
Abstract
Worldwide, there are more than 10 million new cancer cases each year, and cancer is the cause of approximately 12% of all deaths. Given this, a large number of epidemiologic studies have been undertaken to identify potential risk factors for cancer, amongst which the association with trace elements has received considerable attention. Trace elements, such as selenium, zinc, arsenic, cadmium, and nickel, are found naturally in the environment, and human exposure derives from a variety of sources, including air, drinking water, and food. Trace elements are of particular interest given that the levels of exposure to them are potentially modifiable. In this review, we focus largely on the association between each of the trace elements noted above and risk of cancers of the lung, breast, colorectum, prostate, urinary bladder, and stomach. Overall, the evidence currently available appears to support an inverse association between selenium exposure and prostate cancer risk, and possibly also a reduction in risk with respect to lung cancer, although additional prospective studies are needed. There is also limited evidence for an inverse association between zinc and breast cancer, and again, prospective studies are needed to confirm this. Most studies have reported no association between selenium and risk of breast, colorectal, and stomach cancer, and between zinc and prostate cancer risk. There is compelling evidence in support of positive associations between arsenic and risk of both lung and bladder cancers, and between cadmium and lung cancer risk.
Similar content being viewed by others

Introduction
There were an estimated 10.9 million new cancer cases and 6.7 million cancer deaths worldwide in 2002 [1]. Of these, cancers of the lung, breast, colorectum, and stomach were the most common [1]. Additionally, prostate cancer was the fifth most common cancer overall and the second most common among men, and bladder cancer, ranked ninth in terms of incidence, was more common in developed countries (63% of all new bladder cancer cases) and among men (77% of new bladder cancer cases occur in men) [1]. Given the burden of disease associated with these cancers, a large number of epidemiologic studies have been undertaken to identify potential risk factors. Amongst the many factors that have been explored, the association with trace elements has received considerable attention. Trace elements are of particular interest given that levels of exposure to them are potentially modifiable.
The term ‘trace element’ refers to chemical elements present or required in minute quantities. Trace elements are found naturally in the environment and human exposure derives from a variety of sources, including air, drinking water, and food (Table 1). The World Health Organization has classified 19 trace elements as being important to human health, including arsenic (As), cadmium (Cd), nickel (Ni), selenium (Se), and zinc (Zn), amongst others (Table 1) [2].
There is a large body of literature on the role of trace elements in the development of cancer. Arsenic exposure has been examined in relation to cancer risk, generally focusing on exposure via drinking water. In addition, a number of studies of Cd, and Ni have been conducted, with a primary focus on work-place exposures. Finally, there is substantial interest in the role of Se and Zn with respect to a number of cancer sites. While Se tends to be inversely associated with cancer risk [3, 4], Zn appears to be protective when Zn deficient individuals are compared to those who are Zn sufficient [5], whereas it appears harmful when those who have Zn overload as a result of environmental exposure are compared to those who are Zn sufficient [6]. Cd, Ni, and As are generally associated with increased risk of many cancers [7] and each of them has been designated as a Group 1 human carcinogen by the International Agency for Research on Cancer (IARC) [8–10] and the US National Toxicology Program.
In this review, we focus on the association between each of the trace elements noted above and risk of cancers of the lung, breast, colorectum, prostate, urinary bladder, and stomach, the anatomical sites that have been studied most commonly. We precede our review of the epidemiologic literature with a brief discussion of the sources of exposure to trace elements, methods for measuring trace element exposure, and the biological samples in which trace elements can be measured.
Methods
Search strategy
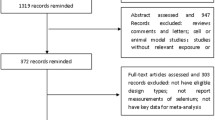
We aimed to identify all epidemiologic evidence relevant to the research question. Therefore, epidemiologic literature regarding trace element exposure and risk of cancers of the breast, lung, colorectum, prostate, bladder, and stomach, was searched for, obtained, and reviewed.
A systematic search of Medline (1966-present) was carried out for the relevant epidemiologic literature. In addition, we followed-up on references from relevant papers and prior reviews of trace elements. Appendices 1 and 2 show the search strategy employed for each of the cancers and trace elements in Medline.
Study selection
Epidemiologic studies of men and women were included in this review. Each of the articles reviewed reported on the effect of exposure to at least one of the trace elements listed in Table 1 and reported on the incidence, prevalence, and/or death from lung, bladder, breast, colorectal, prostate, or stomach cancer. Epidemiologic studies not published in English were excluded from this review, as were published abstracts and non-peer-reviewed literature.
Data extraction and analysis
All relevant epidemiologic studies were read in full and the data were extracted. Details on study design, study population, exposure source and exposure measures, outcome, results, and conclusions were recorded. Included studies were summarized in Tables 3–8 and described briefly in the text. We considered issues related to exposure measurement, along with considerations of study design, sample size, and magnitude of effect, in drawing conclusions from the literature.
Sources of trace element exposure
Trace elements are found naturally in the environment and human exposure derives from a variety of sources, including air, drinking water, and food.
Concentrations of trace elements in the air are generally low. Levels of As in the air range from approximately 1 to 2,000 ng/m3 [11, 12], levels of Cd generally range from 1 to 40 ng/m3 [13] but can reach up to 100 ng/m3 near emission sources [14], and levels of Ni in cities and rural areas range from 7 to 12 ng/m3 [15] (Table 1). Welders, workers in the smelting and refining industries, and those employed in the production of batteries, coatings, and plastics, can be exposed to much higher levels of airborne Cd and Ni [14, 15].
Each of the trace elements under consideration here is found in drinking water supplies. The average amount of Cd in drinking water is approximately 1 part per billion (ppb) and intakes from drinking water range from 0.01 μg/day in more remote geographic locations to 25 μg/day in heavily polluted areas [14]. The average concentration of Ni in water ranges from 3 to 7 ppb [14, 15]. With respect to As, which is found naturally in ground water, the Agency for Toxic Substances and Disease Registry (ATSDR) in the United States estimates that 80% of the US water supply has less than 2 ppb, but about 2% has greater than 20 ppb [11]. Internationally, levels of As in water range from as low as <1 ng/m3 in remote locations (e.g., the Canadian arctic) to as high as 2,000–3,600 μg/l in Bangladesh and India [14, 16].
Diet is the primary source of Zn and a major source of Se exposure. Average Zn consumption from food ranges from 5.2 to 16.2 mg/day [14, 17] and Zn levels in animal products vary depending on the soil and water concentrations where the animals were raised [17]. Average Se consumption from food ranges from 71 to 152 μg/day [18]. Fish and seafood are the main sources of dietary As exposure [11]. However, the As in these foods is mainly in the form of organic As, which is considered less harmful than inorganic As [11]. With respect to Cd, the average individual consumes 30 μg/day, but only 1–3 μg/day is absorbed into the body [13, 14]. Likewise, while average Ni consumption from foods is 170 μg/day in the United States [15] and between 200 and 300 μg/day internationally [14], less than 2% is absorbed [15].
Methods for measuring trace element exposure
Exposure to many trace elements (e.g., As, Cd, and Ni) is largely from occupational sources. Studies of exposure to such trace elements have utilized various exposure assessment methods including job histories (yielding subjective assessments of exposure as high, medium, or low), measurement of airborne and static dust, and personal monitoring devices. Often, these measures are combined with job history information, such as the number of years employed in a particular area, to develop an estimate of cumulative exposure. Between-study differences in the method of exposure assessment make it difficult to compare results across studies. Further, assessments based on type of employment (e.g., production versus maintenance) assume that emissions are confined to specific locations, which may not always be the case. In addition, many of the occupational studies have (of necessity) relied on historical data, which are limited due to possible changes in production techniques and ventilation systems over time.
