
Abstract
Otitis media with effusion (OME), a form of middle ear disease, is the most common reason for young children both to visit their family doctor and to have surgery. Almost all children have at least a single episode of OME before their first birthday and annual incidence rates exceed 50% in each of the first five years. For most children, OME occurs infrequently, but about 10–15% of children have OME during more than half of their first six years. Middle ear effusions attenuate and delay sound, causing conductive sound distortion during the crucial years for language acquisition. The many studies of OME effects on language and other indices of development have produced mixed results. However, a consensus is emerging of mild language impairment in the preschool years, with subsequent performance, emotional, and behavioral difficulties. In addition to the peripheral hearing loss produced directly by the disease, binaural and other central auditory deficits can outlive the OME. It has been unclear which children are at risk of central impairment following OME, since the children studied have generally been recruited from otolaryngology clinics. Consequently, a detailed prospective history of the middle ear status of participants has not been available. By studying six-year-old children with a lifetime known history of OME, we show in this study that only those children with a cumulative OME experience of more than about half the time during the first five years consistently have residual impaired binaural hearing.
Similar content being viewed by others


INTRODUCTION
The high prevalence (Fig. 1A) and incidence (Hogan et al. 1997, 1998; Paradise et al. l997; Hogan 1999) of otitis media with effusion (OME, also known as “glue ear”) in early childhood has generated much speculation concerning its effect on the development of the human auditory system and on language acquisition and perception. Concern about the effects of OME as a form of auditory deprivation was further heightened by research from animal studies, first in the visual system (Wiesel and Hubel 1965; Sherman and Spear 1982) and later in the auditory system (Knudsen et al. 1984; Moore et al. 1989), showing that abnormal sensory experience could produce long-term changes in the structure and function of the primary brain circuits responsible for vision and hearing. More recent research provides further support for changes in auditory brain function (Moore et al. 1999; King et al. 2000; Tucci et al. 2001). However, while the effects of visual form deprivation and interocular misalignment in infancy are profound and relatively well understood, the early, mild, asymmetric conductive hearing loss produced by OME (Kokko 1974; Gravel and Wallace 2000; Hartley and Moore 2000) or, experimentally, by occlusion of the ear canal (Knudsen et al. 1984; Moore et al. 1989, 1999; King et al. 2000) or malleus removal (Cook et al. 2002) seems to exert a more subtle influence on central auditory processing.

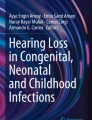
A. Prevalence of OME in the first six years. The data show the mean annual prevalence of OME [as measured by “B”-type tympanograms (Jerger 1970) in either or both ears] in the children in this study, divided into quartiles by overall (6-year) OME prevalence. Testing was conducted at approximately monthly intervals (adapted from Hogan et al. 1998). B. The binaural hearing task was presented as a computer game, with noise in each of two intervals (visually signaled as either frogs or penguins, in color in the actualgame), and the tone (randomly) in just one interval (Linux 2.0 penguin graphic courtesy of Larry Ewing). C. The masking level difference (MLD) involves presentation of target signals (S) and masking noise (N) that is either in-phase (N0S0) or out-of-phase (N0Sπ) at the two ears. When either the signal or the noise is interaurally out-of-phase, the signal is more easily detected, leading to the happy face (adapted from Moore 1997).
Another source of concern about OME came from observation of and research into language-based learning impairments. Although OME is generally a highly prevalent condition, some children with language, reading, attention, and behavior problems have been identified as having particularly high levels of OME (Zinkus et al. 1978; Silva et al. 1982). Because OME distorts sounds entering the ears and is most prevalent during the early crucial years for language acquisition (Fig. 1A; Pinker 1984; Bishop 1997), a causal link has been suggested. However, large-scale prospective studies of OME effects on language (Holm and Kunze 1969; Roberts and Wallace 1997) and other indices (Rapin 1979; Silva et al. 1986; Roberts et al. 1989; Gravel and Wallace 1998; Mody et al. 1999) of development have produced mixed results. Nevertheless, a consensus is beginning to emerge of mild language impairment in the preschool years and some performance, emotional, and behavioral difficulties in the school years (Bennett et al. 2001; Roberts et al. 2002).
