
Abstract
The aim of this study was to define the risk of developing Lyme borreliosis after a tick bite. A survey was conducted from 1993 to 1995 in the western part of Switzerland in a group of patients who presented for treatment of a recent tick bite. Only patients with negative serological tests (enzyme-linked fluorescent assay screening test, and IgG and IgM immunoblots) at the first consultation and for whom a second blood sample was available 2 months later were included in the study. Of the 376 patients included, 266 had no clinical manifestation (group 1) and 110 had a small local cutaneous reaction (<2 cm) (group 2). The tick was available for 160 patients. Seroconversion was observed in 4.5% of 376 patients, 3.4% in group 1 and 7.2% in group 2. Typical erythema migrans, confirmed by seroconversion, was observed in three of 376 (0.8%) patients, while five of 376 (1.3%) patients developed a skin lesion without seroconversion. No other clinical manifestation of Lyme borreliosis was observed among these 376 patients. Borrelia detection in ticks did not correlate significantly with the risk of Lyme borreliosis. In conclusion, the risk of developing Lyme borreliosis in western Switzerland after a tick bite is low, and therefore, prophylactic antibiotics are not required.
Similar content being viewed by others


Introduction
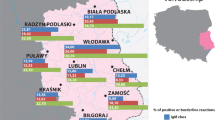
The risk of developing Lyme borreliosis after a tick bite depends on several factors, such as the geographical distribution of the tick population, the length of exposure to the tick, the rate of Borrelia burgdorferi infection in the tick population, and the species of tick that thrives in that region.
This risk is variable for a given individual in a region where Lyme borreliosis is considered endemic. As mentioned above, the risk depends on the duration of tick attachment [1]. In Europe, however, it was shown that the risk of transmission is high even after <24 h of tick attachment [2, 3]. Of course, the risk depends also on the frequency of contacts with tick biotopes, although the notion of tick biotopes is large (forests, riverbanks, lake borders, gardens, public parks).
In Switzerland, the principal vector of B. burgdorferi is a tick of the Ixodidae family, namely Ixodes ricinus, which is frequently found at altitudes of up to 800 m and is not found above 1,500 m. The infection rate of ticks with B. burgdorferi varies between 3% and 55% [4–7]. The rate varies in accordance with the region and with the developmental stage of the tick.
The seroprevalence of Lyme borreliosis is estimated at 26–35% [4, 8, 9, 10] in high-risk populations (forestry workers, military recruits, tour guides, etc.). However, the seroprevalence is not negligible in the general population, since a study showed a seroprevalence of 9% in a population of blood donors in Switzerland [11].
Despite the progress made in recent years in understanding Lyme borreliosis, diagnosis of the infection is not always straightforward. It is based primarily on clinical findings and the patient’s history, but serological tests remain essential, except in cases in which a typical erythema migrans (EM) is present. However, there is a lack of standardisation of the diagnostic methods, particularly in Europe, where five species of B. burgdorferi sensu lato coexist. This makes serological diagnosis difficult.
Switzerland is a region where Lyme borreliosis is endemic, and many questions raised by doctors encouraged us to carry out a prospective epidemiological study to evaluate the risk of developing Lyme borreliosis after a tick bite. To do so, we performed serological tests—enzyme-linked fluorescent assay (ELFA) and IgG and IgM immunoblots—on all sera at 2-month intervals in patients consulting for tick bites. Results were correlated with the presence of B. burgdorferi in the ticks attached to the patients.
Materials and methods
Study design
In 1993, upon a joint initiative by physicians, the University Hospital of Lausanne (Centre Hospitalier Universitaire Vaudois [CHUV]), the Central Institute of Valais Hospitals (Institut Central des Hôpitaux Valaisans [ICHV]) and the University of Neuchâtel a study in western Switzerland on tick bites and Lyme borreliosis was initiated. The study was conducted from June 1993 to December 1995. At the beginning of the study, clinical information on Lyme borreliosis, including pictures of skin lesions (typical EM and other cutaneous manifestations), were sent to all physicians, who were invited to notify us of all persons who presented for consultation about a tick bite. A questionnaire was filled out, and one blood sample was taken during the first consultation; the tick, if available, was also retained for testing. Two months later, a new questionnaire was filled out, and a second blood sample was taken.
