contributed 1.3% to genotypic variance (Table 6). SNP rs1130214 causes a G to T change (representing the H1 and H2 haplotypes, respectively). With at least one copy of the T allele, females had lower values of fasting glucose (GG, N = 201; 86.22 ± 0.50 mg/dL vs. GT/TT, N = 178; 84.55 ± 0.53 mg/dL; p = 0.0236). This SNP did not have any associations with any metabolic syndrome endophenotypes in males in the FAMUSS Study.
We then used rs1130214 as a hap-tag SNP, and genotyped both Strong Heart Study (Table 3) and Health ABC (Table 4) to test for any associations with metabolic phenotypes in older cohorts. For the older and more heterogeneous Strong Heart Study population of Native Americans, rs1130214 showed association with 2-h glucose, fasting insulin, triglycerides, and the HOMA measure of insulin resistance in males (Table 7). The T allele was associated with lower 2 h glucose levels (GG, N = 434; 180.69 ± 5.11 mg/dL vs. GT/TT, N = 147; 160.01 ± 8.77 mg/dL; p = 0.0422) and lower fasting insulin (GG, N = 564; 19.44 ± 0.68 μIU/mL vs. GT/TT, N = 208; 16.21 ± 1.12 μIU/mL; p = 0.0136). In addition, in males, the T allele was associated with a lower HOMA value (GG, N = 559; 7.52 ± 0.32 vs. GT/TT, N = 203; 6.15 ± 0.53; p = 0.267).
In male participants in the Health ABC Study, the T allele of rs1130214 was associated with lower fasting glucose (GG, N = 661; 110.5 ± 1.4 mg/dL vs. GT/TT, N = 798; 106.4 ± 1.3 mg/dL; p = 0.0305) (Table 8). This effect was also seen in African-Americans males (GG, N = 205; 116.8 ± 2.9 mg/dL vs. GT/TT, N = 328; 107.7 ± 2.3 mg/dL; p = 0.0170). These results are not significant after correction for multiple testing (p < 0.007); however, the statistical community is divided on correction methods for multiple testing since the Bonferonni correction may be too harsh and thus increasing false negatives (Rice et al. 2008).
Taken together, associations from all three population-based cohorts suggested that the AKT1 upstream haplotype was a determinant of insulin resistance, resulting in higher circulating glucose and/or insulin with apparent age- and sex-dependence.
Associations between AKT1 rs1130214 and the Health ABC Study for metabolic syndrome
The five commonly accepted endophenotypes of metabolic syndrome are: increased insulin resistance or fasting glucose plasma levels (>100 mg/dl), increased adiposity (central obesity or BMI > 30), elevated triglycerides (equal to or greater than 150 mg/dL), increased blood pressure (>130mmHg/85mmHg), and low serum HDL (<40–50 mg/dl) (Alberti et al. 2006; Alberti and Zimmet 1998; Grundy et al. 2004; NCEP 2001). To determine if the H1/H2 haplotype is a major determinant of metabolic syndrome diagnosis, we studied the Health ABC population. This population-based study had a diagnosis of T2D as an exclusion criterion, with excellent phenotyping of metabolic syndrome endophenotypes in a tightly restricted age range (Harris et al. 2005).
The incidence of metabolic syndrome showed a significant association with rs1130214 in the Health ABC population (Table 9). The analysis was done for both heterozygotes (GT) and homozygotes for the T allele (TT) because the number of TT individuals was too low for some groups to determine any effect. We saw strong effects with having at least one copy of the T allele suggesting that haplotype H2 strongly influences these phenotypes even in the presence of one copy of the H1 haplotype (represented by the G allele). Individuals with at least one copy of the T allele were much less likely to have metabolic syndrome, consistent with the lower insulin resistance observed with the T allele (H2) in all three cohorts. This was true for the entire Health ABC cohort (GT/TT: OR = 0.765, p = 0.001) and all males (GT/TT: OR = 0.650, p < 0.001). There was a significant effect in all females for the TT individuals only (TT, OR = 0.577; p = 0.005). The T allele showed a very strong protective effect in African-American males (GT, OR = 0.539; p = 0.007). These results are significant after correction for multiple testing (p < 0.007).
