
Abstract
To determine the relationship between 25(OH) vitamin D levels and non-melanoma skin cancer (NMSC), we performed a nested case–control study in ambulatory, elderly men enrolled in the Osteoporotic Fractures in Men (MrOS) Study. Health habit and medical history, including self-reported history of NMSC were recorded and 25(OH)D levels were measured on serum collected at baseline from a random sample of Caucasian MrOS subjects. Mean age (73 ± 5), BMI, daily vitamin D and calcium intake were similar in the men with (n = 178) and without NMSC (n = 930), but higher levels of 25(OH)D were associated with a decreased risk of having a history of NMSC (P trend = 0.04). Men in the highest quintile of 25(OH)D (>30 ng/mL) had 47% lower odds of NMSC (95% CI: 0.30–0.93, p = 0.026) compared to those in the lowest quintile. Our results suggest that a diagnosis of NMSC is not a surrogate for adequate 25(OH)D levels or increased UV exposure, and high 25(OH)D levels may be associated with a reduced risk of NMSC.
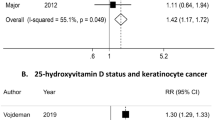
Similar content being viewed by others

Introduction
Non-melanoma skin cancer (NMSC) affects close to 1 million Americans annually. Although metastases are rare, their high incidence and frequent recurrence in affected individuals make NMSCs the 4th most costly cancers of the Medicare population [1]. NSMC is comprised of two subtypes—squamous cell carcinomas (SCC) and basal cell carcinomas (BCC). The majority of NMSCs are of the BCC subtype in older, white subjects (4:1 ratio of BCC:SCC) [2]. Public health education campaigns advocate sunscreen use and sun avoidance for prevention, but the incidence of NMSC continue to rise [2, 3].
NMSC is caused at least in part by sunlight [2] and sunlight is also the primary source of vitamin D [4]. The level of 25(OH)D, the major circulating form of vitamin D, is widely accepted as the best indicator of vitamin D status and vitamin D deficiency occurs if 25(OH)D levels are <20 ng/mL and insufficiency if <30 ng/mL. There is increasing evidence that vitamin D may be protective against cancers of the colon, breast, and prostate [5]. Observational data and one interventional clinical trial suggest that higher levels of 25(OH)D are associated with reduced visceral cancer risk [4, 6, 7]. Thus, based on the idea that the risk of NMSC is related to the amount of ultraviolet (UV) exposure, a diagnosis of NMSC has been used as a surrogate for high 25(OH)D levels [8–10, 11]. NMSC subjects have been hypothesized to have a reduced risk of visceral cancers, but the data are inconsistent. Two studies showed that NMSC subjects have a reduced risk of colorectal cancer [8, 10] while other studies show an increased risk for colorectal and visceral cancers [11, 12]. There has been no study comparing 25(OH)D levels and risk for NMSC. We initially hypothesized that NMSC subjects would have higher 25(OH)D levels given their chronic exposure to UV. To determine the association 25(OH)D levels and risk for NMSC, we conducted a nested case-control study in a cohort of elderly men.
Methods
Study participants
Subjects were participants in the Osteoporotic Fractures in Men Study (MrOS), a prospective cohort study of risk factors for fracture. During the baseline examination from March 2000 to April 2002, 5,995 community-dwelling men 65 years or older were recruited from population-based listings at six clinical centers in the United States: Birmingham, AL; Minneapolis, MN; Palo Alto, CA; Portland, OR; Pittsburgh, PA; and San Diego, CA. MrOS enrollees represent a relatively healthy and highly educated population [13, 14].
Analysis of serum 25(OH)D
At the baseline visit, 1,608 randomly selected MrOS participants had fasting morning blood collected, and serum was prepared immediately and stored at −70°C in vials foil-wrapped to prevent light exposure. Measures for 25(OH)D2 (derived from ergocalciferol and obtained from nutritional supplements and plants such as sun-dried mushrooms) and 25(OH)D3 (derived from cholecalciferol and obtained primarily from UV irradiation, fortified foods, and supplements) were performed at the Mayo Clinic Labs using LC-mass spectroscopy[15]. Duplicate pooled serum controls were included. The inter-assay coefficient of variation was 4.4% and the intra-assay coefficient of variation was 4.9%. Almost all circulating total 25(OH)D levels measured were due to 25(OH)D3 [16] and we define 25(OH)D as 25(OH)D3 in our analysis as we sought to measure endogenous vitamin D3 produced from UV irradiated skin. Levels of 25(OH)D2 were detected in 26% of samples and contributed to less than 10% of the total 25(OH) [16]. Because levels of 25(OH)D vary by race/ethnicity, we limited our analysis to Caucasian men (n = 1,441).