The first questionnaire contained identification data of the patient (surname, first name, date of birth); comprehensive information about the tick bite together with the date of the bite, the geographical location of the patient at the time of the bite, whether the tick had been noticed by the doctor or by the patient, by whom the tick was extracted, and the estimation of the duration of tick attachment; a list of clinical manifestations (see definition below); the date of the onset and the duration of the clinical manifestations; and information about whether antibiotic treatment had been prescribed.
The second questionnaire was sent to the physicians along with the result of the first serological test. It contained information about the following: identification of the patient, any new tick bites since the previous consultation, the appearance of clinical manifestations since the first consultation or changes (if any) in the symptoms observed during the first consultation, and the administration of antibiotic treatment since the previous consultation.
Inclusion criteria
Only patients with a tick embedded in the skin at the time of the consultation or who remembered a recent tick bite were included. In addition, two blood samples were required, with an interval of about 2 months between sampling. The first serum had to be negative for anti-Borrelia antibodies (ELFA Vidas Lyme IgG–IgM screening test, and in-house IgG and IgM immunoblots). Patients were divided into two groups according to the clinical manifestations observed at the first visit: group 1, asymptomatic patients with no clinical manifestation after the tick bite; and group 2, patients with a local reaction (<2 cm) at the site of the tick bite.
Serum analyses
Samples were centrifuged at 3,500 rpm for 10 min. One millilitre of serum was collected in a sterile tube containing a preservative agent (mercurthiolate, 1:10,000 final concentration). All sera were screened for antibodies to B. burgdorferi sensu lato by an ELFA assay (Vidas Lyme IgG and IgM; bioMérieux, Marcy-l’Etoile, France). Tests were performed and interpreted according to instructions of the manufacturer.
All sera were also evaluated by in-house IgG and IgM immunoblots. The Borrelia isolate VS 102 (Borrelia garinii), used as antigen, was a low-passage strain (fewer than 8 passages in BSK-II medium) isolated from Ixodes ricinus ticks [7].
The sodium dodecyl sulfate-polyacrylamide gel electrophoresis and immunoblot assays were performed as described previously [12]. In short, the suspension of washed Borrelia (protein concentration of 1 mg/ml) was electrophoresed (constant voltage, 170 V) on a 12.5% polyacrylamide gel. A commercial standard (low-range-protein molecular weight standard; BioRad, Hercules, CA, USA) was used as reference for the calculation of relative molecular masses. The proteins were transferred by Western blot to polyvinylidene fluoride (Immobilon; Millipore, Kloten, Switzerland).
Immunoreactions were performed with human serum diluted 1:200. Fixed antibodies were revealed by a secondary antibody (anti-human IgG, γ-chain specific; or anti-human IgM, μ-chain specific) conjugated to alkaline phosphatase (Sigma, St Louis, MO, USA), followed by the addition of substrate BCIP/NBT (5-bromo-4-chloro-3-indoyl p-toluidine phosphate/p-nitro blue tetrazolium chloride) (Kirkegaard and Perry Lab., Gaithersburg, MD, USA).
The criterion for a positive immunoblot with human IgG was the appearance of a minimum of five bands, including flagellin and two of the following specific bands: OspC, OspA, p39, 93 kDa (p100). The criterion for positivity with human IgM was a minimum of four bands, including flagellin and one of the following specific bands: OspC, OspA, p39, 93 kDa (p100) (usually OspC).
Detection of Borrelia in ticks
Borrelia infection in ticks was detected using two methods. Ticks that were alive were examined by direct immunofluorescence and by polymerase chain reaction (PCR). Dead ticks were stored in alcohol and examined by PCR alone. Ticks were considered infected when borreliae were detected by at least one method.
Ticks that were alive were examined individually for B. burgdorferi using a direct immunofluorescence antibody test. Whole ticks were smeared on glass slides using a pair of tweezers. Preparations were dried for 10 h at 37°C and fixed in acetone for 10 min.
Slides were treated as described previously [13] using a fluorescein isothiocyanate-labelled conjugate prepared from pooled sera of patients with Lyme borreliosis [14]. Tick tissues were incubated in humid chambers for 30 min at 34°C. Slides were rinsed with phosphate-buffered saline (pH 7.3) and examined for spirochetes with an Olympus epifluorescence microscope at ×400 magnification.
After examination by immunofluorescent microscopy, smears of tick tissue were collected from the slides using sterile scalpels and placed in tubes containing 0.01 M Tris–HCl (pH 7.8) and 0.005 M EDTA. Proteinase K (Sigma) at a concentration of 300 μg/ml was added and maintained overnight at 55°C and then heated at 100°C for 10 min.