Associations between rs1130214 and the STRRIDE Study for glucose-stimulated glucose-release (Sg) levels
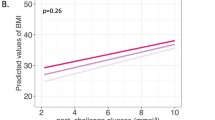
The STRRIDE Study is a cohort of insulin-resistant middle-aged adults. The H2 haplotype (the T allele of rs1130214) was associated with higher Sg in European American males (TT, p = 0.021) (Table 10). This is consistent with the other cohorts and H2 associations with insulin resistance phenotypes and even protection against metabolic syndrome, which often follows the development of insulin resistance. There were no significant associations (denoted as NS) with any other group of this cohort (Table 10).
Discussion
We defined the haplotype structure of the AKT1 gene and studied 12 representative SNPs in a young adult population to identify genetic predispositions to endophenotypes of metabolic syndrome. We identified a relatively small 12 kb haplotype, defined by the SNPs rs1130214, rs10141867 and rs33925946, which are in very strong linkage disequilibrium in all populations studied. In the young adult population (FAMUSS Study), the ancestral haplotype of the 12 kb region (H1; tagged by rs1130214) was associated with higher fasting glucose in females (average age 24 years), suggesting that the 12 kb haplotype is associated with insulin resistance. We validated this finding first in an older and more heterogeneous Native American population (SHS; average age 56 years), where H1 had higher fasting serum glucose, higher serum insulin, and a higher HOMA value in males, all consistent with association with insulin resistance. Although we originally identified an association with fasting glucose levels in the FAMUSS females, we did not see this same association in the older females of the SHS or Health ABC. We then studied a cohort of aged African-American and European American (Health ABC; average age 73 years), and also found evidence for association with insulin resistance, where men with H1 showed higher fasting glucose.
Insulin resistance is one of the five key endophenotypes associated with T2D, and the precursor state of metabolic syndrome. The diagnosis of metabolic syndrome is made when a subject shows increased visceral adiposity, and two additional threshold phenotypes [increased insulin resistance, increased blood pressure, increased triglycerides (TGs), and low HDL serum levels]. Insulin resistance is a complex physiological and biochemical phenotype involving responses to increased serum glucose by the pancreas, muscle, and liver. The individual components of pancreas, muscle and liver can be resolved by an IVGTT. We studied the association of the 12 kb upstream haplotype with the IVGTT data from STRRIDE subjects with features of metabolic syndrome, and found evidence for association with the Sg phenotype. Thus, four distinct cohorts all validated association of the upstream AKT1 12 kb haplotype (H1) with increased insulin resistance; H2 associates with decreased insulin resistance.
Given the association of the 12 kb AKT1 upstream haplotype with measures of insulin resistance in four cohorts, we queried the association of the same haplotype with metabolic syndrome diagnosis. It is important to note that the H1 haplotype is the more common haplotype in all populations, and thus associations of a common haplotype with a rare trait become more challenging statistically. Of the four populations studied, only one was felt to be adequate for testing of metabolic syndrome associations, namely the Health ABC Study. The FAMUSS Study population was too young to have an appreciable incidence of metabolic syndrome. The Strong Heart Study was quite heterogeneous in age and showed a very high incidence of many comorbidities associated with metabolic syndrome. The STRRIDE Study was a non-population based study, where participants were recruited based upon having features of metabolic syndrome. However, the Health ABC Study was of large size (n = 3,000), with tightly restricted age (73.6 years), with metabolic syndrome as a key focus of the study. Genotyping of the upstream haplotype in Health ABC showed a very strong association with metabolic syndrome diagnosis (Table 9). Homozygotes for the ancestral H1 haplotype (GG) had double the risk of metabolic syndrome compared to those homozygous for the less common H2 haplotype (TT). This association was retained when the population was stratified by sex and ethnicity.
