Abstract
The goal of the current study is to examine the relationship amongst social support, stress, and depressive symptoms within a transactional and diathesis-stress framework using a multi-wave, longitudinal design. At the initial assessment, adolescents (n = 258) completed self-report measures assessing social support (peer, classmate, parent, and total), dependent interpersonal stress, anxious symptoms, and depressive symptoms. Additionally, participants reported stress and symptomology in each of the four waves spanning six months. Results of time-lagged, idiographic, multilevel modeling indicated that stress mediated the relationship between lower parental, classmate, and total social support and subsequent depressive, but not anxious, symptoms. In contrast, lower levels of peer support were not associated with higher levels of stress and subsequent depressive symptoms. Additionally, only classmate support deficits significantly moderated the relationship between stress and depressive symptoms. Overall, the results suggest that deficits in parental and classmate support may play a greater role in contributing to adolescent depression as compared to deficits in peer support.
Similar content being viewed by others


Adolescence is a period marked by rapid change, transition, and growth in which many individuals experience depressive symptoms (Hankin et al. 2007). By the age of 18 approximately 15–25% of adolescents will have experienced a major depressive episode (Lewinsohn and Essau 2002), however, subclinical levels of depressive symptoms are also a concern given their association with negative outcomes including academic difficulties, impaired cognitive functioning, and interpersonal instability (Avenevoli et al. 2008; Hammen et al. 2008, 1999). One of the most robust concurrent and prospective predictors of depressive symptomology is stress (Grant et al. 2004). However, even severe stress is not linked to psychopathology in all individuals. Consequently, researchers have begun to examine integrative models with the aim of better understanding the underlying relationship between vulnerability factors, stress, and depressive symptomology. One such factor that plays a prominent role in the development, onset, and maintenance of adolescent depression is perceived social support (e.g., Stice et al. 2004).
Social Support
Research examining the role of social support amongst adolescents has found that lower levels of social support are associated with higher levels of depressive symptoms (Crocker and Hakim-Larson 1997; Ellonen et al. 2008). To date, the majority of adolescent social support research has relied on either main effect or diathesis-stress models (e.g., Stice et al. 2004). In general, cross-sectional investigations have demonstrated that low levels of perceived social support, operationalized with respect to the quality of a given relationship, predict greater depressive symptoms in adolescents (Bogard 2005; Field et al. 2001). Research has also indicated that particular domains of social support play a differential role with respect to the manifestation of depressive symptomology. Bogard (2005) found that greater perceived parental support was associated with lower levels of depressive symptoms. Expanding on this research, Eldeleklio•lu and colleagues (2006) compared the role of parental versus peer support, and results indicated that greater peer support was more strongly associated with reductions in depressive symptoms relative to parental support. Taken together, these studies highlight the importance of examining how social support exerts its influence, especially as it relates to domain as well as over time.
While the preponderance of research has been cross-sectional, these designs are not well suited to make causal inferences about the prospective relationship between vulnerability factors and the subsequent developmental unfolding of depressive symptomology (Riskind and Alloy 2006). Consequently, some other research has begun to examine the prospective relationship between social support and depressive symptomology in adolescence (e.g., Allen et al. 2006; Henrich and Shahar 2008). Kendler et al. (2005) found that low levels of global social support predicted greater risk for major depression. With respect to peer support, research has indicated that such support is not a consistent predictor of symptoms over time (Lewinsohn et al. 1994; Windle 1992). Leadbeater et al. (1999) found that adolescent girls, but not boys, with low levels of parental support reported higher levels of depressive symptoms. However, additional prospective research indicated that greater parental social support predicted attenuated depressive symptoms in both boys and girls (Boutelle et al. 2009; Needham, 2008; Sheeber et al. 1997). Overall, there is inconsistent cross-sectional and prospective evidence for a main effect of social support on depression in adolescence. As these inconsistencies in research findings may be due to the fact that social support predicts changes in depressive symptoms under some circumstances but not others, researchers have begun to explore circumstances in which the relationship between social support and such symptoms may be particularly strong.
In an effort to address past inconsistencies regarding the association between social support and depressive symptoms, as well as develop a more comprehensive understanding of the circumstances under which social support predicts depressive symptoms, recent research has begun to examine such support in adolescence using a diathesis-stress approach (Harkness et al. 2006). While the diathesis-stress framework was originally employed to better understand the relationship between cognitive vulnerability, stress, and depression (for review see Gibb and Coles 2005), more recent research has explored an array of vulnerability factors including biological (serotonin transporter gene—Risch et al., 2009), personality (neuroticism—Kendler et al. 2004), and even cultural (materialism—Auerbach et al. 2010b) variables. With respect to examining the underlying role of social support, the diathesis-stress model posits that lower levels of perceived social support confer vulnerability to depressive symptoms following the occurrence of stressful life events. Within the context of this framework, social support may have a twofold role. On the surface, lacking sufficient social support may limit an individual’s ability to effectively manage interpersonal difficulties, and thus, contribute to interpersonal loss. Further, the presence of stress and simultaneous absence of support may also increase one’s awareness that they do not possess adequate social support, which potentially triggers to a sense of aloneness. As both loss and aloneness are two core themes that arise in the context of adolescent depression, it is an interesting perspective to consider. Recent research examining social support within a diathesis-stress framework has begun to pay particular attention to different domains of support. For example, Stice and colleagues (2004) found that lower parental, but not peer support, predicted increases in depressive symptoms as well as the onset of major depression following the occurrence of stress. In addition, several studies have also indicated that neither parental nor peer support significantly moderated the relationship between stress and depressive symptoms (e.g. Burton et al. 2004; Shu-Guang et al. 2006). At the same time, given the paucity of such research on adolescents, studies are warranted to better understand the role that domains of social support play in the context of a diathesis-stress framework in adolescent samples.