Ticks that had been stored in alcohol were dried and smeared on slides, and smears of tick tissue were collected from the slides and processed as described above.
B. burgdorferi sensu lato and genospecies primer sets were synthesized on a DNA synthesizer (Applied Biosystems, MWG-Biotech, Münchenstein, Switzerland). Primer sequences sensu lato 5′-AATAGGTCTAATAATAGCCTTAATAGC-3′ (forward primer) and 5′-CTAGTGTTTTGCCATCTTCTTTGAAAA-3′ (reverse primer) have been published by Demaerschalck et al. [15]. PCRs were performed with a DNA thermocycler (PTC-100TM; MJ Research, Watertown, MA, USA). Taq DNA polymerase (1.5 U) (Boehringer Mannheim Biochemica, Mannheim, Germany), the four deoxynucleotide triphosphates, 200 μM (dATP, dCTP, dGTP, and dTTP) (Sigma), and the reaction buffer (Boehringer Mannheim Biochemica) were used as recommended by the suppliers.
Twenty picomoles of each primer was used per 50 μl reaction mixture. PCR assays with sensu lato primers were run for 35 cycles under the following conditions: 1 min at 94°C, 1 min at 62°C, and 1 min at 72°C.
Estimation of feeding time
Duration of feeding time (tick attachment to the host) was empirically estimated by direct observation of the ticks by a technician (O.R.) experienced in feeding ticks on laboratory animals.
Statistical methods
Fisher’s exact test and calculation of the relative risk were used for data analysis.
Results
During the study period (June 1993 to December 1995), physicians in the western part of Switzerland reported a total of 1,272 patients who consulted for either a tick bite or for clinical manifestation suggestive of Lyme borreliosis. A total of 376 patients matched the criteria for inclusion in the study. The average age of the study population was 34 years (range, <1–81 years).
Of the 376 study patients, 266 had a tick bite without symptoms (group 1), and 110 had a tick bite with a small local reaction at the site of the tick bite (group 2). Ticks were obtained from 160 of 376 (43%) patients. One-third of the patients (124/376) recalled a previous tick bite.
Serology
At the second consultation 2 months after the first visit (range, 34–118 days), 17 (4.5%) patients showed seroconversion (Table 1): nine (3.4%) belonged to group 1 and eight (7.2%) belonged to group 2. Seroconversion was detected by ELFA in only eight of 17 (47%) patients. For the 15 of 17 (88%) patients whose seroconversion was detected by immunoblots, a rise in IgG was found in two patients, a rise in IgM in five patients, and a rise in both IgG and IgM in eight patients.
Clinical manifestations and treatment
During the 2-month study period, EM lesions were observed in three of 376 (0.8%) patients, all of whom seroconverted. When they entered the study, two of these three patients had a small local reaction and were included in group 2, and one was asymptomatic and was included in group 1. In addition, rash-like lesions were observed in five patients (1.3%) who did not seroconvert. When they entered the study, these five patients were asymptomatic and were included in group 1. These rash-like lesions were mostly large, red or purplish, and without annular lesion. No other clinical manifestations (neurological or articular symptoms) were observed among the 376 patients during the study period.
Of the eight patients who developed dermatological lesions during the study period, six received antibiotic treatment, including the three patients with EM. A preventive antibiotic treatment was administered to 36 of 376 patients during the first consultation, and none of them developed clinical manifestations during the study period.
Thus, a total of 42 of 376 patients were treated with antibiotics (amoxicillin, amoxicillin + clavulanic acid, ciprofloxacin, clarithromycin, cefuroxime, or doxycycline). Treatment duration varied from 3 to 35 days (mean, 11 days).
Tick analysis
Among ticks obtained from the 160 patients, one (0.6%) was a larva, 58 (36.3%) were nymphs, and 96 (60%) were adults. All belonged to Ixodes ricinus. Five (3.1%) additional ticks could not be identified (Fig. 1). Seventeen of the 160 ticks (11/96 adults and 6/58 nymphs) [(10%)] were infected, as determined by direct immunofluorescence and/or PCR. However, no spirochetal infection (direct immunofluorescence and/or PCR) was detected in ticks (n=6) collected from among patients who seroconverted (n=17).

