
Abstract
Purpose Firstly, to give a review of characteristic indocyanine green angiographic (ICGA) signs in Vogt–Koyanagi–Harada (VKH) disease and, secondly, to determine the utility of ICG angiography in the assessment and follow-up of choroidal inflammatory activity during initial high-dose inflammation suppressive therapy and during the tapering of therapy.
Methods We have first reviewed characteristic ICGA signs in VKH. This is followed by a study of four patients with an acute initial VKH uveitis episode who received regular initial and follow-up angiographic examinations for at least 9 months. Classical ICGA signs were recorded at onset and followed for at least 9 months and were correlated with treatment levels. The treatment consisted of high-dose oral corticosteroids (0.8–1.5 mg/kg) preceded by pulse intravenous methylprednisolone (500–1000 mg) for 3 days in hyperacute cases and followed by very slow tapering with the addition of an immunosuppressive agent in cases of insufficient response.
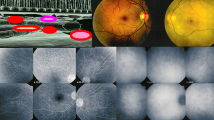
Results The major ICGA signs that were both consistently present and easy to record in the four VKH patients having an acute initial uveitis episode with a pre-treatment angiography and an angiographic follow-up for a minimum of 9 months include (1) early choroidal stromal vessel hyperfluorescence and leakage, (2) hypofluorescent dark dots, (3) fuzzy vascular pattern of large stromal vessels and (4) disc hyperfluorescence. All patients were treated with high-dose inflammation suppressive therapy: in two patients, within 14 and 21 days after initial symptoms, respectively, and in the other two patients, within 6 weeks. Hypofluorescent dark dots, the most constant and easily recordable sign, was very prominent in all cases at presentation. A 90% to complete resolution of dark dots was noted in all four patients after 4 months of therapy. The other three major angiographic signs, early choroidal stromal vessel hyperfluorescence and leakage, indistinct fuzzy vessels at the intermediate angiographic phase and disc hyperfluorescence resolved in all cases within 8 weeks or less of high-dose inflammation suppressive therapy. In three of the four patients, dark dots reappeared after a mean of 7.8 ± 2.8 months after onset of therapy when the patients were under a mean corticosteroid dose of 13.2 ± 6.3 mg per day without any significant clinical or fluorescein angiographic signs, indicating subclinical recurrence. An increase in the inflammation suppressive therapy again brought about angiographic resolution of choroidal subclinical disease in all cases.
Conclusion Choroidal inflammation shown by ICG angiography can be suppressed completely by initial high-dose inflammation suppressive therapy. However, recurrent subclinical choroidal inflammation is detected at the end of the tapering period in a high proportion of cases. This indicates that, in the absence of an ICGA follow-up, undetected smoldering subclinical disease may persist, thereby explaining the frequently reported evolution towards sunset glow fundus despite an apparently controlled disease. This is a clear indication that VKH disease should be followed by ICG angiography and, in the case of choroidal subclinical reactivation, a reversal of therapy tapering and an extension of therapy duration should be considered.







Similar content being viewed by others


References
Sugita S, Takase H, Taguchi C, Imai Y, Kamoi k, Kawaguchi T, Sugamoto Y, Futagami Y, Itoh K, Mochizuki M (2006) Ocular infiltrating CD4+ T cells from patients with Vogt–Koyanagi–Harada disease recognize human melanocyte antigens. Invest Ophthalmol Vis Sci 47:2547–2554
Damico FM, Cunha-Neto E, Goldberg AC, Iwai LK, Marin ML, Hammer J, Kalil J, Yamamoto JH (2005) T-cell recognition and cytokine profile induced by melanocyte epitopes in patients with HLA-DRB1*0405-positive and -negative Vogt–Koyanagi–Harada uveitis. Invest Ophthalmol Vis Sci 46:2465–2471
Foster DJ, Cano MR, Green RL, Rao NA (1990) Echographic features of the Vogt–Koyanagi–Harada Syndrome. Arch Ophthalmol 108:1421–1426