By utilizing a diathesis-stress framework, there has been greater clarity regarding circumstances in which social support may impact depressive symptoms. Along these lines, more recent research has also begun to employ transactional models, which incorporate a stress generation framework, to conceptualize vulnerability to depression (see Auerbach et al. 2010a; Eberhart and Hammen 2010). In general, the diathesis-stress model posits that the occurrence of stress activates underlying diatheses or vulnerabilities, and further, the interaction between premorbid vulnerability factors and stress contributes to higher levels of depressive symptoms. A diathesis-stress model is effective in examining individual difference variables; however, it implicitly assumes that (a) individuals are passive recipients of stress and (b) vulnerability factors are dormant in the absence of stress. Conversely, the transactional approach posits that individuals actively contribute to the occurrence of stressors they experience through a process labeled stress generation (Hammen, 1991). Such stress generation may then result in higher levels of depressive symptoms (e.g., Auerbach et al. 2010a; Shih et al. 2009). The majority of research examining stress generation has been conducted amongst adult samples (e.g., Hammen 1991), however, there has been accumulating evidence of stress generation amongst adolescents (Auerbach et al. 2010; Rudolph 2008; Wingate and Joiner 2004). Consistent with this approach, we would hypothesize that lower quality of perceived social support would predict higher levels of stress, irrespective of domain, as the lack of support in these different environmental and interpersonal contexts would likely result in a greater occurrence of stress. More specifically, individuals who do not feel supported by peers, classmates, or parents may act in ways that create interpersonal conflict as they pursue the support they feel is lacking. For example, adolescents who perceive the support they are receiving as insufficient may paradoxically generate interpersonal discord by continually demanding additional support from their network. Along similar lines, adolescents who possess fewer social supports likely rely more heavily on specific relationships, which may burden and tax these select individuals and thereby contribute to interpersonal stress. Further, given the strong relationship between stress and depression (see Hammen 2006), stress would then contribute to higher levels of subsequent depressive symptoms.
Goals of the Current Study
The present study aimed to address empirical and theoretical gaps regarding the relationship between social support, stress, and depressive symptoms using a 6-month multi-wave, longitudinal design in a sample of adolescents. Such an approach allows us to examine the time-lagged relationship between vulnerability factors, stress, and depressive symptoms, and thus, more clearly delineates the role that social support plays regarding the emergence of such symptoms. To date, cross-sectional and prospective main effect models have examined the relationship between social support and depressive symptoms in adolescence. However, results have been mixed regarding the role that domain-specific support plays in the manifestation of depressive symptoms. Markedly less research has examined the relationship of social support in the context of a diathesis-stress framework, and to our knowledge, no research has examined social support utilizing a transactional perspective.
Consequently, the goals of the present study are as follows. Regarding our primary aim, we sought to examine different domains of social support including parents, peers, and classmates using both a diathesis-stress and transactional perspective. It is important to note that diathesis-stress (i.e., moderation) and the transactional (i.e., mediation) perspectives are not competing models as either one or both may explain the relationship among social support, stress, and depressive symptoms. To date, research has not clearly elucidated which type of support consistently predicts changes in depressive symptoms over time. In examining these models, the study focused on dependent interpersonal stressors, as such stressors are highly predictive of depressive symptoms and episodes in adolescence (e.g., Shih et al. 2006), and have been emphasized in both transactional (e.g., Hankin et al. 2005; see Hammen 2006, for a review) and diathesis-stress (e.g., Mazure et al. 2000; Shahar et al. 2004) models of depression. Indeed, stress generation effects are particularly strong for interpersonal stressors (e.g., Hammen 1991). Furthermore, our examination of interpersonal stressors is particularly germane given our exploration of the role that social support, an interpersonal factor, plays regarding the manifestation of depressive symptoms. Thus, we hypothesized that (a) social support deficits would moderate the relationship between higher levels of stress and depressive symptoms and (b) dependent interpersonal stress would mediate the relationship between social support deficits and depressive symptoms.