Distribution of ticks, according to stage of development, brought by patients to the first consultation
Risk analysis
The relative risk (RR) of infection by B. burgdorferi, as evidenced by a seroconversion, was calculated (Table 2) in relation to bites of larval and nymphal ticks versus bites of adult ticks. Seroconversions were clearly increased when patients were exposed to nymph bites (RR=3.25 [0.61–17.22]). When the risk of seroconversion was considered in relation to the duration of tick attachment (<24 h vs ≧24 h), we observed a slightly increased risk with a higher duration of tick attachment (RR=1.26 [0.26–6.05], but the difference was not significant. In the present study, 35% of adult ticks were detected <24 h after attachment, whereas only 20% of nymphs were detected during this period of time. The feeding time of the ticks varied between <24 h and 7 days.
Discussion
Among the population studied, we observed a seroconversion rate of 4.5%. This level reached 3% in the group who had no clinical manifestation at the first consultation and who consulted for a tick bite and 7% in the group with a local cutaneous reaction at the first consultation. Lower levels of seroconversion have already been reported [16], as have higher levels [17]. The seroconversion level observed in our study is comparable with that found in a general population in Sweden (4.6%) [18]. Comparison of the different seroconversion levels should be done carefully. First, criteria for selection of patients differ from one study to another. Second, the observation periods were different (2 months between the 2 consultations in our study versus 6 months to 1 year in other studies). Third, various serological tests have been used in these studies. Indeed, several parameters may differ from one laboratory to another, including the Borrelia strains used as antigens, the methods employed to prepare the antigens, the reagents used, and the criteria for positivity [19–22].
In our study, immunoblots detected seroconversion in 88% (15/17) of patients who seroconverted, with the rise in IgM observed either alone or along with the rise in IgG. In the serological kinetics of Lyme borreliosis, IgM antibodies increase during the first 2–4 weeks, while IgG antibodies appear later. Using ELFA alone, seroconversion was detected in only 47% (8/17) of patients. This corroborates results from other studies showing that the sensitivity of the immunoblots for the detection of B. burgdorferi immunoglobulins is higher than that of enzyme immunoassays [23].
In Lyme borreliosis, EM is one of the earliest clinical manifestations after a tick bite. Among our patients, three of 376 (0.8%) developed a typical ring-like migrating rash accompanied by seroconversion, and 5 (1.3%) additional patients developed a rash or a rash-like lesion without seroconversion. We estimate that, of these five patients, one or two may have contracted Lyme borreliosis, since it is known that serological tests may be negative in about 20% of patients with Lyme borreliosis, even 2 months after a tick bite.
Globally, the risk of developing Lyme borreliosis after a tick bite is around 1%. In the group that seroconverted (n=17), the majority of patients (83%) remained symptom free, although EM was found in three of 17 (17%) patients. In the seronegative population, the frequency of true EM was relatively low compared to the 3.2% reported in the study of Nadelman et al. [24]. On the other hand, among patients who remained seronegative during the entire study, only five of 359 (1.3%) developed a rash. Thus, the difference between the two groups was highly significant (P=0.002). We may postulate that most of the rashes or rash-like lesions in the seronegative patients are probably due not to Borrelia but rather to some other pathogenic agent or allergens transmitted by Ixodes ricinus [25]. Of course, we know that serological investigation has an expected sensitivity of around 80% 2 months after a tick bite. No other clinical manifestation was observed during the 2-month period of observation. A preventive antibiotic treatment was administered to about 10% (36/376) of the patients at the first consultation. We, therefore, considered the problem of whether to administer systematic prophylactic treatment of a tick bite as proposed by some investigators [24].
The observation of a seroconversion without symptoms seems to be frequent in European Lyme borreliosis, which explains the relatively high level of seropositivity in populations in endemic areas in Europe and in populations at risk [9, 10]. However, one question persists: what happens to the patients in the long term? In some studies, it was hypothesized that serological positivity indicates a persistence of antibodies in a patient but does not prevent reinfection upon the development of an EM [26]. Furthermore, seropositivity does not indicate a higher risk of developing clinical manifestations [9, 27], but there is little information on the long-term follow-up of these patients.
In our study, we observed that in the seroconversion group, the proportion of nymphs was higher than that of adult ticks. This is in contrast to the serologically negative group, in which the proportion of adult ticks dominated. This is probably related to the smaller size of the nymphs, which allows them to feed longer before being noticed, which in turn increases the risk of Borrelia transmission [2, 3]. In the present study, 35% of adult ticks were detected <24 h after attachment, whereas only 20% of nymphs were detected during this period of time. Furthermore, the risk of being bitten by nymphs is increased because nymphs are 10–30 times more abundant in endemic areas than adult ticks [28], and therefore the frequency of humans bitten by nymphs should reflect this relative abundance [29]. In our study, most nymph bites were not detected or were considered not significant by some persons who had been bitten.