Along with protection from metabolic syndrome, the AKT1 H2 haplotype was associated with higher values of TGs in males in the SHS. This result is counterintuitive to the association of lower 2-h glucose, lower fasting insulin, and lower HOMA value. A current issue in genetics is the extension of associated loci discovered using genome-wide association studies (GWAS) in European ancestry to non-European individuals (Murray et al. 2010; Teslovich et al. 2010). For example, a recent study (Murray et al. 2010) examined SNPs for asthma risk in two African ancestry groups that were located near a gene encoding ORMDL3 (17q21) that was identified for asthma risk in individuals with European-descent (Moffatt et al. 2007). The SNPs near the ORMDL3 gene did not replicate risk for asthma in the African ancestry groups (Murray et al. 2010). Concurrently, another study focusing on the genetics of blood lipids found 24 of 27 SNPs replicated for TG values between European-descent and South Asians, a replication of 26 of 28 SNPs for TG values in East Asians, and a replication of 24 of 30 SNPs for TG values in African-Americans (Teslovich et al. 2010). These results speak of the difficulty that exists in understanding genetic variation and its relationship to different phenotypes in different ethnic groups. The higher TG values associated with H2 haplotype in the SHS may be due an interaction with the lack of access to medications that can control lipids (Stern 1998) and genotype. Finally, there is an ongoing unfavorable increase in the prevalence of hypertension, low HDL, and diabetes mellitus in the aging survivors of the SHS and this will likely lead to further increases in CVD morbidity and mortality. This interaction between AKT1 H2 and TG will need to be further explored in additional populations.
To our knowledge, the 12 kb haplotype described here is one of the strongest candidate gene studies for either insulin resistance or a metabolic syndrome diagnosis identified to date. In another report, we report function for all the SNPs in the associated haplotype (Harmon et al. 2010, submitted). In future studies, we will examine how this AKT1 haplotype impacts the effect on insulin resistance when combined with the numerous reported genome-wide association studies (GWAS) of isolated insulin resistance (Lyssenko et al. 2009), insulin response (Rich et al. 2009), fasting glucose (Bouatia-Naji et al. 2008; Dupuis et al. 2010; Prokopenko et al. 2009), glucose response (Saxena et al. 2010), and GWAS studies of the fully morbid T2D diagnosis (Wellcome Trust Case Control Consortium 2007; Rung et al. 2009; Saxena et al. 2007; Scott et al. 2007; Zeggini et al. 2008).
References
Alberti KG, Zimmet PZ (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 15:539–553
Alberti KG, Zimmet P, Shaw J (2006) Metabolic syndrome—a new world-wide definition. A consensus statement from the International Diabetes Federation. Diabet Med 23:469–480
Bernal-Mizrachi E, Wen W, Stahlhut S, Welling CM, Permutt MA (2001) Islet beta cell expression of constitutively active Akt1/PKB alpha induces striking hypertrophy, hyperplasia, and hyperinsulinemia. J Clin Investig 108:1631–1638