Several other methods for measuring trace element exposure have been tested and utilized, including assessment of dietary intake and analytical assessment of trace element levels in biological and environmental samples. Methods to assess intake of trace elements from dietary sources (and via supplement use) include 24-h and 7-day dietary recalls, diet histories, and food frequency questionnaires (FFQ) [19]. To date, these methods have been used mostly to estimate dietary intake of Zn and Se. Diet measurement methods are limited due to the possibility of recall bias (particularly in case–control studies), by the possibility of misclassification of exposure due to the inherent inaccuracy of such methods (for example, Se intake is measured inaccurately by food frequency questionnaires [20]), due to potential differences in absorption of trace elements depending upon food preparation methods, and due to variation by geographic locale in the levels of trace elements in the soil in which foods are grown [21]. However, this is less of an issue in developed countries where most people do not eat locally grown produce.
The various analytical methods for measuring the content of trace elements in biological and environmental samples are listed in Table 2. It should be noted that the ability of each of these methods to detect trace elements in biological specimens is dependent, in large part, on the specimen (e.g., blood, urine, hair, or nail), the methods used to prepare the specimen for analysis, and the trace element of interest [22]. A comprehensive discussion of the methods utilized for each trace element is beyond the scope of the present review—more information (described under the ToxFaq for each trace element) can be found at the United States Department of Health and Human Services ATSDR website http://www.atsdr.cdc.gov/toxfaq.html.
Use of biological specimens for measuring trace element exposure
Estimates of trace element exposure are often determined by sampling biological specimens such as blood (including whole blood, serum, plasma, and erythrocytes), urine, hair, and nails, each of which differs in terms of the exposure period represented. In relation to the etiology of cancer, cumulative exposure is usually of interest. Plasma and serum measures tend to reflect short-term exposures, while trace element levels in erythrocytes represent long-term exposure [23]. Toenails are often preferable to other biological samples (e.g., blood, urine) for the measurement of trace element levels because they reflect longer-term exposure. A number of studies have assessed the validity/reproducibility of toenails as a surrogate measure of selenium intake [20, 24–26] and have shown good or strong correlations between toenail measures and intake. Although analytical methods for determining arsenic levels in nails were outlined by Agahian et al. in 1990 [27], few epidemiologic studies have employed this method. Garland et al. [24], using data from a 6-year reproducibility study, suggests that toenail measures of zinc may be a good indicator of long-term zinc exposure. In contrast, serum and plasma biomarkers of Zn are considered to be poor indicators of whole body Zn status [28, 29] given that plasma levels of zinc are homeostatically regulated and that other common factors that can influence its distribution [29]. A detailed discussion of the validity/reproducibility of biological specimens used for measuring trace element exposure is beyond the scope of the present review—more information can be found in the World Health Organization’s (WHO) Trace Elements in Human Nutrition and Health [2] and at the United States Department of Health and Human Services ATSDR website (described under the ToxFaq for each trace element) http://www.atsdr.cdc.gov/toxfaq.html.
Results: trace elements and cancer risk—epidemiologic evidence
Arsenic
Although there is some evidence of clinical manifestations resulting from As deficiencies in certain animal species [2, 30, 31], currently there is no known beneficial biological function of As in humans. In contrast, As has been shown to induce carcinogenesis via a wide range of cellular changes including alterations in cell differentiation and proliferation [7, 32]. In addition, inorganic As has been found to induce chromosomal aberrations and sister chromatid exchange [7]. Cells exposed to As have also been shown to increase cellular tyrosine phosphorylation, which is related to the aberrant cell signaling and uncontrolled cell growth associated with cancer development [33, 34]. A review of the As in drinking water was recently compiled by the State of California [35] and provides information on the association between As and other health conditions, including cancer outcomes not included in this review.
A number of ecologic studies from Taiwan, a location known for its high levels of As in drinking water (average intake > 1 mg/day [36]), have suggested that As may be associated with increased risks of bladder and lung cancer. Given this, studies of lung and bladder cancer risk have been conducted in other areas with known geologic As contamination of drinking water. A summary of the literature regarding high levels of As exposure (≥100 μg/l) and cancer risk is presented in Table 3. Two case–control [37, 38] and two [39, 40] out of three [39–41] cohort studies have found elevated lung cancer risks associated with high levels of exposure to As from drinking water, whereas one cohort study showed an inverse association [41]. In addition, case–control [37, 42] and four [39, 40, 43, 44] out of five [39–41, 43, 44] cohort studies conducted in areas with high As concentrations in drinking water have shown positive associations between As in drinking water and bladder cancer risk. Furthermore, there is some evidence that exposure to high levels of As in drinking water is associated with an increased risk of prostate cancer [41].
While the association between As and cancer, particularly lung and bladder cancers, is established at high levels of exposure, the association at lower levels (< 100 μg/l) is less certain. A summary of the literature regarding lower levels of As exposure (both occupational and from drinking water) and cancer risk is presented in Table 4. In the only study of As and breast cancer risk reported to date, Garland et al. [45] observed no association between levels measured in toenails and risk. With respect to lung cancer, one case–control [46] and two cohort studies [47, 48] have observed positive associations between occupational As exposure and lung cancer risk, while one case–control study by Coggon et al. [49] found no association between occupational As exposure and risk of lung cancer. However, exposure in the latter study was estimated by creating a job matrix where occupational units were classified according to their likely exposure to As rather than direct measurement of airborne levels, and therefore the levels of exposure cannot be directly compared to those in the other studies included in this review [49]. Both Bates et al. [50] and Steinmaus et al. [51], in analyses of As in drinking water, and Michaud et al. [52], in an analysis of toenail As, found no association between As exposure and bladder cancer risk.
Cadmium
Although there is some evidence that low concentrations of dietary Cd may be beneficial to some animal species [2], currently there is no evidence of a beneficial function in humans. Indeed, on the basis of evidence from experimental and epidemiologic studies, IARC [8] and the US National Toxicology Program [53] have designated Cd as a known human carcinogen. It is thought that Cd acts via genotoxic mechanisms including induction of single-strand DNA breaks [54], and also that it inhibits DNA repair by inactivation of the mismatch repair system [54, 55], activates proto-oncogenes [56, 57] and inhibits apoptosis [58].
Table 5 presents a summary of the literature regarding Cd exposure and cancer risk. To date, most studies of Cd and cancer have focused on lung and prostate cancer. Six of the seven occupational cohort studies that have been reported have found statistically significant increased risks of lung cancer associated with relatively high Cd exposure [59–65].
The relationship between Cd exposure and prostate cancer risk has been examined in one case–control [66], two nested case–control [67, 68], and two cohort analyses [60, 63]. In the only case–control study to date (358 incident cases), West et al. [66] reported a statistically significant positive association with ingested Cd from dietary sources, as assessed by a food frequency questionnaire. The remaining studies differed in that they examined the association between occupational Cd exposure and prostate cancer risk. Armstrong and Kazantzis [68] and Platz et al. [67] each analyzed data from two separate US cohort studies using nested case–control designs (39 and 115 incident cases, respectively) and reported no association between high Cd exposure and prostate cancer risk. Kazantzis et al. [63] likewise found no association between occupational exposure to Cd and prostate cancer mortality in a British cohort, but the study included only 30 cases. In contrast, Sorahan and Watherhouse [60] observed a statistically significant increased risk of prostate cancer mortality among Ni–Cd alloy workers in the United Kingdom, although this finding was based on only five prostate cancer cases.
Nickel
In 1996, the World Health Organization classified Ni as a trace element that is ‘probably’ essential [2], given its role in Ni-containing enzymes found in plants and microorganisms. However, evidence that Ni has similar functions in humans is not currently available. In contrast, Ni compounds can display tumor promoting capability via a number of mechanisms including inhibition of intercellular communication [69], immortalization of fibroblasts and epithelial cells [70–73], the induction of DNA deletions and aberrations [74], production of DNA-protein cross-links, oxidative damage, inhibition of nucleotide excision repair [74–76] and an increase in DNA methylation leading to inactivation of gene expression [77]. In epidemiologic studies of the association between Ni and cancer risk, Ni has been examined either alone or in combination with Cd (in the form of Ni–Cd) (Table 6).