OME has both acute and persistent effects on hearing. During early childhood, especially in the first three years, active OME reduces the level of sound entering the ear by up to 40 dB (Kokko 1974; Gravel and Wallace 2000) and delays the sound by up to 300 µs (Hartley and Moore 2000). OME fluctuates between unilateral and bilateral, with individual episodes lasting from a few days to many weeks (Bluestone and Klein 1995; Hogan et al. 1997, 1998; Paradise et al. 1997; Hogan 1999). After the OME clears, however, binaural and other central hearing impairments can persist. These include impaired spectrotemporal processing (Hall and Grose 1994), poor sound localization (Besing and Koehnke 1995), and difficulties in separating sounds using spatial cues (Moore et al. 1991; Pillsbury et al. 1991).
The relation between these persistent, central hearing impairments and the individual history of OME is largely unknown, since participants have generally been recruited from otolaryngology clinics. These participants have, in turn, usually been referred from family medicine practices, based on a relatively small number of clinical observations and parental selection. Moreover, the samples have been further biased by the tendency to refer, both at primary and secondary levels, on the basis of acute otitis media, a rapid onset, symptomatic form of middle ear disease. OME, by contrast and by definition, lacks the signs and symptoms of acute infection (Bluestone and Klein 1995) but is, by far, the most common form of middle ear disease in childhood. In this study, we were able to relate the lifetime history of OME to binaural hearing, since we have objectively documented the middle ear status of a group of children from birth to the time at which their binaural hearing was tested (Hogan et al. 1997, 1998).
METHODS
Participants
The children tested in this study [n = 31, age = 6.7 years (mean), 0.6 (SD)] were participants in a longitudinal study of OME (Hogan et al. 1997, 1998). Full-term, healthy infants with uneventful birth histories were examined at approximately monthly intervals during domiciliary visits for the first six years (total examinations = 1963; mean examinations per child per year = 10.4; range = 5–14), except for one child who was examined only for the first three and a half years. Each ear was examined otoscopically, to check that there was no obstruction of the canal, and tympanometrically. For the present purpose, tympanograms classified as types “A” and “C” represented an effusion-free state, while type “B” (in either ear) represented an instance of OME. The prevalence of OME was calculated as the number of instances of OME in a given year as a percentage of the total number of observations for the year. The children had a variable lifetime prevalence of the disease (Fig. 1A), from 0% to 64% in the first five years (Fig. 2A), but no effusion at the time of binaural testing. Where the children presented an effusion-free state, pure tone audiometry (British Society of Audiology 1981) was performed at least once, during domiciliary visits, between the 3rd and 6th years of the longitudinal study. Audiometry was also routinely performed during domiciliary visits in those years when type “B” tympanograms were recorded. Two of the 31 children underwent surgery for ventilation tubes. The first child had tubes at 11 months because of repeated acute ear infections, and the second child had tubes fitted in her fifth year because of chronic OME.

A,B. MLD at 6.7 years as a function of the total prevalence of OME in the first five years. OME prevalence was the percentage of flattympanograms, in either ear, relative to the total number of tests (see Fig. 1A). The data from A are replotted in B as the mean (±1 SEM) in each quartile of OME experience. Also shown are the data for adult listeners with unknown OME experience. C. Tone thresholds in the N0S0 and N0Sπ conditions for the children from the lowest three quartiles and from the highest quartile of OME experience.
Measuring binaural hearing
An index of binaural hearing is the masking level difference (MLD; Durlach and Colburn 1978; Fig. 1B). This is the extent to which the detection of an auditory signal (S 0) is enhanced in the presence of a simultaneous, in-phase masking noise (N 0) when it is presented out-of-phase (S π) at the two ears. The MLD is the laboratory model for the binaural contribution to the “cocktail party problem” (Cherry 1953), the ability to detect target sounds in noisy environments. For a 500 Hz signal tone presented in a broadband masking noise (Fig. 1C), normal-hearing adult listeners have a MLD of ~15 dB (Hogan et al. 1996; Bernstein and Trahiotis 1999).