The prevalence of B. burgdorferi infection in ticks removed from the patients was only 10%, although we know that the infection rate in ticks collected from the vegetation in this area is 2–3 times higher (about 25% in nymphs, and 30% in adults) [4, 7, 30]. None of the six ticks removed from patients who seroconverted was found to be infected. One of the hypotheses could be that during the biting process, the tick may have injected the major portion or even all of its bacterial charge. It could also be a dilution factor, since the blood meal drastically decreases the sensitivity of the detection methods. Another hypothesis is that the tick found by the patient was not infected; instead, the infection was caused by a different tick bite that had gone unnoticed. It has been frequently reported that most tick bites remain unnoticed because of their small size and the painlessness of the bite itself.
In conclusion, the risk of developing Lyme borreliosis in western Switzerland after being bitten by a tick is low (0.8%), and prophylactic treatment after a tick bite is not recommended. Patients who present with a small local reaction have a tendency to undergo seroconversion twice as frequently as those who do not show any symptoms. In such cases, it is important to maintain a close follow-up of each patient, and if necessary, further treatment may be considered in accordance with the development of the lesion and the time interval between the tick bite and the consultation. In case of atypical clinical signs, it is advisable to perform two serological tests at an interval of 2–4 weeks and to confirm all equivocal or positive tests using an immunoblot. Although systematic antibiotic prophylaxis after a tick bite is not recommended, the development of a lesion typical of an EM requires immediate treatment, even before a serological test is performed.
References
Piesman J, Mather TN, Sinsky RJ, Spielman A (1987) Duration of tick attachment and Borrelia burgdorferi transmission. J Clin Microbiol 25:557–558
Kahl O, Gern L, Gray JS, Guy EC, Jongejan F, Kirstein F, et al (1998) Detection of Borrelia burgdorferi sensu lato in ticks: immunofluorescence assay versus polymerase chain reaction. Zentralblatt Bakteriol 287:205–210
Crippa M, Rais O, Gern L (2002) Investigations on the mode and dynamics of transmission and infectivity of Borrelia burgdorferi ss and Borrelia afzelii in Ixodes ricinus ticks. Vector Borne Zoonotic Dis 2:3–11
Aeschlimann A, Chamot E, Gigon F, Jeanneret JP, Kesseler D, Walther C (1987) B. burgdorferi in Switzerland. Zentralblatt Bakteriol [A] 263:450–458
Miserez V, Gern L, Aeschlimann A (1990) Borrelia burgdorferi in ticks of the Canton Tessin (Switzerland). Parasitology 32:293–299
Péter O (1990) Lyme borreliosis in the state of Valais, Switzerland. J Int Fed Clin Chem 2:121–124
Péter O, Bretz AG, Bee D (1995) Occurrence of different genospecies of Borrelia burgdorferi sensu lato in ixodid ticks of Valais, Switzerland. Eur J Epidemiol 11:463–467
Gern L, Frossard E et al (1989) Presence of antibodies against Borrelia burgdorferi in a population of the Swiss Plateau. Zentralblatt Bakteriol Suppl 18:321–328
Fahrer H, Sauvain MJ, Zhioua E, Van Hoecke C, Gern LE (1998) Longterm survey (7 years) in a population at risk for Lyme borreliosis: what happens to the seropositive individuals? Eur J Epidemiol 14:117–123
Fahrer H, van der Linden SM, Sauvain MJ, Gern L, Zhioua E, Aeschlimann A (1991) The prevalence and incidence of clinical and asymptomatic Lyme borreliosis in a population at risk. J Infect Dis 163:305–310
Nadal D, Wunderli W, Briner H, Hansen K (1989) Prevalence of antibodies to Borrelia burgdorferi in forestry workers and blood donors from the same region in Switzerland. Eur J Clin Microbiol Infect Dis 8:992–995
Péter O, Bretz AG, Postic P, Dayer E (1997) Association of distinct species of Borrelia burgdorferi sensu lato with neuroborreliosis in Switzerland. Clin Microbiol Infect 3:423–431