Grimsrud et al. [78], in a nested case–control study of Norwegian Ni-refinery workers, reported no association between lung cancer incidence and occupational sulfidic, oxidic, or metallic Ni exposure. However, in a subsequent study based on the same cohort, Grimsrud et al. [79] analyzed data for workers employed between 1910 and 1989 and who were alive after 1953, and they reported an increased risk of lung cancer associated with both total and water-soluble Ni after controlling for smoking history. Of the six cohort studies of job-related Ni exposure, four observed no association with lung cancer risk [61, 62, 80, 81], and two observed an increased risk [82, 83] (Table 6).
Studies of colorectal, bladder, and gastric cancers [80, 81] and Ni exposure have also been conducted and have reported no association (Table 6). In contrast, Sorahan and Watherhouse [60] reported a statistically significant increased risk of prostate cancer mortality with relatively high occupational Ni exposure. As with results for other cancer sites, the conclusions that can be drawn from these studies are limited by the relatively small number of cases included (Table 6).
Selenium
Selenium is considered an essential trace element because it is the primary component of selenoproteins, which have roles in counteracting oxidative stress and regulating the redox status of other molecules [84]. Not surprisingly, therefore, Se has been studied extensively in relation to cancer risk due to its possible preventive effects. While there is epidemiologic evidence to support an inverse association between Se and risk of some cancers, the evidence is not consistent. A summary of the current literature regarding Se exposure and risk of breast, colorectal, lung, stomach, bladder, and prostate cancer is presented in Table 7.
The results of case–control and prospective cohort studies conducted to date do not support an association between Se and breast cancer [23, 85–94]. Of the seven case–control studies [23, 85–87, 91, 93, 94], only Schrauzer et al. [93] found a statistically significant inverse association between Se exposure and breast cancer risk. In contrast, larger case–control studies such as those by Van’t Veer et al. [85, 86] and Ghadirian et al. [87], both of which examined toenail Se, which is considered more representative of long-term Se exposure [95, 96], found no association with breast cancer risk. In addition, none of the four cohort studies that have examined this relationship [88–90, 92], of which three utilized toenail measures of Se exposure [88–90], have found any association between Se and breast cancer risk. The conclusion that Se is not associated with breast cancer risk is supported by the fact that studies to date have measured exposure using different approaches (including analysis of toenail, whole blood, plasma, and erythrocyte samples, and measurement of dietary Se), and produced mostly null results. In this regard, van’t Veer et al. [85] examined the association between Se and breast cancer risk by measuring both dietary Se intake using a FFQ and Se concentrations in plasma, erythrocytes, and toenails. The magnitude of the odds ratios comparing extreme quartile levels ranged from 0.9 (erythrocyte Se) to 2.0 (plasma Se), and none of these associations was statistically significant [85].
In a cross-sectional study of 48 individuals in the United States, Clark et al. [97] observed an almost 4-fold increased risk of colorectal cancer for plasma Se concentrations ≥ 128 μg/l versus those < 128 μg/l (95% CI = 1.02–15.71). However, subsequent case–control and cohort studies of Se and colorectal cancer risk, using either serum [98–100] or toenails [87, 101–103] for Se measurement, have largely reported no association [87, 99–103]. Fernandes-Banares et al. [98] used fasting blood samples and showed an inverse association between serum Se levels and risk, while Nomura et al. [99] used non-fasting samples and showed no association with serum Se levels. However, given that Se levels measured in blood samples represent recent exposure, comparison of the results of studies using fasting blood samples to those using non-fasting blood samples may not be appropriate. Furthermore, long-term measures of Se intake are more useful. In this regard, Ghadirian et al. [87], Mannisto et al. [102], van den Brandt et al. [103], and Garland et al. [101] measured Se concentrations in toenail samples, each using similar methodologies. However, the results were mixed, with Ghadirian et al. [87] reporting a statistically significant inverse association, Mannisto et al. [102] and van den Brandt et al. [103] observing no association, and Garland et al. [101] reporting a statistically non-significant increased risk of colorectal cancer.
Results from nested case–control studies of Se and lung cancer risk have been mixed. Kabuto et al. [104] conducted a nested case–control study in Japan and reported that cases were more likely to have higher serum Se concentrations than controls, while Nomura et al. [99] and Ratnasinghe et al. [105], in nested case–control analyses of data from Hawaii and China, respectively, reported no association with serum levels. More recently, a randomized trial was conducted in the United States to test the effect of Se supplementation (200 μg/day) on non-melanoma skin cancer recurrence, with lung cancer incidence as a secondary endpoint [106]. Although analysis of data from the first 10 years of the study (1983–1993) revealed a 44% decrease in lung cancer risk (95% CI = 0.31–0.76) in association with the intervention [106], a re-analysis conducted after three years of additional follow-up revealed attenuation of the hazard ratio to 0.74, which was no longer statistically significant (95% CI = 0.44–1.24). A limitation of this study is that it included only 60 incident lung cancer cases [106]. In addition to these studies, which assessed Se exposure using serum samples, toenail Se levels have been investigated in relation to lung cancer risk in a number of studies. Hartman et al. [107], in a nested case–control analysis of data from the Alpha-Tocopherol Beta-Carotene (ATBC) Cancer Prevention Cohort based on 250 cases, found a statistically significant inverse association between toenail Se and risk. Likewise, van den Brandt et al. [108] reported a 50% decreased risk of lung cancer associated with toenail Se concentrations (p trend = 0.0006). In contrast, Garland et al. [101], in an analysis of data from the Nurses’ Health Study (47 incident cases), reported an approximately 4-fold increased risk of lung cancer, although this finding was not statistically significant.
The results of studies of the association between Se and gastric cancer risk have varied somewhat, although most have yielded point estimates at or below unity. Ecologic studies conducted in Japan [109] and China [110] showed statistically significant inverse correlations between Se in drinking water and plasma Se, respectively, and gastric cancer mortality. Chen et al. [111] in a cross-sectional study and Kabuto et al. [104], in a case–control study, however, observed no association between serum Se and stomach cancer risk. Likewise, both Zhang et al. [112] and Nomura et al. [99] observed no association between serum Se and stomach cancer risk in nested case–control studies in the United States. In contrast, three of four case-cohort studies have reported statistically significant inverse associations [103, 113–115]. Two randomized trials of dietary supplementation have been conducted in Linxian, China [116, 117], a region known for both its high incidence of gastric cancer and a number of nutritional deficiencies [114]. The larger General Population Trial, which included 29,584 adults (16 incident cases) found no association with the vitamin E/β-carotene/Se combination [117]. Dawsey et al. [116] analyzed data from the Dysplasia Trial in Linxian, China, and at the 1987 follow-up they found an increased risk of gastric cancer in association with a multivitamin, multimineral supplement containing Se, but an inverse association in 1991; neither of these findings was statistically significant. However, given that these trials examined the effect of Se in concert with other vitamins/minerals, conclusions about the effect of Se supplementation alone cannot be drawn from them.
With respect to bladder cancer, Nomura et al. [99] and Helzlsouer et al. [118] each examined the association between serum Se and risk and reported elevated odds ratios (1.9 and 2.06, respectively) for the lowest versus the highest tertile of serum Se. While neither of these associations was statistically significant, Helzlsouer et al. [118] did report a statistically significant trend (p trend = 0.03) of increasing risk with decreasing serum Se levels. Similarly, Zeegers et al. [119] reported an inverse association between toenail Se concentration and bladder cancer risk in a case-cohort analysis from the Netherlands Cohort Study. Michaud et al. [120], however, found no association between toenail Se and bladder cancer in a nested case–control analysis of male smokers enrolled in the Alpha-Tocopherol/Beta-Carotene (ATBC) trial. Currently there is insufficient evidence to draw a conclusion regarding the association between Se exposure and bladder cancer risk.