We devised a computer game to test the MLD in children (Fig. 1B). A trial consisted of two noise bursts, in one of which a tone was randomly presented. One of two animal graphics opened its mouth in synchrony with each interval (Hartley et al. 2000). The children were trained to point to the character that “uttered” the tone. An adaptive procedure was used to measure their threshold for detection of the tone.
Digitally generated sounds (500 Hz tones, 80 ms cosine square gating envelope; 100 Hz wide, 80 ms gated, narrowband and noise centered at 500 Hz, 63 dB spectrum level; see Hartley et al. 2000) were presented as shown in Figure 1B, C and delivered by Telephonies TDH-39 earphones.
Procedure
Following brief (5 consecutive correct responses) initial training at a high tone level (90 dB SPL), tone thresholds were determined using a two-interval, forced-choice “maximum likelihood” procedure (Green 1990) that tracked 94% correct detections. Correct responses were rewarded with a brief video graphic and an increment on a linear scale. Incorrect responses produced a gesture of disappointment on the face of the nominated character (Fig. 1B). Thirtysix trials were run, including six probe trials (at 90 dB SPL) that did not contribute to the adaptive procedure. An incorrect response to a probe trial resulted in a test run being abandoned. Testing was conducted individually in a sound-attenuated room. Half the children were tested first on the N 0 S 0 condition and half on the N 0 S π condition (Fig. 1C). Otoscopy, tympanometry, and 5-frequency audiometry (British Society of Audiology 1981) were conducted between masked threshold tests. Normal-hearing adult (23–35 years) listeners (n = 8), with no known history of ear disease, were tested in an identical fashion.
RESULTS
Binaural hearing
The children had variable MLDs, from 4 to 24 dB (Fig. 2A). However, we found that children with the greatest experience of OME tended to have the lowest MLDs. By dividing the children into four equal groups (quartiles) of lifetime OME prevalence (Fig. 2B), we found children in the lowest three groups not to have significantly different mean MLDs, whereas those in the highest OME group had significantly lower MLDs than any of the other three groups (multiple one-tailed t-tests, p = 0.015, 0.022, 0.028). These data suggest a “threshold” effect for binaural impairment produced by OME. While some children with little OME had a low MLD, no children in the highest prevalence group had a MLD that exceeded the mean of any of the other groups (Fig. 2A,B). Only those children with the highest incidence of OME (>~45%) had MLDs that were consistently low. One child in the highest OME quartile and one child in the third highest OME quartile had ventilation tubes earlier in childhood (see Methods), but the tubes had extruded long before MLD testing. Identically tested adults had higher (p = 0.047) mean MLDs than the combined mean of the lower OME children, suggesting that the children's MLDs were not fully mature.
The reduced MLD during (Hall et al. 1995) and after (Moore et al. 1991; Pillsbury et al. 1991) conductive hearing loss has been shown to be due primarily to elevated thresholds in the antiphasic (S π) condition, with little change in S 0 thresholds. Here we compared S 0 and S π thresholds in children belonging to the highest quartile of OME incidence with those belonging to the other three quartiles (Fig. 2C). Consistent with these previous reports, S π thresholds in the High OME group were significantly raised relative to the collapsed data from the Low OME groups (p < 0.015). The S 0 thresholds did not differ significantly between the High and Low OME groups, suggesting that the MLD decrement in the High group was not due to a general inability to perform the task. Apparently, a major effect of prolonged OME experience is to decrease the advantage in hearing that is normally obtained when target and interfering sounds come from different directions in space and thereby generate different interaural level and phase relations.
Audiometry
Some of the audiometric results obtained during the longitudinal screening study are shown in Table 1. All the data in this table are from children who subsequently participated in the study of binaural hearing. Data are shown for 7 children in the lowest OME quartile (Low OME) who had “A”-type tympanograms at each of several visits. Their mean, air-conducted (a/c) thresholds were almost all within the normal range (≤20 dB HL). Also shown are data from 8 children belonging to the highest prevalence quartile (High OME), who had flat (“B”-type) tympanograms at each of many visits. Their a/c thresholds were highly variable and ranged from hearing within normal limits to moderate losses (55 dB HL). Their mean thresholds at the time of extant effusion were significantly (p ≪ 0.01) higher, by 10–15 dB, than those of the Low OME children.