Non-melanoma skin cancer outcome and covariates
At the baseline and the 5-year follow-up visit, MrOS participants responded to a questionnaire item that inquired about having a history of NMSC (“Has a doctor or health care provider ever told you that you have skin cancer (not melanoma)” and asked their age at first NMSC diagnosis. 1,234 subjects out of 1,441 subjects had evaluable responses. We defined the group without NMSC as those participants who answered “no” to ever having skin cancer at both the baseline and 5-year visits (n = 930). We defined the NMSC group (n = 178) as those subjects who answered “yes” to ever having skin cancer at both the baseline and the 5-year visits or who answered “yes” to ever having NMSC at the 5-year visit and whose age at first skin cancer diagnosis was consistent with a diagnosis before the baseline visit. Incident NMSC cases (n = 100) were defined as those subjects who answered “no” to ever having skin cancer at baseline and “yes” to skin cancer at the 5 year visit and whose age a first skin cancer diagnosis was consistent with diagnosis after the baseline visit. Other studies have demonstrated that patient self-reported history of NMSC has a positive predictive value of 95.1% and a negative predictive value of 85.9% [17].
Covariates were obtained by self-administered questionnaire at the baseline visit [13, 14]. Physical activity was quantified using the physical activity scale for the elderly (PASE) and “walking outdoors” for exercise was used as a proxy for outdoor activity [18]. Total calcium and vitamin D intake (from foods and supplements) in the past 12 months were estimated using a modified block food frequency questionnaire (Block Dietary Data Systems, Berkeley, CA). UV exposure history of each subject was estimated by participant’s clinic site (to determine latitude) and walking outdoors physical activity [6]. UV exposure is a major confounder as increased UV exposure contributes to NMSC risk and raises 25(OH)D levels.
Statistical analysis
We used univariate and multivariable logistic regression to determine a dose-response association between serum 25(OH)D and odds of NMSC. Quintiles of 25(OH)D were based on the distribution of 25(OH)D in the NMSC and no NMSC groups. Odds of NMSC for quintiles Q2 through Q5 were compared with the lowest quintile. We calculated 95% confidence intervals and used the Mantel extension test to evaluate the presence of linear trend across quintiles. We tested for an interaction between 25(OH)D per ng/mL and each of the covariates; age, PASE walking score and clinic site for effect modification on the association of 25(OH)D3 with NMSC and reported the p value for interaction.
Results
Baseline characteristics for men with and without NSMC were similar in mean age (73.4 ± 5.5 years), BMI, smoking, education, calcium intake, and in their general health (Table 1). The mean value of 25(OH)D for the entire cohort was 23 ng/mL and consistent with reported values in the persons >70 years of age in the US population[16, 19]. Subjects with NMSC diagnosis had slightly lower levels of outdoor walking activity (p = 0.02) and minimally higher (22 IU) daily vitamin D intake (p = 0.05). The average age of skin cancer development was 61 ± 12 years, approximately 10 years prior to the median age at which blood for assessing vitamin D status was collected.
As a measure of consistency, we investigated the association of known predictors to serum 25(OH)D levels in univariate analyses. As expected, increasing age was significantly associated with decreasing 25(OH)D levels (p < 0.0001) [16] likely due to the age-related decline in vitamin D status due to decreasing amounts of the vitamin D precursor, 7-dehydrocholesterol in the skin [4]. Participants who resided near a clinic with higher UV exposure (San Diego) had higher levels of 25(OH)D compared to participants residing in clinics in Minnesota and Portland (p < 0.0001) as previously reported [16].
As a measure of internal validity, we examined the effect of a number of known risk factors for NMSC (Table 2). Subjects residing in Minneapolis or Portland versus San Diego had a reduced odds of NMSC (p < 0.004), consistent with other reports showing a lower incidence of NMSC in areas of low UV exposure [20]. Subject age was not associated with prevalent history of NMSC, perhaps because our subjects were of an older age range (65–78 years). BMI, cigarette smoking, and outdoor walking activity were not significantly associated with history of NSMC [2].