Recently, much attention has been given to the potentially protective effect of Se in relation to prostate cancer. In this regard, although a number of case–control studies, nested [92, 94, 113], and non-nested [87, 121, 122], have suggested that there is no association between Se and prostate cancer risk, several other nested case–control analyses of data from different study populations within the United States [123–127] and a case-cohort analysis of data from the Netherlands [128] have reported statistically significant inverse associations between Se concentrations (based on measurements in plasma [123, 127], serum [125] and/or toenails [124, 126, 128]) and prostate cancer risk. Hartman et al. [129] analyzed data from the ATBC trial as a cohort study and reported that dietary Se (both including and excluding supplements) was not associated with prostate cancer risk, although there was some evidence for an inverse association with Se among those receiving α-tocopherol supplements. Randomized trials have also been undertaken to further study the potential association between Se and prostate cancer risk. In one such study, Clark et al. [130] examined data from a trial conducted in the United States and reported a 63% decreased risk of prostate cancer for those receiving 200 μg of Se per day versus placebo after 4.5 years of treatment and 6.5 years of follow up (p trend = 0.002). The Selenium and Vitamin E Cancer Prevention Trial (SELECT), a clinical trial with more than 35,000 participants, which will take approximately 12 years to complete, was initiated in order to further investigate this association (http://cancer.gov/select).
Zinc
The effects of Zn deficiency in humans were first reported in the 1960s [131, 132] and include growth retardation, cognitive impairment and immune dysfunction [133]. Zinc is also involved with metallothionine synthesis, which is thought to inhibit free radical production [134]. Furthermore, it has been shown that zinc chloride significantly decreases DNA strand breaks in human cutaneous fibroblasts exposed to UVA1 radiation [135]. Hence, it is conceivable that there might be an inverse association between Zn and cancer risk.
The association between Zn levels and cancer risk has been examined for several anatomic sites (Table 8]. Case–control studies by Gupta et al. [136] (35 cases), and more recently by Adzersen et al. [137] (310 cases), both yielded statistically significant inverse associations between Zn exposure, measured in serum and diet, respectively, and breast cancer risk. Garland et al. [45], however, in a nested case–control study, including 433 incident cases, reported no association between toenail Zn and breast cancer risk. Whole blood, and its components, can be tested to measure exposure to a number of trace elements. Plasma and serum measures tend to reflect short-term exposures, while trace element levels in erythrocytes represent long-term exposure [23]. As noted earlier, there is evidence that status biomarkers such as blood and plasma tend to be poor indicators of whole body Zn status [28]. Toenails are often preferable to other biological samples (e.g., blood, urine) for the measurement of trace element levels because they tend to reflect longer-term exposure. The use of different status biomarkers in these studies may be an important contributor to the mixed outcome results of competing studies.
The literature regarding the association between Zn exposure and lung cancer differs according to the level of Zn exposure. That is, when compared to those who are Zn sufficient, the effect of Zn deficiency is different from that of Zn overexposure (e.g, through occupational exposure). A case–control study by Sattar et al. [5], which compared individuals who were Zn deficient as a result of inadequate dietary intake to those who were Zn sufficient, suggested that there is an inverse association between plasma Zn levels and lung cancer risk, while in other studies of Zn deficiency, both Harris et al. [138] and Kabuto et al. [104] found no association with lung cancer risk. The results of studies of occupational Zn exposure are mixed. A case–control study by Blot et al. [6], which compared individuals who are Zn sufficient to those who have Zn overload, found a positive association between occupational Zn exposure and risk. In contrast, Cocco et al. [139], in a prospective study of 4,740 lead and Zn smelter workers in Italy, found no association between lung cancer mortality and airborne Zn concentrations as assessed using regular measurements of airborne dust from personal and static sampling devices.
Zinc has also been examined in association with risk of gastric cancer. In a case–control study, Zhang et al. [140] utilized a FFQ to determine dietary Zn intake and reported an inverse trend of borderline statistical significance with increasing consumption (p trend = 0.07). In contrast, Kabuto et al. [104] compared serum Zn concentrations in cases of gastric cancer (77 incident cases) and controls in Japan and observed essentially no difference. Zhang et al. [112] likewise observed no difference in the Zn:Cu ratio between cases and controls in a nested case–control study in the United States (88 incident cases). Analyses of data from two randomized trials conducted in China have found no association between a combination of supplements, including Zn (22.5 mg and 45 mg, respectively), and gastric cancer risk [116, 117].
A number of studies have also been undertaken to examine the association of Zn with prostate cancer. Studies comparing Zn levels in malignant to normal prostate tissue have found that Zn is 60–70% lower in malignant prostate tissue [141]. However, thus far, results from case–control and cohort studies have been mixed. Kolonel et al. [142] studied the association between dietary Zn intake and risk, stratified by age, and reported a statistically significant positive association between total Zn (including Zn from foods and supplements) and prostate cancer risk among Hawaiian men 70 years of age and older, but found no association between either total dietary Zn or non-supplemental Zn and risk among men under 70 years of age, while Leitzmann et al. [143] found a 2.9-fold increased risk of advanced prostate cancer with supplemental Zn use in a prospective cohort study conducted in the United States.. In contrast, Kristal et al. [144] found a borderline inverse association between frequency of Zn supplement use and prostate cancer risk in a case–control study in the United States, and recently, Platz et al. [67] conducted a nested case–control study of prediagnostic toenail Zn and found a statistically non-significant 37% decreased risk of prostate cancer in association with toenail Zn levels. In case–control studies in Utah and Yugoslavia, respectively, neither West et al. [66] nor Vlajinac et al. [145] found an association between dietary Zn and case status.
Discussion
Conclusions
There is now a substantial body of epidemiologic literature on the association between trace element exposure and cancer risk and a summary of the current state of the evidence for the cancer sites of interest here is presented in Table 9. In drawing our conclusions, we considered issues related to exposure measurement, study design, and sample size. Results from cohort studies and randomized trials (when available) were given greater consideration than were results from case–control and cross-sectional studies on the same topic. In addition, studies which utilized objective exposure measures (e.g., biological measures) were given more weight than were those that used subjective measures (e.g., qualitative assessments of high/medium/low exposures).
In brief, the evidence currently available appears to support an inverse association between Se exposure and prostate cancer risk. In contrast, the vast majority of the studies of Se and breast cancer, which have included large case–control and cohort studies utilizing different means of quantifying exposure, do not appear to support an association. Similarly, there do not appear to be associations between Se and risk of colorectal or stomach cancer. With respect to Zn, although there is literature from case–control studies to support an inverse association between Zn and breast cancer risk, the one cohort study to date does not support an association and additional prospective studies are needed. To date, there is essentially no evidence for associations between dietary Zn intake and risk of stomach or prostate cancer, or between occupational Zn exposure and lung cancer risk. There is compelling evidence to support positive associations between As and risk of lung cancer at both high and low exposure levels and between As and bladder cancer risk at high exposure levels [35]. There is also strong evidence of a positive association between occupational Cd exposure and lung cancer risk.
Future directions
Although the association between trace element exposure and cancer risk has been examined in a number of large prospective studies, there is a need for a larger studies to be conducted to enable the possibility of effect modification to be examined. For example, it would be of interest to examine the association between Zn and other trace elements and lung cancer risk across strata of smoking history due to the antioxidant role of Zn.
While randomized trials of Se have been conducted with respect to stomach cancer and have been initiated to assess its effect on risk of prostate cancer, randomized trials investigating other trace elements that may also reduce cancer risk (e.g., Zn) have not been conducted as yet. Such trials might focus initially on the effect of the interventions on intermediate end-points such as cancer precursors.