Gern L, Toutoungi LN, Hu CM, Aeschlimann A (1991) Ixodes (Pholeoixodes) hexagonus, an efficient vector of Borrelia burgdorferi in the laboratory. Med Vet Entomol 5:431–435
Peacock MG, Burgdorfer W, Ormsbee RA (1971) Rapid fluorescent antibody conjugation procedure. Infect Immun 3:355–357
Demaerschalck I, Ben Messaoud A, De Kesel M, Hoyois B, Lobet Y, Hoet P et al (1995) Simultaneous presence of different Borrelia burgdorferi genospecies in biological fluids of Lyme disease patients. J Clin Microbiol 33:602–608
Vos K, Van Dam AP, Kuiper H, Bruins H, Spanjaard L, Dankert J (1994) Seroconversion for Lyme borreliosis among Dutch military. Scand J Infect Dis 26:427–434
Rath PM, Ibershoff B, Mohnhaupt A, Albig J, Eljaschewitsch B, Jurgens D et al (1996) Seroprevalence of Lyme borreliosis in forestry workers from Brandenburg, Germany. Eur J Clin Microbiol Infect Dis 15:372–377
Gustafson R, Svenungsson B, Forsgren M, Gardulf A, Granstrom M (1992) Two-year survey of the incidence of Lyme borreliosis and tick-borne encephalitis in a high-risk population in Sweden. Eur J Clin Microbiol Infect Dis 11:894–900
Craft JE, Grodzicki RL, Steere AC (1984) Antibody response in Lyme disease: evaluation of diagnostic tests. J Infect Dis 149:789–795
Dressler F, Whalen JA, Reinhardt BN, Steere AC (1993) Western blotting in the serodiagnosis of Lyme disease. J Infect Dis 167:392–400
Guy EC, Robertson JN, Cimmino M, Gern L, Moosmann Y, Rijpkema SG et al (1998) European interlaboratory comparison of Lyme borreliosis serology. Zentralblatt Bakteriol 287:241–247
Hilton E, Devoti J, Sood S (1996) Recommendation to include OspA and OspB in the new immunoblotting criteria for serodiagnosis of Lyme disease [published erratum appears in J Clin Microbiol (1997) 35:2713]. J Clin Microbiol 34:1353–1354
Magid D, Schwartz B, Craft J, Schwartz JS (1992) Prevention of Lyme disease after tick bites. A cost-effectiveness analysis. N Engl J Med 327:534–541
Nadelman RB, Nowakowski J, Fish D, Falco RC, Freeman K, McKenna D et al (2001) Prophylaxis with single-dose doxycycline for the prevention of Lyme disease after an Ixodes scapularis tick bite. N Engl J Med 345:79–84
Aeschlimann A, Burgdorfer W, Matile H, Péter O, Wyler R (1979) New aspects of the part of the vector played by Ixodes ricinus L. in Switzerland. Preliminary note (author’s transl). Acta Trop 36:181–191
Malane MS, Grant-Kels JM, Feder HM Jr, Luger SW (1991) Diagnosis of Lyme disease based on dermatologic manifestations. Ann Intern Med 114:490–498
Hulshof MM, Vandenbroucke JP, Nohlmans LM, Spanjaard L, Bavinck JN, Dijkmans BA (1997) Long-term prognosis in patients treated for erythema chronicum migrans and acrodermatitis chronica atrophicans. Arch Dermatol 133:33–37
Mermod C, Aeschlimann A, Graf JF (1975) Ecology and ethology of Ixodes ricinus L. in Switzerland. II. Comparison of the populations 1972 and 1973. Acarology 16:612–620
Robertson JN, Gray JS, Stewart P (2000) Tick bite and Lyme borreliosis risk at a recreational site in England. Eur J Epidemiol 16:647–652
Jouda F, Perret J-L, Gern L (2004) Density of questing Ixodes ricinus nymphs and adults infected by Borrelia burgdorferi sensu lato in Switzerland: spatio-temporal pattern at a regional scale. Vector Borne Zoonotic Dis 4:23–32
Acknowledgements
We thank B. Giroud, O. Rais, R. Martinez, D. Raffalli, and M. Mottaz for excellent technical assistance; E. Godfroid for helpful advice and assistance with PCR assays; and GlaxoSmithkline for financial support. This project was supported by the Swiss National Foundation for Scientific Research, grant no. 3200-45’572.94.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nahimana, I., Gern, L., Blanc, D.S. et al. Risk of Borrelia burgdorferi infection in western Switzerland following a tick bite. Eur J Clin Microbiol Infect Dis 23, 603–608 (2004). https://doi.org/10.1007/s10096-004-1162-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-004-1162-0