We found that higher quintiles of serum 25(OH)D levels are associated with decreased odds of NMSC when adjusting for age, BMI, season of blood draw, and clinic site (P trend = 0.032) (Table 3). This inverse association persisted in the multivariable model when cigarette smoking and outdoor walking activity were adjusted (P trend = 0.044). The majority of the effect was observed among men in the highest quintile of 25(OH)D who had a 47% lower odds of NMSC (OR: 0.53, 95% CI: 0.30–0.93, p = 0.026) compared to those in the lowest quintile in both multivariable models. A 40% reduction in the odds of NMSC was also detected when comparing Q5 versus Q1-4 (≥29.9 ng/mL) in both models. Findings were similar in analysis expressing 25(OH)D levels using standard clinical definitions [21, 22, 23]. Subjects who had sufficient levels of 25(OH)D (>32 ng/mL) had a 43% lower odds compared to subjects with insufficient levels (OR: 0.57, 95% CI: 0.33–0.98, p = 0.045) in the base model, and the association approached but did not reach statistical significance after further adjustment for walking and cigarette use. The association between 25(OH)D and NMSC risk was not significantly modified by age, clinic site, or walking activity (P interaction > 0.05).
There were relatively few incident NMSC cases (n = 100) during the 5 year follow-up period. When we compared subjects with 25(OH)D levels ≥32 ng/mL versus those with levels <32 ng/mL, we found trends suggesting a reduction of NMSC risk (OR: 0.72; 95% CI: 0.38–1.38, p = 0.33) in both base and multivariable models although this did not reach statistical significance.
Discussion
We have found that higher serum 25(OH)D levels are associated with a decreased risk of NMSC in older Caucasian men. To our knowledge, this is the first study to examine this association, and our data argue against the assumption that a NMSC diagnosis is a surrogate for increased UV exposure or elevated 25(OH)D levels. Studies in NMSC are difficult as these cancers are not reported in US national registries. One prior prospective cohort study on vitamin D intake from diet found no association between vitamin D and BCC risk [24]. One explanation for these differences is that our study measured 25(OH)D3 levels which primarily reflect vitamin D obtained from UV exposure and a smaller contribution from diet and supplements.
A major strength of this study is that we are using a large cohort of community dwelling men from diverse geographical regions for which we have information on season and lifestyle factors that may modify 25(OH)D levels and NMSC risk. In addition, 25(OH)D measurements were performed using mass spectroscopy, a more precise assay compared to other techniques [16, 25]. Our study had several limitations. NMSC outcome was ascertained through subject self-report and not histological confirmation, although most (but not all) previous investigators have reported a positive predictive value of 80–95% [17, 24, 26]. Our analyses were adjusted for several skin cancer risk factors such as smoking, amount of outdoor activity, and geographic residence but we did not have information on other skin cancer risk factors such as subject skin type, hair color, or eye color [2]. Differences in baseline pigmentation among case and non-case groups might affect skin cancer development and 25(OH)D as subjects with lighter skin color would have an increased risk for skin cancer but also an increased ability for cutaneous synthesis of vitamin D. Given the observational design, the possibility of residual confounding cannot be eliminated and we are unable to determine a causal inference between 25(OH)D levels and NMSC risk.
Our results suggest that subjects with 25(OH)D >32 ng/ml appear to have a 40% lower risk of NMSC and perhaps raising the 25(OH)D levels may be protective. Laboratory studies have also shown that vitamin D may be protective as 1.25(OH)D2 inhibits SCC cell lines, and mice deleted for the vitamin D receptor exhibit SCC and BCC tumors [27, 28]. Consistent with this hypothesis, we detected a trend of reduced risk of incident NMSC among subjects with higher 25(OH)D levels. Another possible explanation is that NMSC subjects may have lower 25(OH)D levels due to sun avoidance behaviors after their NMSC diagnosis. A prospective study of 25(OH)D and incident NMSC cases is needed to further explore the possible protective effect of vitamin D on non-melanoma skin cancer.