Finally, while there is now a considerable amount of epidemiologic evidence concerning the role of trace elements in influencing cancer risk, additional studies are needed to elucidate further the mechanisms underlying trace element carcinogenesis.
Abbreviations
- ATBC:
-
Alpha-Tocopherol Beta-Carotene Cancer Prevention Cohort
- As:
-
arsenic
- AAS:
-
atomic absorption spectrophotometry
- AES:
-
atomic emission spectrophotometry
- AR:
-
attributable risk
- Cd:
-
cadmium
- EMR:
-
excessive mortality rate
- FAA:
-
flame atomic absorption
- GC:
-
gastric cardia adenocarcinoma
- ICP-MS:
-
inductively coupled plasma mass spectometry
- IARC:
-
International Agency for Research on Cancer
- NAA:
-
neutron activation analysis
- Ni:
-
nickel
- OG:
-
non-cardia gastric adenocarcinoma
- ppb:
-
part per billion
- Se:
-
selenium
- SIR:
-
standardized incidence ratio
- SMR:
-
standardized mortality ratio
- SELECT:
-
The Selenium and Vitamin E Cancer Prevention Trial
- ATSDR:
-
United States Department of Health and Human Services Agency for Toxic Substances & Disease Registry
- Zn:
-
zinc
References
Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global cancer statistics, 2002. CA Cancer J Clin 55: 74–108
World Health Organization (1996) Trace elements in human nutrition and health. World Health Organization, Geneva
Whanger PD (2004) Selenium and its relationship to cancer: an update dagger. Br J Nutr 91:11–28
Prasad AS, Kucuk O (2002) Zinc in cancer prevention. Cancer Metastasis Rev 21:291–295
Sattar N, Scott HR, McMillan DC, Talwar D, O’Reilly DSJ, Fell GS (1997) Acute-phase reactants and plasma trace element concentrations in non-small cell lung cancer patients and controls. Nutr Cancer 28:308–312
Blot WJ, Brown LM, Pottern LM, Stone BJ, Fraumeni Jr JF (1983) Lung cancer among long-term steel workers. Am J Epidemiol 117:706–716
Hayes RB (1997) The carcinogenicity of metals in humans. Cancer Causes Control 8:371–385
International Agency for Research on Cancer (IARC) (1993) IARC monographs on the evaluation of the carcinogenic risk to man: beryllium, cadmium, mercury, and exposures in the glass manufacturing industry. Working Group views and expert opinions. IARC Press, Lyon
International Agency for Research on Cancer (IARC) (1999) Arsenic and arsenic compounds. Overall evaluations of carcinogenicity: an updating of IARC Monographs Volumes 1 to 42. IARC, Lyon (France). Report No.: Supplement 7
International Agency for Research on Cancer (IARC) (1990) Chromium, nickel and welding. IARC Monogr Eval Carcinog Risk Chem Man 49:1–648
Agency for Toxic Substances and Disease Registry (ATSDR) (2003) Toxicological profile for arsenic. United States Department of Health and Human Services Agency for Toxic Substances and Disease Registry, Atlanta, GA, Report No.: 7440-38-2
Rasmussen L, Andersen KJ (2003) Environmental health and human exposure assessment. In: World Health Organization, UNICEF, editors. Arsenic in drinking water. IWA, London, pp 67–168
Agency for Toxic Substances and Disease Registry (ATSDR) (1999) Toxicological profile for cadmium. United States Department of Health and Human Services Agency for Toxic Substances and Disease Registry, Atlanta, GA, Report No.: 7440-43-9
WHO Regional Office for Europe (2000) Air quality guidelines, 2nd edn. World Health Organization, Copenhagen, Denmark
Agency for Toxic Substances and Disease Registry (ATSDR) (2003) Toxicological profile for nickel. United States Department of Health and Human Services Agency for Toxic Substances and Disease Registry, Atlanta, GA, Report No.: 7440-02-0
Lamm SH, Engel A, Kruse MB, et al (2004) Arsenic in drinking water and bladder cancer mortality in the United States: an analysis based on 133 U.S. counties and 30 years of observation. J Occup Environ Med 46:298–306
Agency for Toxic Substances, Disease Registry (ATSDR) (2003) Toxicological profile for zinc. United States Department of Health and Human Services Agency for Toxic Substances and Disease Registry, Atlanta, GA, Report No.: 7440-66-6
Agency for Toxic Substances and Disease Registry (ATSDR) (2003) Toxicological profile for selenium. United States Department of Health and Human Services Agency for Toxic Substances and Disease Registry, Atlanta, GA, Report No.: 7782-49-2
Abdulla M, Parr RM, Iyengar GV (1993) Trace element requirements, intake and recommendations. In: Prasad AS (eds) Essential and toxic trace elements in human health and disease: an update. Wiley-Liss, New York, pp 311–328
D Hunter JS Morris CG Chute et al. (1990) ArticleTitlePredictors of selenium concentration in human toenails Am J Epidemiol 132 IssueID1 114–122 Occurrence Handle2356804 Occurrence Handle1:STN:280:DyaK3c3ovFOhtA%3D%3D
Burguera JL, Burguera M, Gallignani M, Alarcon OM, Burguera JA (1990) Blood serum selenium in the province of Merida, Venezuela, related to sex, cancer incidence, and soil selenium contnet. J Trace Elem Electrolytes Health Dis 4:73–77
Agency for Toxic Substances and Disease Registry (ATSDR) (2001) ToxFAQs. U.S. Department of Health and Human Services, Public Health Service, Atlanta, GA
Meyer F, Verreault R (1987) Erythrocyte selemium and breast cancer risk. Am J Epidemiol 125:917–919
Garland M, Morris JS, Rosner B, et al (1993) Toenail trace element levels as biomarkers: reproducibility over a 6-year period. Cancer Epidemiol Biomarkers Prev 2:493–497
Swanson CA, Longnecker MP, Veillon C, et al (1990) Selenium intake, age, gender, and smoking in relation to indices of selenium status of adults residing in seleniferous area. Am J Clin Nutr 52:858–862
Longnecker MP, Stram DO, Taylor PA, et al (1996) Use of selenium concentration in whole blood, serum, toenails, or urine as a surrogate measure of selenium intake. Epidemiol 7:384–390
Agahian B, Lee JS, Nelson JH, John RE (1990) Arsenic levels in fingernails as a biological indicator of exposure to arsenic. Am Ind Hyg Assoc J 51:646–651
King JC (1990) Assessment of zinc status. J Nutr 120:1474–1479
Wood RJ (2000) Assessment of marginal zinc status in humans. J Nutr 130:1350S–1354S
Nielsen FH (1993) Ultratrace elements of possible importance for human health: an update. In: Prasad AS (eds) Essential and toxic trace elements in human health and disease: an update. Wiley-Liss, New York, pp 355–376
Uthus EO, Seaborn CD (1996) Deliberations and evaluations of the approaches, endpoints and paradigms for dietary recommendations of the other trace elements. J Nutr 126:2452S–2459S
Leonard A, Gerber GB (1994) Mutagenicity, carcinogenicity and teratogenicity of vanadium compounds. Mutat Res 317:81–88
Hossain K, Akhand AA, Kato M, et al (2000) Arsenite induces apoptosis of murine T lymphocytes through membrane raft-linked signaling for activation of c-Jun amino-terminal kinase. J Immunol 165:4290–4297