Bernal-Mizrachi E, Fatrai S, Johnson JD, Ohsugi M, Otani K, Han Z, Polonsky KS, Permutt MA (2004) Defective insulin secretion and increased susceptibility to experimental diabetes are induced by reduced Akt activity in pancreatic islet beta cells. J Clin Investig 114:928–936
Bouatia-Naji N, Rocheleau G, Van Lommel L, Lemaire K, Schuit F, Cavalcanti-Proenca C, Marchand M, Hartikainen AL, Sovio U, De Graeve F, Rung J, Vaxillaire M, Tichet J, Marre M, Balkau B, Weill J, Elliott P, Jarvelin MR, Meyre D, Polychronakos C, Dina C, Sladek R, Froguel P (2008) A polymorphism within the G6PC2 gene is associated with fasting plasma glucose levels. Science 320:1085–1088
Dupuis J, Langenberg C, Prokopenko I, Saxena R, Soranzo N, Jackson AU, Wheeler E, Glazer NL, Bouatia-Naji N, Gloyn AL, Lindgren CM, Magi R, Morris AP, Randall J, Johnson T, Elliott P, Rybin D, Thorleifsson G, Steinthorsdottir V, Henneman P, Grallert H, Dehghan A, Hottenga JJ, Franklin CS, Navarro P, Song K, Goel A, Perry JR, Egan JM, Lajunen T, Grarup N, Sparso T, Doney A, Voight BF, Stringham HM, Li M, Kanoni S, Shrader P, Cavalcanti-Proenca C, Kumari M, Qi L, Timpson NJ, Gieger C, Zabena C, Rocheleau G, Ingelsson E, An P, O’Connell J, Luan J, Elliott A, McCarroll SA, Payne F, Roccasecca RM, Pattou F, Sethupathy P, Ardlie K, Ariyurek Y, Balkau B, Barter P, Beilby JP, Ben-Shlomo Y, Benediktsson R, Bennett AJ, Bergmann S, Bochud M, Boerwinkle E, Bonnefond A, Bonnycastle LL, Borch-Johnsen K, Bottcher Y, Brunner E, Bumpstead SJ, Charpentier G, Chen YD, Chines P, Clarke R, Coin LJ, Cooper MN, Cornelis M, Crawford G, Crisponi L, Day IN, de Geus EJ, Delplanque J, Dina C, Erdos MR, Fedson AC, Fischer-Rosinsky A, Forouhi NG, Fox CS, Frants R, Franzosi MG, Galan P, Goodarzi MO, Graessler J, Groves CJ, Grundy S, Gwilliam R, Gyllensten U, Hadjadj S et al (2010) New genetic loci implicated in fasting glucose homeostasis and their impact on type 2 diabetes risk. Nat Genet 42:105–116
Elghazi L, Balcazar N, Bernal-Mizrachi E (2006) Emerging role of protein kinase B/Akt signaling in pancreatic beta-cell mass and function. Int J Biochem Cell Biol 38:157–163
Frevert EU, Bjorbaek C, Venable CL, Keller SR, Kahn BB (1998) Targeting of constitutively active phosphoinositide 3-kinase to GLUT4-containing vesicles in 3T3–L1 adipocytes. J Biol Chem 273:25480–25487
Grundy SM, Brewer HB Jr, Cleeman JI, Smith SC Jr, Lenfant C (2004) Definition of metabolic syndrome: report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 109:433–438
Hajduch E, Alessi DR, Hemmings BA, Hundal HS (1998) Constitutive activation of protein kinase B alpha by membrane targeting promotes glucose and system A amino acid transport, protein synthesis, and inactivation of glycogen synthase kinase 3 in L6 muscle cells. Diabetes 47:1006–1013
Harris SL, Gil G, Robins H, Hu W, Hirshfield K, Bond E, Bond G, Levine AJ (2005) Detection of functional single-nucleotide polymorphisms that affect apoptosis. Proc Natl Acad Sci USA 102:16297–16302