We measured the MLD only when the children had “A”-type tympanograms. Audiometric data obtained from the children at the time of their MLD test are shown in Figure 3 and demonstrate that audiometric thresholds were unrelated to MLD. The mean thresholds at 500 Hz (or at other frequencies, not shown) did not vary markedly, or significantly, from those of the Low OME children recorded at various intervals during the longitudinal study (Table 1), and they are indicative of normal sensitivity at the time of MLD testing. In fact, the audiometric thresholds obtained at the time of MLD testing (measured in a sound chamber) were slightly lower than those obtained in the longitudinal study (measured in the children's homes). Thus, the lower MLDs recorded in the High OME children were not due to peripheral insensitivity.

Relation between audiometric threshold for each ear at 500 Hz and MLD. Audiometric thresholds were obtained in the same test session as the MLD. All children were free of OME, bilaterally, at the time of testing.
DISCUSSION
Previous studies of the effects of OME on hearing and language have mainly recruited subjects retrospectively. In a retrospective design, it is not possible to specify a relation between the disease and its consequences with any precision. Some studies (Teele et al. 1984) have used high levels of medical contact or referral to an ENT department (Moore et al. 1991; Hall et al. 1995) as the primary criterion for inclusion in an OME group. While many subjects recruited in this way will have had a high incidence of OME, it is likely that many subjects in the control group will also have had high levels of OME (Hogan et al. 1998). The sensitivity of the test is therefore compromised. Moreover, children who have hearing or language problems caused by factors other than OME are likely to be disproportionately represented in the clinical ENT population and their problems may therefore be incorrectly associated with OME.
Within our prospective study, we have been able to quantify the prevalence of OME for any given child and the levels of hearing loss associated with OME. While the hearing loss associated with OME is variable, the audiometric data collected during the longitudinal study indicate that there were significant differences in the mean hearing thresholds between the children of the lowest OME quartile and those in the highest OME quartile. This suggests that the children in these two quartiles would have different listening experiences in their early childhood. At the time of the assessment for binaural listening, there were no differences in auditory sensitivity among the four quartiles of children, and the observed differences in binaural hearing ability are therefore attributed to the child's lifetime auditory experience.
Care must also be taken in prospective designs to allow for nonlinear relations between OME and its consequences. While the effect of OME across an entire population may be weak, the results presented here show that there exists at least one measure of hearing where only a very high level of the disease leads to significant impairment. If this were also true for other outcome measures of OME, it could explain some of the discrepancies in the literature.
The mean MLD in the High OME children was about 6 dB, or 40% less than that in the lower OME children. Should we be worried about this level of binaural “impairment?” The main function of binaural unmasking is to facilitate detection of target sounds in noisy environments. However, binaural/directional enhancement is only one of at least seven cues (Cherry 1953) to this task. Therefore, we might expect that a binaural deficit is relatively unimportant. On the other hand, the acceptable level of noise in a child's environment is often determined by an adult whose judgment is based on his or her own experience. Developmental improvements in binaural hearing, shown here and elsewhere (Nozza 1987; Morrongiello et al. 1990; Moore et al. 1991), suggest that children will be relatively more disadvantaged by a given background noise level than adults. It appears that the fluctuating nature of OME may adversely affect the normal pattern of development for binaural hearing. Moreover, the presence of OME early in childhood has detrimental effects on other aspects of hearing after the disease has resolved, including comodulation masking release (Hall and Grose 1994), a measure of spectrotemporal pattern analysis (Moore 1997). These problems presumably add to those resulting from poor binaural unmasking. Finally, although we have focused in this study on the aftermath of early OME, it is important to remember that young children spend much time with impaired hearing due to active OME (Fria et al. 1985). This is, of course, especially the case for those exceeding the threshold identified here.