Chen W, Martindale JL, Holbrook NJ, Liu Y (1998) Tumor promoter arsenite activates extracellular signal-regulated kinase through a signaling pathway mediated by epidermal growth factor receptor and Shc. Mol Cell Biol 18:5178–5188
Office of Environmental Health Hazard Assessment (2004) Public health goal for arsenic in drinking water. California Environmental Protection Agency
Bates MN, Smith AH, Hopenhayn-Rich C (1992) Arsenic ingestion and internal cancers: a review. Am J Epidemiol 135:462–476
Chen CJ, Chuang YC, You SL, Lin HY (1986) A retrospective study on malignant neoplasms of bladder, lung and liver in blackfoot disease endemic area in Taiwan. Br J Cancer 53:399–405
Ferreccio C, Gonzalez PC, Milosavjlevic SV, Marshall GG, Sancha AM, Smith AH (2000) Lung cancer and arsenic concentrations in drinking water in Chile. Epidemiology 11:673–679
Chiou HY, Hsueh YM, Liaw KF, et al (1995) Incidence of internal cancers and ingested inorganic arsenic: a seven-year follow-up study in Taiwan. Cancer Res 55:1296–1300
Chen Y, Ahsan H (2004) Cancer burden from arsenic in drinking water in Bangladesh. Am J Public Health 94:741–744
Lewis DR, Southwick JW, Ouellet-Hellstrom R, Rench J, Calderon RJ (1999) Drinking water arsenic in Utah: A cohort mortality study. Environ Health Perspect 107:359–365
Bates MN, Rey OA, Biggs ML, et al (2004) Case–control study of bladder cancer and exposure to arsenic in Argentina. Am J Epidemiology 159:381–389
Chiou HY, Chiou ST, Hsu YH, et al (2001) Incidence of transitional cell carcinoma and arsenic in drinking water: a follow-up study of 8,102 residents in an arseniasis-endemic area in northeastern Taiwan. Am J Epidemiol 153:411–418
Kurttio P, Pukkala E, Kahelin A, Auvinen A, Pekkanen J (1999) Arsenic concentrations in well water and risk of bladder and kidney cancer in Finland. Environ Health Perspect 107:705–710
Garland M, Morris JS, Colditz GA, et al (1996) Toenail trace element levels and breast cancer: a prospective study. Am J Epidemiol 144:653–660
Pershagen G (1985) Lung cancer mortality among men living near an arsenic-emitting smelter. Am J Epidemiology 122:684–694
Hazelton WD, Leubeck EG, Heidenreich WF, Moolgavkar SH (2001) Analysis of a historical cohort of Chinese tin miners with arsenic, radon, cigarette smoke, and pipe smoke exposures using the biologically based two-stage clonal expansion model. Radiation Research 156:78–94
Mabuchi K, Lilienfeld AM, Snell LM (1980) Cancer and occupational exposure to arsenic: a study of pesticide workers. Prev Med 9:51–77
Coggon D, Pannett B, Acheson ED (1984) Use of job-exposure matrix in an occupational analysis of lung and bladder cancers on the basis of death certificates. JNCI 72:61–65
Bates MN, Smith AH, Cantor KP (1995) Case–control study of bladder cancer and arsenic in drinking water. Am J Epidemiology 141:523–530
Steinmaus C, Yuan Y, Bates MN, Smith AH (2003) Case–control study of bladder cancer and drinking water arsenic in the western United States. Am J Epidemiol 158:1193–1201
Michaud DS, Wright ME, Cantor KP, Taylor PR, Virtamo J, Albanes D (2004) Arsenic concentrations in prediagnostic toenails and the risk of bladder cancer in a cohort of male smokers. Am J Epidemiol 160:835–859
U.S. Department of Health and Human Services, Public Health Service, National Toxicology Program (2002) Report on Carcinogens, 10th edn. 2002 December
McMurray CT, Tainer JA (2003) Cancer, cadmium and genome integrity. Nature Genetics 34:239–241
Waalkes MP (2000) Cadmium carcinogenesis in review. J Inorg Chem 79:241–244
Zheng H, Liu J, Choo KH, Michalska AE, Klaassen CD (1996) Metallothionein-I and -II knock-out mice are sensitive to cadmium-induced liver mRNA expression of c-jun and p53. Toxicol Appl Pharmacol 136:229–235
Abshire MK, Buzard GS, Shiraishi N, Waalkes MP (1996) Induction of c-myc and c-jun proto-oncogene expression in rat L6 myoblasts by cadmium is inhibited by zinc preinduction of the metallothionein gene. J Toxicol Environ Health 48:359–377
Shimada H, Shiao YH, Shibata M, Waalkes MP (1998) Cadmium suppresses apoptosis induced by chromium. J Toxicol Environ Health 54:159–168
Lemen RA, Lee JS, Wagoner JK, Blejer HP (1976) Cancer mortality among cadmium production workers. Ann NY Acad Sci 271:273–279
Sorahan T, Watherhouse JAH (1983) Mortality study of nickel–cadmium battery workers by the method of regression models in life tables. Br J Ind Med 40:293–300
Elinder CG, Kjellstrom T, Hogstedt C, Andersson K, Spang G (1985) Cancer mortality of cadmium workers. Br J Ind Med 42:651–655
Sorahan T (1987) Mortality from lung cancer among a cohort of nickel cadmium battery workers: 1946–84. Br J Ind Med 44:803–809
Kazantzis G, Lam TH, Sullivan KR (1988) Mortality of cadmium-exposed workers. Scand J Work Environ Health 14:220–223
Stayner L, Smith R, Thun M, Schnorr T, Lemen R (1992) A dose-response analysis and quantitative assessment of lung cancer risk and occupational cadmium exposure. Ann Epidemiol 2:177–194
Sorahan T, Lister A, Gilthorpe MS, Harrington JM (1995) Mortality of copper cadmium alloy workers with special reference to lung cancer and non-malignant diseases of the respiratory system, 1946–92. Occup Environ Med 52:804–812
West DW, Slattery ML, Robison LM, French TK, Mahoney AW (1991) Adult dietary intake and prostate cancer risk in Utah: a case–control study with special emphasis on aggressive tumors. Cancer Causes Control 2:85–94
Platz EA, Helzlsouer KJ, Hoffman SC, Morris JS, Baskett CK, Comstock GW (2002) Prediagnostic toenail cadmium and zinc and subsequent prostate cancer risk. Prostate 52:288–296
Armstrong BG, Kazantzis G (1985) Prostatic cancer and chronic respiratory and renal disease in British cadmium workers: a case–control study. Br J Ind Med 42:540–545
Miki H, Kasprzak KS, Kenney S, Heine UI (1987) Inhibition of intercellular communication by nickel (II): antagonistic effect of magnesium. Carcinogensis 8:1757–1760
DiPaolo JA, Casto BC (1979) Quantitative studies of in vitro morphological transformation of Syrian hamster cells by inorganic metal salts. Cancer Res 39:1008–1013
Biedermann KA, Landolph JT (1987) Induction of anchorage independence in human diploid foreskin fibroblasts by carcinogenic metal salts. Cancer Res 47:3815–3823
Patierno SR, Dirscherl L, Xu J (1993) Transformation of rat tracheal epithelial cells to immortal growth variants by particulate and soluble nickel compounds. Mutat Res 300:179–193
Costa M (1996) Mehcanisms of nickel genotoxicity and carcinogenicity. In: Chang LW (eds) Toxicology of metals. CRC Press, Boca Raton, FL, pp 245–251
Sen P, Conway K, Costa M (1987) Comparison of the localization of chromosome damage induced by calcium chromate and nickel compounds. Cancer Res 47:2142–2147
Kasprzak KS (1991) The role of oxidative damage in metal carcinogenicity. Chem Res Toxicol 4:604–615