Jones AC, Austin J, Hansen N, Hoogendoorn B, Oefner PJ, Cheadle JP, O’Donovan MC (1999) Optimal temperature selection for mutation detection by denaturing HPLC and comparison to single-stranded conformation polymorphism and heteroduplex analysis. Clin Chem 45:1133–1140
Lee ET, Welty TK, Fabsitz R, Cowan LD, Le NA, Oopik AJ, Cucchiara AJ, Savage PJ, Howard BV (1990) The Strong Heart Study. A study of cardiovascular disease in American Indians: design and methods. Am J Epidemiol 132:1141–1155
Lyssenko V, Nagorny CL, Erdos MR, Wierup N, Jonsson A, Spegel P, Bugliani M, Saxena R, Fex M, Pulizzi N, Isomaa B, Tuomi T, Nilsson P, Kuusisto J, Tuomilehto J, Boehnke M, Altshuler D, Sundler F, Eriksson JG, Jackson AU, Laakso M, Marchetti P, Watanabe RM, Mulder H, Groop L (2009) Common variant in MTNR1B associated with increased risk of type 2 diabetes and impaired early insulin secretion. Nat Genet 41:82–88
Moffatt MF, Kabesch M, Liang L, Dixon AL, Strachan D, Heath S, Depner M, von Berg A, Bufe A, Rietschel E, Heinzmann A, Simma B, Frischer T, Willis-Owen SA, Wong KC, Illig T, Vogelberg C, Weiland SK, von Mutius E, Abecasis GR, Farrall M, Gut IG, Lathrop GM, Cookson WO (2007) Genetic variants regulating ORMDL3 expression contribute to the risk of childhood asthma. Nature 448:470–473
Mogensen J, Bahl A, Kubo T, Elanko N, Taylor R, McKenna WJ (2003) Comparison of fluorescent SSCP and denaturing HPLC analysis with direct sequencing for mutation screening in hypertrophic cardiomyopathy. J Med Genet 40:e59
Murray T, Beaty TH, Mathias RA, Rafaels N, Grant AV, Faruque MU, Watson HR, Ruczinski I, Dunston GM, Barnes KC (2010) African and non-African admixture components in African Americans and an African Caribbean population. Genet Epidemiol 34(6):561–568
Nader GA (2005) Molecular determinants of skeletal muscle mass: getting the “AKT” together. Int J Biochem Cell Biol 37:1985–1996
NCEP (2001) Executive summary of the third report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 285:2486–2497
Prokopenko I, Langenberg C, Florez JC, Saxena R, Soranzo N, Thorleifsson G, Loos RJ, Manning AK, Jackson AU, Aulchenko Y, Potter SC, Erdos MR, Sanna S, Hottenga JJ, Wheeler E, Kaakinen M, Lyssenko V, Chen WM, Ahmadi K, Beckmann JS, Bergman RN, Bochud M, Bonnycastle LL, Buchanan TA, Cao A, Cervino A, Coin L, Collins FS, Crisponi L, de Geus EJ, Dehghan A, Deloukas P, Doney AS, Elliott P, Freimer N, Gateva V, Herder C, Hofman A, Hughes TE, Hunt S, Illig T, Inouye M, Isomaa B, Johnson T, Kong A, Krestyaninova M, Kuusisto J, Laakso M, Lim N, Lindblad U, Lindgren CM, McCann OT, Mohlke KL, Morris AD, Naitza S, Orru M, Palmer CN, Pouta A, Randall J, Rathmann W, Saramies J, Scheet P, Scott LJ, Scuteri A, Sharp S, Sijbrands E, Smit JH, Song K, Steinthorsdottir V, Stringham HM, Tuomi T, Tuomilehto J, Uitterlinden AG, Voight BF, Waterworth D, Wichmann HE, Willemsen G, Witteman JC, Yuan X, Zhao JH, Zeggini E, Schlessinger D, Sandhu M, Boomsma DI, Uda M, Spector TD, Penninx BW, Altshuler D, Vollenweider P, Jarvelin MR, Lakatta E, Waeber G, Fox CS, Peltonen L, Groop LC, Mooser V, Cupples LA, Thorsteinsdottir U, Boehnke M, Barroso I et al (2009) Variants in MTNR1B influence fasting glucose levels. Nat Genet 41:77–81