References
KE Bennett MP Haggard PA Silva IA Stewart (2001) ArticleTitleBehaviour and developmental effects of otitis media with effusion into the teens. Arch. Dis. Child. 85 91–95 Occurrence Handle10.1136/adc.85.2.91 Occurrence Handle1:STN:280:DC%2BD3Mvhs1yisA%3D%3D Occurrence Handle11466180
JM Besing J Koehnke (1995) ArticleTitleA test of virtual auditory localization. Ear Hear. 16 220–229 Occurrence Handle1:STN:280:ByqA3cblslE%3D Occurrence Handle7789673
LR Bernstein C Trahiotis (1999) ArticleTitleThe effects of signal duration on N 0 S 0 and N 0 S π thresholds at 500 Hz and 4 kHz. J. Acoust. Soc. Am. 105 1776–1783 Occurrence Handle10.1121/1.426715 Occurrence Handle1:STN:280:DyaK1M7ovFCksw%3D%3D Occurrence Handle10089601
CD Bluestone JO Klein (1995) Otitis Media in Infants and Children, 2nd ed. W.B. Saunders Philadelphia
DVM Bishop (1997) Uncommon understanding: Development and disorders of language comprehension in children. Psychology Press Hove, E. Sussex
InstitutionalAuthorNameBritish Society of Audiology (1981) ArticleTitleRecommended procedures for pure tone audiometry using a manually operated instrument. Br. J. Audiol. 15 213–216 Occurrence Handle1:CAS:528:DyaK2sXnsFahtb4%3D Occurrence Handle9386961
EC Cherry (1953) ArticleTitleSome experiments on the recognition of speech, with one and with two ears. J. Acoust. Soc. Am. 25 975–979
RD Cook TY Hung RL Miller DW Smith DL Tucci (2002) ArticleTitleEffects of conductive hearing loss on auditory nerve activity in gerbil. Hear. Res. 164 127–137 Occurrence Handle10.1016/S0378-5955(01)00424-5 Occurrence Handle11950532
NI Durlach HS Colburn (1978) Binaural phenomena. EC Carterette MP Friedman (Eds) Handbook of Perception, Vol 4. Academic Press New York 365–466
TJ Fria EI Cantekin JA Eichler (1985) ArticleTitleHearing acuity of children with effusion. Arch. Otolaryngo. 11 10–16
JS Gravel I Wallace (1998) ArticleTitleLanguage, speech and educational outcomes of otitis media. J. Otolaryngol. 2 17–25
JS Gravel JF Wallace (2000) ArticleTitleEffects of otitis media with effusion on hearing in the first 3 years of life. J. Speech Lang. Hear. Res. 43 631–644 Occurrence Handle1:STN:280:DC%2BD3cvptl2htQ%3D%3D Occurrence Handle10877434
DM Green (1990) ArticleTitleStimulus selection in adaptive psychophysical procedures. J. Acoust. Soc. Am. 87 2662–2674 Occurrence Handle1:STN:280:By%2BA38vksVc%3D Occurrence Handle2373801
JW Hall JH Grose (1994) ArticleTitleEffect of otitis media with effusion on comodulation masking release in children. J. Speech Hear. Res. 37 1441–1449 Occurrence Handle1:STN:280:ByqC1c3lvFQ%3D Occurrence Handle7877299
JW Hall JH Grose LL Mendoza (1995) ArticleTitleMasker interaural phase and the MLD: effects of conductive hearing loss. Hear. Res. 84 91–98 Occurrence Handle10.1016/0378-5955(95)00016-W Occurrence Handle7642459
DEH Hartley DR Moore (2000) ArticleTitleEffects of conductive hearing loss on timing of cochlear microphonic responses in the gerbil. Abstr. Assoc. Res. Otolaryngol. 23 114
DEH Hartley BA Wright SC Hogan DR Moore (2000) ArticleTitleAge-related improvements in auditory backward and simultaneous masking in 6 to 10 year old children. J. Speech Lang. Hear. Res. 43 1402–1415 Occurrence Handle1:STN:280:DC%2BD3M7ptFartA%3D%3D Occurrence Handle11193961
SC Hogan (1999) The Development of Hearing in Children: Some Effects of Otitis Media with Effusion, dissertation University of Oxford
SC Hogan SE Meyer DR Moore (1996) ArticleTitleBinaural unmasking returns to normal in teenagers who had otitis media in infancy. Audiol. Neurootol. 1 104–111 Occurrence Handle1:STN:280:DyaK1c%2Fks1ersA%3D%3D Occurrence Handle9390794