Hartwig A, Mullenders LHF, Schlepegrell R, Kasten U, Beyersmann D (1994) Nickel (II) interferes with the incision step in nucleotide excision repair in mammalian cells. Cancer Res 54:4045–4051
Lee YW, Klein CB, Kargacin B, et al (1995) Carcinogenic nickel silences gene expression by chromatin condensation and DNA methylation: a new model for epigenetic carcinogens. Mol Cell Biol 15:2547–2557
Grimsrud TK, Berge SR, Haldorsen T, Andersen A (2002) Exposure to different forms of nickel and risk of lung cancer. Am J Epidemiol 156:1123–1132
Grimsrud TK, Berge SR, Martinsen JI, Andersen A (2003) Lung cancer incidence among Norwegian nickel-refinery workers 1953–2000. J Environ Monit 5:190–197
Karjalainen S, Kerttula R, Pukkala E (1992) Cancer risk among workers at a copper/nickel smelter and nickel refinery in Finland. Int Arch Occup Environ Health 63:547–551
D Pang DCL Burges T Sorahan (1996) ArticleTitleMortality study of nickel platers with special reference to cancers of the stomach and lung, 1945–93 Occup Environ Med 53 714–717 Occurrence Handle8943838 Occurrence Handle1:CAS:528:DyaK28XmvVaku7o%3D
Jarup L, Bellander T, Hogstedt C, Spang G (1998) Mortality and cancer incidence in Swedish battery workers exposed to cadmium and nickel. Occup Environ Med 55:755–759
Andersen A, Berge SR, Engeland A, Norseth T (1996) Exposure to nickel compounds and smoking in relation to incidence of lung and nasal cancer among nickel refinery workers. Occup Environ Med 53:708–713
Goldhaber SB (2003) Trace element risk assessment: essentiality vs. toxicity. Regul Toxicol Pharmacol 38:232–242
van’t Veer P, van der Wielen RP, Kok F, Hermus RJ, Sturmans F (1990) Selenium in diet, blood and toenails in relation to breast cancer: a case–control study. Am J Epidemiol 131:987–994
van’t Veer P, Strain JJ, Fernandez-Crehuet J, et al (1996) Tissue antioxidants and postmenopausal breast cancer: the European Community Multicentre Study on Antioxidants, Myocardial Infarction, and Cancer of the Breast (EURAMIC). Cancer Epidemiol Biomark Prev 5:441–447
Ghadirian P, Maisonneuve P, Perret C, et al (2000) A case-control study of toenail selenium and cancer of the breast, colon, and prostate. Cancer Detection Prev 24: 305–313
van Noord PA, de Waard F, Collette C, Mass MJ (1987) Selenium levels in nails of premenopausal breast cancer patients assessed prediagnostically in a cohort-nested case-referent study among women screened in the DOM project. Int J Epidemiol 16: 318–322
Hunter DJ, Morris JS, Stampfer MJ, Colditz GA, Speizer FE, Willett WC (1990) A prospective study of selenium status and breast cancer risk. JAMA 264:1128–1131
van den Brandt PA, Goldbohm RA, van’t Veer P, et al (1994) Toenail selenium and risk of breast cancer. Am J Epidemiol 140:20–26
Strain JJ, Bokje E, van’t Veer P, et al (1997) Thyroid hormones and selenium status in breast cancer. Nutr Cancer 27:48–52
Coates RJ, Weiss NS, Daling JR, Morris JS, Labbe RF (1988) Serum levels of selenium and retinol and the subsequent risk of cancer. Am J Epidemiol 128:515–523
Schrauzer GN, Molenaar T, Mead S, Kuehn K, Yamamoto H, Araki E (1985) Selenium in the blood of Japanese and American women with and without breast cancer and fibrocystic disease. Jpn J Cancer Res 76:374–377
Willett WC, Polk BF, Morris JS, et al (1983) Prediagnostic serum selenium and risk of cancer. Lancet 2:130–134
Longnecker MP, Stampfer MJ, Morris JS, et al (1993) A 1-y trial of the effect of high-selenium bread on selenium concentrations in blood and toenails. Am J Clin Nutr 57:408–413
Morris JS, Stampfer MJ, Willett WC (1983) Dietary selenium in humans. Toenails as an indicator. Biol Trace Elem Res 5:529–537
Clark LC, Hixson LJ, Combs GF Jr, Reid ME, Turnbull BW, Sampliner RE (1993) Plasma selenium concentration predicts the prevalence of colorectal adenomatous polyps. Cancer Epidemiol Biomark Prev 2:41–46
Fernandez-Banares F, Cabre E, Esteve M, et al (2002) Serum selenium and risk of large size colorectal adenomas in a geographical area with a low selenium status. Am J Gastroenterol 97:2103–2108
Nomura A, Heilbrun LK, Morris JS, Stemmermann GN (1987) Serum selenium and the risk of cancer, by specific sites: case–control analysis of prospective data. JNCI 79:103–108
Wallace K, Byers T, Morris JS, et al (2003) Prediagnostic serum selenium concentration and the risk of recurrent colorectal adenoma: a nested case–controls study. Cancer Epidemiol Biomark Prev 12:464–467
Garland M, Morris JS, Stampfer MJ, et al (1995) Prospective study of toenail selenium levels and cancer among women. J Natl Cancer Inst 87:497–505
Mannisto S, Alfthan G, Virtanen M, Kataja V, Uusitupa M, Pietinen P (2000) Toenail selenium and breast cancer – a case–control study in Finland. Eur J Clin Nutr 54:98–103
van den Brandt PA, Goldbohm RA, van’t Veer P, et al (1993) A prospective cohort study on toenail selenium levels and risk of gastrointestinal cancer. JNCI 85:224–229
Kabuto M, Imai H, Yonezawa C, et al (1994) Prediagnostic serum selenium and zinc levels and subsequent risk of lung and stomach cancer in Japan. Cancer Epidemiol Biomark Prev 3:465–469
Ratnasinghe D, Tangrea JA, Forman MR, et al (2000) Serum tocopherols, selenium and lung cancer risk among tin miners in China. Cancer Causes Control 11:129–135
Reid ME, Duffield-Lillico AJ, Garland L, Turnbull BW, Clark LC, Marshall JR (2002) Selenium supplementation and lung cancer incidence: an update of the nutritional prevention of cancer trial. Cancer Epidemiol Biomark Prev 11:1285–1291
Hartman TJ, Taylor PR, Alfthan G, et al (2002) Toenail selenium concentration and lung cancer in male smokers. Cancer Causes Control 13:923–928
van den Brandt PA, Goldbohm RA, van’t Veer P, et al (1993) A prospective study on selenium status and the risk of lung cancer. Cancer Res 53:4860–4865
Nakaji S, Fukuda S, Sakamoto J, et al (2001) Relationship between mineral and trace element concentrations in drinking water and gastric cancer mortality in Japan. Nutr Cancer 40:99–102
Kneller RW, Guo WD, Hsing AW, et al (1992) Risk factors for stomach cancer in sixty-five Chinese counties. Cancer Epidemiol Biomark Prev 1:113–118
Chen SY, Liu TY, Shun CT, et al (2004) Modification effects of GSTM1, GSTT1 and CYP2E1 polymorphisms on associates between raw salted food and incomplete intestinal metaplasia in a high-risk area of stomach cancer. Int J Cancer 108:606–612
Zhang L, Blot WJ, You WC, et al (1994) Serum micronutrients in relation to pre-cancerous gastric lesions. Int J Cancer 56:650–654
Knekt P, Aromaa A, Maatela J, et al (1990) Serum selenium and subsequent risk of cancer among Finnish men and women. JNCI 82:864–868
Wei WQ, Abnet CC, Qiao YL, et al (2004) Prospective study of serum selenium concentrations and esophageal and gastric cardia cancer, heart disease, stroke, and total death. Am J Clin Nutr 79:80–85
Mark SD, Qiao YL, Dawsey SM, et al (2000) Prospective study of serum selenium levels and incident esophageal and gastric cancers. J Natl Cancer Inst 92:1753–1763