Rice TK, Schork NJ, Rao DC (2008) Methods for handling multiple testing. Adv Genet 60:293–308
Rich SS, Goodarzi MO, Palmer ND, Langefeld CD, Ziegler J, Haffner SM, Bryer-Ash M, Norris JM, Taylor KD, Haritunians T, Rotter JI, Chen YD, Wagenknecht LE, Bowden DW, Bergman RN (2009) A genome-wide association scan for acute insulin response to glucose in Hispanic-Americans: the Insulin Resistance Atherosclerosis Family Study (IRAS FS). Diabetologia 52:1326–1333
Rung J, Cauchi S, Albrechtsen A, Shen L, Rocheleau G, Cavalcanti-Proenca C, Bacot F, Balkau B, Belisle A, Borch-Johnsen K, Charpentier G, Dina C, Durand E, Elliott P, Hadjadj S, Jarvelin MR, Laitinen J, Lauritzen T, Marre M, Mazur A, Meyre D, Montpetit A, Pisinger C, Posner B, Poulsen P, Pouta A, Prentki M, Ribel-Madsen R, Ruokonen A, Sandbaek A, Serre D, Tichet J, Vaxillaire M, Wojtaszewski JF, Vaag A, Hansen T, Polychronakos C, Pedersen O, Froguel P, Sladek R (2009) Genetic variant near IRS1 is associated with type 2 diabetes, insulin resistance and hyperinsulinemia. Nat Genet 41:1110–1115
Saxena R, Voight BF, Lyssenko V, Burtt NP, de Bakker PI, Chen H, Roix JJ, Kathiresan S, Hirschhorn JN, Daly MJ, Hughes TE, Groop L, Altshuler D, Almgren P, Florez JC, Meyer J, Ardlie K, Bengtsson Bostrom K, Isomaa B, Lettre G, Lindblad U, Lyon HN, Melander O, Newton-Cheh C, Nilsson P, Orho-Melander M, Rastam L, Speliotes EK, Taskinen MR, Tuomi T, Guiducci C, Berglund A, Carlson J, Gianniny L, Hackett R, Hall L, Holmkvist J, Laurila E, Sjogren M, Sterner M, Surti A, Svensson M, Tewhey R, Blumenstiel B, Parkin M, Defelice M, Barry R, Brodeur W, Camarata J, Chia N, Fava M, Gibbons J, Handsaker B, Healy C, Nguyen K, Gates C, Sougnez C, Gage D, Nizzari M, Gabriel SB, Chirn GW, Ma Q, Parikh H, Richardson D, Ricke D, Purcell S (2007) Genome-wide association analysis identifies loci for type 2 diabetes and triglyceride levels. Science 316:1331–1336
Saxena R, Hivert MF, Langenberg C, Tanaka T, Pankow JS, Vollenweider P, Lyssenko V, Bouatia-Naji N, Dupuis J, Jackson AU, Kao WH, Li M, Glazer NL, Manning AK, Luan J, Stringham HM, Prokopenko I, Johnson T, Grarup N, Boesgaard TW, Lecoeur C, Shrader P, O’Connell J, Ingelsson E, Couper DJ, Rice K, Song K, Andreasen CH, Dina C, Kottgen A, Le Bacquer O, Pattou F, Taneera J, Steinthorsdottir V, Rybin D, Ardlie K, Sampson M, Qi L, van Hoek M, Weedon MN, Aulchenko YS, Voight BF, Grallert H, Balkau B, Bergman RN, Bielinski SJ, Bonnefond A, Bonnycastle LL, Borch-Johnsen K, Bottcher Y, Brunner E, Buchanan TA, Bumpstead SJ, Cavalcanti-Proenca C, Charpentier G, Chen YD, Chines PS, Collins FS, Cornelis M, JC G, Delplanque J, Doney A, Egan JM, Erdos MR, Firmann M, Forouhi NG, Fox CS, Goodarzi MO, Graessler J, Hingorani A, Isomaa B, Jorgensen T, Kivimaki M, Kovacs P, Krohn K, Kumari M, Lauritzen T, Levy-Marchal C, Mayor V, McAteer JB, Meyre D, Mitchell BD, Mohlke KL, Morken MA, Narisu N, Palmer CN, Pakyz R, Pascoe L, Payne F, Pearson D, Rathmann W, Sandbaek A, Sayer AA, Scott LJ, Sharp SJ, Sijbrands E, Singleton A, Siscovick DS, Smith NL, Sparso T et al (2010) Genetic variation in GIPR influences the glucose and insulin responses to an oral glucose challenge. Nat Genet 42:142–148