SC Hogan KJ Stratford DR Moore (1997) ArticleTitleDuration and recurrence of otitis media with effusion in children from birth to 3 years: Prospective study using monthly otoscopy and tympanometry. Br. Med. J. 314 350–353 Occurrence Handle1:STN:280:ByiC1M3nsVQ%3D
SC Hogan KJ Stratford DR Moore (1998) ArticleTitleAge and experience-related persistence of otitis media with effusion: A prospective study over five years. Abstr. Assoc. Res. Otolaryngol. 21 124
VA Holm LH Kunze (1969) ArticleTitleEffect of chronic otitis media on language and speech development. Pediatrics 43 833–839 Occurrence Handle1:STN:280:CCaC1crjs10%3D Occurrence Handle5769509
J Jerger (1970) ArticleTitleClinical experience with impedance audiometry. Arch. Otolaryngol. 92 311–324 Occurrence Handle1:STN:280:CS%2BB1c3hs1Y%3D Occurrence Handle5455571
AJ King CH Parsons DR Moore (2000) ArticleTitlePlasticity in the neural coding of auditory space in the mammalian brain. Proc. Natl. Acad. Sci. USA 97 11821–11828 Occurrence Handle10.1073/pnas.97.22.11821 Occurrence Handle1:CAS:528:DC%2BD3cXnvVSgs7k%3D Occurrence Handle11050215
EI Knudsen SD Esterly PF Knudsen (1984) ArticleTitleMonaural occlusion alters sound localization during a sensitive period in the barn owl. J. Neurosci. 4 1001–1011 Occurrence Handle1:STN:280:BiuC1cjmtVU%3D Occurrence Handle6716127
E Kokko (1974) ArticleTitleChronic secretory otitis media in children: a clinical study. Acta Otolaryngol. Suppl. (Stockh.) 327 6–44
M Mody RG Schwartz JS Gravel RJ Ruben (1999) ArticleTitleSpeech perception and verbal memory in children with and without histories of otitis media. J. Speech Lang. Hear. Res. 42 1069–1079 Occurrence Handle1:STN:280:DyaK1MvktlGhuw%3D%3D Occurrence Handle10515506
BCJ Moore (1997) An Introduction to the Psychology of Hearing, 4th ed. Academic Press San Diego
DR Moore ME Hutchings SE Meyer (1991) ArticleTitleBinaural masking level differences in children with a history of otitis media. Audiology 30 91–101 Occurrence Handle1:STN:280:By6A2crltVI%3D Occurrence Handle1877902
DR Moore ME Hutchings AJ King NE Kowalchuk (1989) ArticleTitleAuditory brain stem of the ferret: some effects of rearing with a unilateral ear plug on the cochlea, cochlear nucleus, and projections to the inferior colliculus. J. Neurosci. 9 1213–1222 Occurrence Handle1:STN:280:BiaC1MbgsFw%3D Occurrence Handle2539441
DR Moore JE Hine ZD Jiang H Matsuda CH Parsons AJ King (1999) ArticleTitleConductive hearing loss produces a reversible binaural hearing impairment. J. Neurosci. 19 8704–8711 Occurrence Handle1:CAS:528:DyaK1MXmt1ejsbs%3D Occurrence Handle10493771
BA Morrongiello K Fenwick G Chance (1990) ArticleTitleSound localisation acuity in very young infants: An observer based testing procedure. Dev. Psychol. 26 75–84 Occurrence Handle10.1037//0012-1649.26.1.75
RJ Nozza (1987) ArticleTitleThe binaural masking level difference in infants and adults: Developmental change in binaural hearing. Infant Beh. Dev. 10 105–110
JL Paradise HE Rockette DK Colborn BS Bernard CG Smith M Kurs–Lasky JE Janosky (1997) ArticleTitleOtitis media in 2,253 Pittsburgh area infants: prevalence and risk factors during the first two years of life. Pediatrics 99 318–333 Occurrence Handle1:STN:280:ByiC1MzmvFM%3D Occurrence Handle9041282
HC Pillsbury JH Grose JW Hall (1991) ArticleTitleOtitis media with effusion in children. Binaural hearing before and after corrective surgery. Arch. Otolaryngol. Head Neck Surg. 117 718–723 Occurrence Handle1:STN:280:By6A387otl0%3D Occurrence Handle1863436