Bouchenaki N, Cimino L, Auer C, Tran VT, Herbort CP (2002) Assessement and classification of choroidal vasculitis in posterior uveitis using indocyanine green angiography. Klin Monatsbl Augenheilk 219:243–249
Khairallah M, Ben Yahia S, Attia S, Zaouali S, Jelliti B, Jenzri S, Ladjimi A, Messaoud R (2006) Indocyanine green angiographic features in multifocal chorioretinitis associated with West Nile virus infection. Retina 26:358–359
Machida S, Tanaka M, Murai K, Takahashi T, Tazawa Y (2004) Choroidal circulatory disturbance in ocular sarcoidosis without the appearance of retinal lesions or loss of visual function. Jpn J Ophthalmol 48:392–396
Dhingra S, Stavrou P (2004) Indocyanine green angiography in systemic lupus erythematosus-associated uveitis. Ocul Immunol Inflamm 12:69–73
Howe L Stanford M, Graham E, Marshall J (1998) Indocyanine green angiography in inflammatory eye diseases. Eye 12:761–767
Harada T, Kanbara Y,Takeuchi T, Niwa T, Majima T (1997) Exploration of Vogt-Koyanangi Harada syndrome by infrared choroidal angiography with indocyanine green. Eur J Ophthalmol 7:163–170
Ohshima Y, Harino S, Hara Y, Tona Y (1996) Indocyanine green angiographic findings in Vogt–Koyanagi–Harada disease. Am J Ophthalmol 122:58–66
Okada AA, Mizusawa T, Sakai J, Usui M (1998) Videofunduscopy and videoangiography using the scanning laser ophthalmoscope in Vogt–Koyanagi–Harada disease. Br J Ophthalmol 82:1175–1181
Bouchenaki N, Morisod L, Herbort CP (2000) Vogt–Koyanagi–Harada syndrome: importance of rapid diagnosis and therapeutic intervention. Klin Monatsbl Augenheilk 216:290–294
Bouchenaki N, Herbort CP (2001) The contribution of indocyanine green angiography to the appraisal and management of Vogt–Koyanagi–Harada. Ophthalmology 108:54–64
Bouchenaki N, Herbort CP (2000) Indocyanine green angiography (ICGA) in the assessement and follow-up of choroidal inflammation in active chronically evolving Vogt–Koyanagi–Harada disease. In: Dodds EM, Couto CA (eds) Uveitis in the third millennium. Elsevier Science, Amersterdam, pp 35–38
Herbort CP, Bodaghi B, LeHoang P (2001) Angiographie au vert d’indocyanine au cours des maladies oculaires inflammatoires: principes, interprétation schématique, sémiologie et intérêt clinique. J Fr Ophtalmol 24:423–447
Herbort CP, LeHoang P, Guex-Crosier Y (1998) Schematic interpretation of indocyanine green angiography in posterior uveitis using a standard protocol. Ophthalmology 105:432–440
Altan-Yaycioglu R, Akova YA, Akca S, Yilmaz G (2006) Inflammation of the posterior uvea: findings on fundus fluorescein and indocyanine green angiography. Ocul Immunol Inflamm 14:171–179
Chen L, Yang P, Wen F, Zhou H, Huang X (2002) Fundus fluorescein and indocyanine green angiographic study of Behçest’ disease and Vogt–Koyangi–Harada syndrome Zhonghua. Yan Ke Za Zhi 38:210–212
Kohno T, Miki T, Shiraki K, Kano K, Matsushita M, Hayashi K, Sw Laey JJ (1999) Substraction ICG angiography in Harada’s disease. Br J Ophthalmol 83:822–833
Tugal-Tutkun I, Ozyazgan Y, Akova, Sullu Y, Akyol N, Soylu M, Kazokoglu H (2006) The spectrum of Vogt–Koyanagi–Harada disease in Turkey. Int Ophthalmol. 7 September 2006 (Epub ahead of print)
Keino H, Goto H, Ususi M (2002) Sunset glow fundus in Vogt–Koyanangi–Harada disease with or without chronic ocular inflammation. Graefe’s Arch Clin Exp Ophthalmol 240:878–882
Yang P, Wang H, Zhou H. Huang X, Zhong H, Chen L, Fu T (2002) Clinical manifestations and diagnosis of Vogt–Koyanagi–Harada syndrome. Zonghua Yan Ke Za Zhi 38:736–739
Keino H, Goto H, Mori H, Iwasaki T,Ususi M (2006) Association between severity of inflammation in CNS and development of sunset glow fundus in Vogt–Koyanagi–Harada disease. Am J Ophthalmol 141:1140–1142
Suzuki S (1999) Quantitative evaluation of “sunset glow” fundus in Vogt–Koyanagi–Harada disease. Jpn J Ophthalmol 43:327–333
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Herbort, C.P., Mantovani, A. & Bouchenaki, N. Indocyanine green angiography in Vogt–Koyanagi–Harada disease: angiographic signs and utility in patient follow-up. Int Ophthalmol 27, 173–182 (2007). https://doi.org/10.1007/s10792-007-9060-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-007-9060-y