Scott LJ, Mohlke KL, Bonnycastle LL, Willer CJ, Li Y, Duren WL, Erdos MR, Stringham HM, Chines PS, Jackson AU, Prokunina-Olsson L, Ding CJ, Swift AJ, Narisu N, Hu T, Pruim R, Xiao R, Li XY, Conneely KN, Riebow NL, Sprau AG, Tong M, White PP, Hetrick KN, Barnhart MW, Bark CW, Goldstein JL, Watkins L, Xiang F, Saramies J, Buchanan TA, Watanabe RM, Valle TT, Kinnunen L, Abecasis GR, Pugh EW, Doheny KF, Bergman RN, Tuomilehto J, Collins FS, Boehnke M (2007) A genome-wide association study of type 2 diabetes in Finns detects multiple susceptibility variants. Science 316:1341–1345
Slentz CA, Houmard JA, Johnson JL, Bateman LA, Tanner CJ, McCartney JS, Duscha BD, Kraus WE (2007) Inactivity, exercise training and detraining, and plasma lipoproteins. STRRIDE: a randomized, controlled study of exercise intensity and amount. J Appl Physiol 103:432–442
Stephens M, Smith NJ, Donnelly P (2001) A new statistical method for haplotype reconstruction from population data. Am J Hum Genet 68:978–989
Stern MP (1998) Invited commentary: cardiovascular mortality in American Indians: paradox explained? Am J Epidemiol 147:1009–1010
Sun XJ, Rothenberg P, Kahn CR, Backer JM, Araki E, Wilden PA, Cahill DA, Goldstein BJ, White MF (1991) Structure of the insulin receptor substrate IRS-1 defines a unique signal transduction protein. Nature 352:73–77
Sun XJ, Wang LM, Zhang Y, Yenush L, Myers MG Jr, Glasheen E, Lane WS, Pierce JH, White MF (1995) Role of IRS-2 in insulin and cytokine signalling. Nature 377:173–177
Teslovich TM, Musunuru K, Smith AV, Edmondson AC, Stylianou IM, Koseki M, Pirruccello JP, Ripatti S, Chasman DI, Willer CJ, Johansen CT, Fouchier SW, Isaacs A, Peloso GM, Barbalic M, Ricketts SL, Bis JC, Aulchenko YS, Thorleifsson G, Feitosa MF, Chambers J, Orho-Melander M, Melander O, Johnson T, Li X, Guo X, Li M, Shin Cho Y, Jin Go M, Jin Kim Y, Lee JY, Park T, Kim K, Sim X, Twee-Hee Ong R, Croteau-Chonka DC, Lange LA, Smith JD, Song K, Hua Zhao J, Yuan X, Luan J, Lamina C, Ziegler A, Zhang W, Zee RY, Wright AF, Witteman JC, Wilson JF, Willemsen G, Wichmann HE, Whitfield JB, Waterworth DM, Wareham NJ, Waeber G, Vollenweider P, Voight BF, Vitart V, Uitterlinden AG, Uda M, Tuomilehto J, Thompson JR, Tanaka T, Surakka I, Stringham HM, Spector TD, Soranzo N, Smit JH, Sinisalo J, Silander K, Sijbrands EJ, Scuteri A, Scott J, Schlessinger D, Sanna S, Salomaa V, Saharinen J, Sabatti C, Ruokonen A, Rudan I, Rose LM, Roberts R, Rieder M, Psaty BM, Pramstaller PP, Pichler I, Perola M, Penninx BW, Pedersen NL, Pattaro C, Parker AN, Pare G, Oostra BA, O’Donnell CJ, Nieminen MS, Nickerson DA, Montgomery GW, Meitinger T, McPherson R, McCarthy MI et al (2010) Biological, clinical and population relevance of 95 loci for blood lipids. Nature 466:707–713
Thompson PD, Moyna N, Seip R, Price T, Clarkson P, Angelopoulos T, Gordon P, Pescatello L, Visich P, Zoeller R, Devaney JM, Gordish H, Bilbie S, Hoffman EP (2004) Functional polymorphisms associated with human muscle size and strength. Med Sci Sports Exerc 36:1132–1139