S Pinker (1984) Language Learnability and Language Development. Harvard University Press Cambridge, MA
I Rapin (1979) ArticleTitleConductive hearing loss effects on children's language and scholastic skills. A review of the literature. Ann. Otol. Rhinol. Laryngol. Suppl. 60 3–12
JE Roberts MR Burchinal AM Collier CT Ramey MA Koch FW Henderson (1989) ArticleTitleOtitis media in early childhood and cognitive, academic, and classroom performances of the school-aged child. Pediatrics 83 477–485 Occurrence Handle1:STN:280:BiaC1czktFE%3D Occurrence Handle2927985
JE Roberts et al. (2002) ArticleTitleOtitis media and language learning sequelae: controversies and current research. Pediatrics Occurrence Handle11986435
J Roberts I Wallace (1997) Language and otitis media. J Roberts I Wallace F Henderson (Eds) Otitis Media in Young Children. Brookes Baltimore, MD 133–162
SM Sherman PD Spear (1982) ArticleTitleOrganization of visual pathways in normal and visually deprived cats. Physiol. Rev. 62 738–855 Occurrence Handle1:STN:280:Bi2C2svpsVI%3D Occurrence Handle6280221
PA Silva C Kirkland A Simpson IA Stewart SM Williams (1982) ArticleTitleSome developmental and behavioral problems associated with bilateral otitis media with effusion. J. Learn. Disabil. 15 417–421 Occurrence Handle1:STN:280:BiyC3M%2FlvV0%3D Occurrence Handle6891396
PA Silva D Chalmers I Stewart (1986) ArticleTitleSome audiological, psychological, educational and behavioural characteristics of children with bilateral otitis media with effusion: A longitudinal study. J. Learn. Disabil. 19 590–604
DW Teele JO Klein BA Rosner (1984) ArticleTitleOtitis media with effusion during the first three years of life and development of speech and language. Pediatrics 74 282–287 Occurrence Handle1:STN:280:BiuB2s3gslY%3D Occurrence Handle6540437
DL Tucci NB Cant D Durham (2001) ArticleTitleEffects of conductive hearing loss on gerbil central auditory system activity in silence. Hear. Res. 155 124–132 Occurrence Handle10.1016/S0378-5955(01)00256-8 Occurrence Handle1:STN:280:DC%2BD3M3ktVSgsA%3D%3D Occurrence Handle11335082
TN Wiesel DH Hubel (1965) ArticleTitleComparison of the effects of unilateral and bilateral eye closure on cortical unit responses in kittens. J. Neurophysiol. 28 1029–1040 Occurrence Handle1:STN:280:CCmC3sjlsVM%3D Occurrence Handle5883730
PW Zinkus MI Gottlieb M Shapiro (1978) ArticleTitleDevelopmental and psychoeducational sequelae of chronic otitis media. Am. J. Dis. Child. 132 1100–1104 Occurrence Handle1:STN:280:CSaD2MbkvVU%3D Occurrence Handle82400
Acknowledgements
We thank the children who participated in the study, and their parents, for their years of dedicated commitment to our research. Mervyn Hardiman designed and programmed the computer game and provided other valuable help and advice throughout the experiment. Doug Hartley helped test some of the children. We are grateful to Oliver Kacelnik, Andy King, Marina Rose, and Jan Schnupp for reading and commenting on the paper. The research was generously supported by grants from the Medical Research Council, the Oxford and Anglia Regional Health Authority, Defeating Deafness (The Hearing Research Trust), and the John Ellerman Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hogan, S.C., Moore, D.R. Impaired Binaural Hearing in Children Produced by a Threshold Level of Middle Ear Disease . JARO 4, 123–129 (2003). https://doi.org/10.1007/s10162-002-3007-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10162-002-3007-9