References
Chen JG et al (2001) Cost of nonmelanoma skin cancer treatment in the united states. Dermatol Surg 27(12):1035–1038
Rubin AI, Chen EH, Ratner D (2005) Basal-cell carcinoma. N Engl J Med 353(21):2262–2269
Corona R et al (2001) Risk factors for basal cell carcinoma in a Mediterranean population: role of recreational sun exposure early in life. Arch Dermatol 137(9):1162–1168
Holick MF (2007) Vitamin D deficiency. N Engl J Med 357(3):266–281
Giovannucci E (2009) Vitamin D and cancer incidence in the Harvard cohorts. Ann Epidemiol 19(2):84–88
Giovannucci E et al (2006) Prospective study of predictors of vitamin D status and cancer incidence and mortality in men. J Natl Cancer Inst 98(7):451–459
Lappe JM et al (2007) Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr 85(6):1586–1591
Soerjomataram I et al (2008) Are patients with skin cancer at lower risk of developing colorectal or breast cancer? Am J Epidemiol 167(12):1421–1429
Srikanth V et al (2007) The association between non-melanoma skin cancer and osteoporotic fractures–a population-based record linkage study. Osteoporos Int 18(5):687–692
Nugent Z et al (2005) Risk of second primary cancer and death following a diagnosis of nonmelanoma skin cancer. Cancer Epidemiol Biomarkers Prev 14(11 Pt 1):2584–2590
Milan T et al (2007) Subsequent primary cancers after basal-cell carcinoma: a nationwide study in Finland from 1953 to 1995. Int J Cancer 87(2):283–288
Chen J et al (2008) Nonmelanoma skin cancer and risk for subsequent malignancy. J Natl Cancer Inst 100(17):1215–1222
Orwoll E et al (2005) Design and baseline characteristics of the osteoporotic fractures in men (MrOS) study–a large observational study of the determinants of fracture in older men. Contemp Clin Trials 26(5):569–585
Blank JB et al (2005) Overview of recruitment for the osteoporotic fractures in men study (MrOS). Contemp Clin Trials 26(5):557–568
Singh RJ et al (2006) C-3 epimers can account for a significant proportion of total circulating 25-hydroxyvitamin D in infants, complicating accurate measurement and interpretation of vitamin D status. J Clin Endocrinol Metab 91(8):3055–3061
Orwoll E et al (2009) Vitamin D deficiency in older men. J Clin Endocrinol Metab 94(4):1214–1222
Ming ME et al (2004) Validity of patient self-reported history of skin cancer. Arch Dermatol 140(6):730–735
Washburn RA et al (1993) The physical activity scale for the elderly (PASE): development and evaluation. J Clin Epidemiol 46(2):153–162
Yetley EA (2008) Assessing the vitamin D status of the US population. Am J Clin Nutr 88(2):558S–564S
Qureshi AA et al (2008) Geographic variation and risk of skin cancer in US women. Differences between melanoma, squamous cell carcinoma, and basal cell carcinoma. Arch Intern Med 168(5):501–507
Institute of Medicine (1997) Dietary references intakes for calcium, phosphorous, magnesium, vitamin D and fluoride. National Academy Press, Washington, DC
Bischoff-Ferrari HA et al (2006) Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr 84(1):18–28
Neuhouser ML et al (2008) Vitamin D insufficiency in a multiethnic cohort of breast cancer survivors. Am J Clin Nutr 88(1):133–139
van Dam RM et al (2000) Diet and basal cell carcinoma of the skin in a prospective cohort of men. Am J Clin Nutr 71(1):135–141
Lips P et al (1999) An international comparison of serum 25-hydroxyvitamin D measurements. Osteoporos Int 9(5):394–397
Bergmann MM et al (1998) Validity of self-reported Cancers in a prospective cohort study in comparison with data from state cancer registries. Am J Epidemiol 147(6):556–562
Bikle DD (2004) Vitamin D and skin cancer. J Nutr 134(12 Suppl):3472S–3478S
Zinser GM, Sundberg JP, Welsh J (2002) Vitamin D(3) receptor ablation sensitizes skin to chemically induced tumorigenesis. Carcinogenesis 23(12):2103–2109
Acknowledgments
This publication was made possible by Grant Numbers 1K23AR056736-01 (NIAMS) and KL2 RR024130 (NCRR), a component of the NIH and NIH Roadmap for Medical Research, the Prevent Cancer Foundation, and the American Skin Association. The Osteoporotic Fractures in Men (MrOS) Study is supported by National Institutes of Health funding. The following institutes provide support: the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), the National Institute on Aging (NIA), the National Center for Research Resources (NCRR), and NIH Roadmap for Medical Research under the following grant numbers: U01 AR45580, U01 AR45614, U01 AR45632, U01 AR45647, U01 AR45654, U01 AR45583, U01 AG18197, U01-AG027810, and UL1 RR024140.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Tang, J.Y., Parimi, N., Wu, A. et al. Inverse association between serum 25(OH) vitamin D levels and non-melanoma skin cancer in elderly men. Cancer Causes Control 21, 387–391 (2010). https://doi.org/10.1007/s10552-009-9470-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-009-9470-4