Tuttle RL, Gill NS, Pugh W, Lee JP, Koeberlein B, Furth EE, Polonsky KS, Naji A, Birnbaum MJ (2001) Regulation of pancreatic beta-cell growth and survival by the serine/threonine protein kinase Akt1/PKBalpha. Nat Med 7:1133–1137
Uthurralt J, Gordish-Dressman H, Bradbury M, Tesi-Rocha C, Devaney J, Harmon B, Reeves EK, Brandoli C, Hansen BC, Seip RL, Thompson PD, Price TB, Angelopoulos TJ, Clarkson PM, Moyna NM, Pescatello LS, Visich PS, Zoeller RF, Gordon PM, Hoffman EP (2007) PPARalpha L162V underlies variation in serum triglycerides and subcutaneous fat volume in young males. BMC Med Genet 8:55
Visser M, Fuerst T, Lang T, Salamone L, Harris TB (1999) Validity of fan-beam dual-energy X-ray absorptiometry for measuring fat-free mass and leg muscle mass. Health, Aging, and Body Composition Study–Dual-Energy X-ray Absorptiometry and Body Composition Working Group. J Appl Physiol 87:1513–1520
Wellcome Trust Case Control Consortium (2007) Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature 447:661–678
Zdychova J, Komers R (2005) Emerging role of Akt kinase/protein kinase B signaling in pathophysiology of diabetes and its complications. Physiol Res 54:1–16
Zeggini E, Scott LJ, Saxena R, Voight BF, Marchini JL, Hu T, de Bakker PI, Abecasis GR, Almgren P, Andersen G, Ardlie K, Bostrom KB, Bergman RN, Bonnycastle LL, Borch-Johnsen K, Burtt NP, Chen H, Chines PS, Daly MJ, Deodhar P, Ding CJ, Doney AS, Duren WL, Elliott KS, Erdos MR, Frayling TM, Freathy RM, Gianniny L, Grallert H, Grarup N, Groves CJ, Guiducci C, Hansen T, Herder C, Hitman GA, Hughes TE, Isomaa B, Jackson AU, Jorgensen T, Kong A, Kubalanza K, Kuruvilla FG, Kuusisto J, Langenberg C, Lango H, Lauritzen T, Li Y, Lindgren CM, Lyssenko V, Marvelle AF, Meisinger C, Midthjell K, Mohlke KL, Morken MA, Morris AD, Narisu N, Nilsson P, Owen KR, Palmer CN, Payne F, Perry JR, Pettersen E, Platou C, Prokopenko I, Qi L, Qin L, Rayner NW, Rees M, Roix JJ, Sandbaek A, Shields B, Sjogren M, Steinthorsdottir V, Stringham HM, Swift AJ, Thorleifsson G, Thorsteinsdottir U, Timpson NJ, Tuomi T, Tuomilehto J, Walker M, Watanabe RM, Weedon MN, Willer CJ, Illig T, Hveem K, Hu FB, Laakso M, Stefansson K, Pedersen O, Wareham NJ, Barroso I, Hattersley AT, Collins FS, Groop L, McCarthy MI, Boehnke M, Altshuler D (2008) Meta-analysis of genome-wide association data and large-scale replication identifies additional susceptibility loci for type 2 diabetes. Nat Genet 40:638–645
Zoeller RF, Ryan ED, Gordish-Dressman H, Price TB, Seip RL, Angelopoulos TJ, Moyna NM, Gordon PM, Thompson PD, Hoffman EP (2007) Allometric scaling of biceps strength before and after resistance training in men. Med Sci Sports Exerc 39:1013–1019
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Devaney, J.M., Gordish-Dressman, H., Harmon, B.T. et al. AKT1 polymorphisms are associated with risk for metabolic syndrome. Hum Genet 129, 129–139 (2011). https://doi.org/10.1007/s00439-010-0910-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00439-010-0910-8