Dawsey SM, Wang GQ, Taylor PR, et al (1994) Effects of vitamin/mineral supplementation on the prevalence of histological dysplasia and early cancer of the esophagus and stomach: results from the Dysplasia Trial in Linxian, China. Cancer Epidemiol Biomark Prev 3:167–172
Wang GQ, Dawsey SM, Li JY, et al (1994) Effects of vitamin/mineral supplementation on the prevalence of histological dysplasia and early cancer of the esophagus and stomach: results from the General Population Trial in Linxian, China. Cancer Epidemiol Biomark Prev 3:161–166
Helzlsouer KJ, Comstock GW, Morris JS (1989) Selenium, lycopene, alpha-tocopherol, beta-carotene, retinol, and subsequent bladder cancer. Cancer Res 49:6144–6148
Zeegers MP, Goldbohm A, Bode P, van den Brandt PA (2002) Prediagnostic toenail selenium and risk of bladder cancer. Cancer Epidemiol Biomark Prev 11:1292–1297
Michaud DS, Hartman TJ, Taylor PR, et al (2002) No association between toenail selenium levels and bladder cancer risk. Cancer Epidemiol Biomark Prev 11:1505–1506
Vogt TM, Ziegler RG, Graubard BI, et al (2003) Serum selenium and risk of prostate cancer in US blacks and whites. Int J Cancer 103:664–670
Allen NE, Morris JS, Ngwenyama RA, Key TJ (2004) A case–control study of selenium in nails and prostate cancer risk in British men. Br J Cancer 90:1392–1396
Brooks JD, Metter EJ, Chan DW, et al (2001) Plasma selenium level before diagnosis and the risk of prostate cancer development. J Urol 166: 2034–2038
Helzlsouer KJ, Huang HY, Alberg AJ, et al (2000) Association between alpha-tocopherol, gamma-tocopherol, selenium, and subsequent prostate cancer. J Natl Cancer Inst 92:2018–2023
Nomura AMY, Lee J, Stemmermann GN, Combs GF Jr (2000) Serum selenium and subsequent risk of prostate cancer. Cancer Epidemiol Biomark Prev 9:883–887
Yoshizawa K, Willett WC, Morris SJ, et al (1998) Study of prediagnostic selenium level in toenails and the risk of advanced prostate cancer. JNCI 90:1219–1224
Li H, Stampfer MJ, Giovannucci EL, et al (2004) A prospective study of plasma selenium levels and prostate cancer risk. J Natl Cancer Inst 96:696–703
van den Brandt PA, Zeegers MPA, Bode P, Goldbohm RA (2003) Toenail selenium levels and the subsequent risk of prostate cancer: a prospective cohort study. Cancer Epidemiol Biomark Prev 12:866–871
Hartman TJ, Albanes D, Pietinen P, et al (1998) The association between baseline vitamin E, selenium, and prostate cancer in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study. Cancer Epidemiol Biomark Prev 7:335–340
Clark LC, Dalkin B, Krongrad A, et al (1998) Decreased incidence of prostate cancer with selenium supplementation: results of a double-blind cancer prevention trial. Br J Urol 81:730–734
Prasad AS, Halsted JA, Nadimi M (1961) Syndrome of iron deficiency anemia, hepatospenomegaly, hyopgonadism, dwarfism,and geophagia. Am J Med 31:532–546
Prasad AS, Miale A, Farid Z, Sandstead HH, Schulert AR (1963) Zinc metabolism in patients with the syndrome of iron deficiency anemia, hypogonadism and dwarfism. J Lab Clin Med 61:537–549
Prasad AS (1998) Zinc in human health: an update. J Trace Elem Exp Med 11:63–78
O’Connor JM (2001) Trace elements and DNA damage. Biochem Soc Trans 29:354–357
Leccia MT, Richard MJ, Favier A, Beani JC (1999) Zinc protects against ultraviolet A1-induced DNA damage and apoptosis in cultured human fibroblasts. Biol Trace Elem Res 69:177–190
Gupta SK, Shukla VK, Vaidya MP, Roy SK, Gupta S (1991) Serum trace elements and Cu/Zn ratio in breast cancer patients. J Surg Oncol 46:178–181
Adzersen KH, Jess P, Freivogel KW, Gerhard I, Bastert G (2003) Raw and cooked vegetables, fruits, selected micronutrients, and breast cancer risk: a case–control study in Germany. Nutr Cancer 46:131–137
Harris RWC, Key TJA, Silcocks PB, Bull D, Wald NJ (1991) A case–control study of dietary carotene in men with lung cancer and in men with other epithelial cancers. Nutr Cancer 15:63–68
Cocco PL, Carta P, Belli S, Picchiri GF, Flore MV (1994) Mortality of Sardinian lead and zinc miners: 1960–88. Occup Environ Med 51:674–682
Zhang ZF, Kurtz RC, Yu GP, et al (1997) Adenocarcinomas of the esophagus and gastric cardia: the role of diet. Nutr Cancer 27:298–309
Costello LC, Franklin RB, Tan M, Bagasra O (2005) Zinc and prostate cancer: a critical scientific, medical, and public interest issue (United States). Cancer Causes Control 16:901–915
Kolonel LN, Yoshizawa CN, Hankin JH (1988) Diet and prostatic cancer: a case–control study in Hawaii. Am J Epidemiol 127:999–1012
Leitzmann MF, Stampfer MJ, Wu K, Colditz GA, Willett WC, Giovannucci EL (2003) Zinc supplement use and risk of prostate cancer. J Natl Cancer Inst 95:1004–1007
Kristal AR, Stanford JL, Cohen JH, Wicklund K, Patterson RE (1999) Vitamin and mineral supplement use is associated with reduced risk of prostate cancer. Cancer Epidemiol Biomarkers Prev 8:887–892
Vlajinac HD, Marinkovic JM, Ilic MD, Kocev NI (1997) Diet and prostate cancer: a case–control study. Eur J Nutr 33:101–107
Author information
Authors and Affiliations
Corresponding author
Appendix 1
Appendix 1
Search strategy employed for each of the cancers of interest in Medline
Cancer of interest | Search terms |
|---|---|
Lung | Exp lung neoplasms |
Lung adj4 cancer$.tw | |
Lung adj4 neoplas$.tw | |
Lung adj4 carcinoma$.tw | |
Lung adj4 tumor$.tw | |
Colorectal | Exp colorectal neoplasms |
Colorectal adj4 cancer$.tw | |
Colorectal adj4 neoplas$.tw | |
Colorectal adj4 carcinoma$.tw | |
Colorectal adj4 tumor$.tw | |
Breast | Exp breast neoplasms |
Breast adj4 cancer$.tw | |
Breast adj4 neoplas$.tw | |
Breast adj4 carcinoma$.tw | |
Breast adj4 tumor$.tw | |
Stomach | Exp stomach neoplasms |
Stomach adj4 cancer$.tw | |
Stomach adj4 neoplas$.tw | |
Stomach adj4 carcinoma$.tw | |
Stomach adj4 tumor$.tw | |
Bladder | Exp bladder neoplasms |
Bladder adj4 cancer$.tw | |
Bladder adj4 neoplas$.tw | |
Bladder adj4 carcinoma$.tw | |
Bladder adj4 tumor$.tw | |
Prostate | Exp prostate neoplasms |
Prostate adj4 cancer$.tw | |
Prostate adj4 neoplas$.tw | |
Prostate adj4 carcinoma$.tw | |
Prostate adj4 tumor$.tw |
Appendix 2
Search strategy employed for each of the trace elements of interest in Medline
Trace element of interest | Search terms |
|---|---|
Selenium | Exp selenium |
Selenium compounds | |
Zinc | Exp zinc |
Zinc compounds | |
Arsenic | Exp arsenic |
Arsenic compounds | |
Cadmium | Exp cadmium |
Cadmium compounds | |
Nickel | Exp nickel |
Nickel compounds |
Rights and permissions
About this article
Cite this article
Silvera, S.A.N., Rohan, T.E. Trace elements and cancer risk: a review of the epidemiologic evidence. Cancer Causes Control 18, 7–27 (2007). https://doi.org/10.1007/s10552-006-0057-z
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s10552-006-0057-z