Our secondary aim examined model specificity. Specifically, there is a marked overlap between depressive and anxious symptoms (Seligman and Ollendick 1998) as well as depressive and anxious disorders (odds ratio = 8.2) (Angold et al. 1999). While a number of researchers have suggested that the high rate of comorbidity between anxious and depressive symptoms may be an artifact of overlapping symptom criteria or the splitting of a unitary latent construct into two or more categories, Seligman and Ollendick (1998) hypothesize that the co-occurrence of such symptoms may be explained by common etiological factors that increase the probability that both disorders will occur. As there is clinical utility in examining unique vulnerability factors for depression, we also examined model specificity in order to better understand whether our proposed models differentially predict fluctuations in depressive as opposed to anxious symptoms over the course of the study.
Method
Participants
Participants in the current study were recruited from high schools in Montreal, Canada. The sample included 258 adolescents (42.6% male and 57.4% female) between the ages of 12 and 18 (Mean = 14.48; SD = 1.47). The sample was 79.5% Caucasian, 8.0% Asian, 4.8% African American, 1.5% Hispanic, and 6.0% reported other as their ethnicity. Participants’ predominant mother tongues were English (76.2%) and French (11.8%).
Procedure
Approval for the study was granted by the university ethics board, and the treatment of participants was in accordance with APA ethical standards. Prior to the initial assessment, letters of informed consent were sent home to parents describing the aims of the project and requesting consent for their child to participate. In the present study, all students who received parental consent also gave personal consent. During the initial assessment, which occurred on school grounds during class time, students completed a demographics form and the following questionnaires: (1) Center for Epidemiologic Studies Depression Scale (Radloff 1977), (2) Multidimensional Anxiety Scale for Children—Short Form (March 1997), (3) Adolescent Life Event Questionnaire—Revised (Hankin and Abramson 2002), and (4) the Social Support Scale for Children and Adolescents (Harter 1985). Follow-up assessments occurred every 6 weeks for 6 months (Times 2–5) on school grounds during class time and participants completed self-report measures assessing negative events, depressive symptoms, and anxious symptoms. The average rate of retention for each follow-up during the course of the study was 82%, and each participant completed at least three assessments.
Assessments were spaced close enough together to enable participants to accurately recall events that had occurred within their life but far enough apart such that individuals would experience changes in their levels of stress and symptoms. Within such research, 4–6 weeks has become the most commonly used time interval between the initial and follow-up assessments (see Abela and Hankin 2008). At the conclusion of the study, all participants were provided a cognitive-behavioral skills workshop that (a) discussed the project aims, (b) taught evidenced-based skills to challenge maladaptive patterns of thinking, and (c) offered counseling services within the greater Montreal area for individuals in need.
Measures
Center for Epidemiologic Studies Depression Scale (CES-D; Radloff 1977)
The CES-D is a 20-item self-report measure that assesses levels of depressive symptoms. Examples of questions include: “I felt sad,” “I felt hopeless about the future,” and “I felt lonely.” Items on the scale ranged from 0 to 3 with possible total scores ranging from 0–60, and higher scores reflect greater depressive symptomology. The CES-D has been shown across numerous studies to have strong test-retest reliability and high correlations with other measures of depressive symptoms (Radloff 1991). While the CES-D was administered every 6 weeks, participants reported how they felt during the past week by using the following scale: rarely (<1 day), some or a little of the time (1–2 days), occasionally or a moderate amount of time (3–4 days), and most or all of the time (5–7 days). Across administrations the Cronbach’s alpha ranged from 0.92 to 0.94 which indicates high internal consistency.
Multidimensional Anxiety Scale for Children—Short Form (MASC-SF; March 1997)
The MASC-SF is a 10-item measure that assesses severity of anxious symptoms in the past week. Each item consists of a statement such as “I feel restless or on edge” or “I’m afraid that other kids will make fun of me” that participants rate on a four-point Likert scale ranging from 0 (never applies to me to) to 3 (often applies to me) and possible total scores ranged from 0–30. Past research has indicated that the MASC-SF has satisfactory test-retest reliability and validity (March et al. 1999). In the present study, the Cronbach’s alpha ranged from 0.71 to 0.81 which indicates moderate to moderately high internal consistency.
Adolescent Life Events Questionnaire—Revised (ALEQ; Hankin and Abramson 2002)
The ALEQ is a 57-item self-report questionnaire that was developed to assess a broad range of negative life events occurring in the past month. Past research has found that the ALEQ is both reliable and valid (Hankin and Abramson 2002). A consensus team consisting of three advanced doctoral students and one postdoctoral fellow rated whether each item was (a) dependent (i.e., at least in part dependent on the actions of the individual) and (b) interpersonal. A significant body of previous life stress research examining children, adolescents, and adults has used a similar consensus rating method to assess whether stressors are dependent and interpersonal in nature (e.g., Eberhart and Hammen 2009; Hammen 1991; Rudolph and Hammen 1999; Shih et al. 2006). This research, which is based on life stress interviews, initially conducted continuous ratings of independence, finding inter-team reliability ratings ranging from 0.85 to 0.97 across studies, but dichotomized the variable into dependent versus independent for all analyses. Early research using the consensus rating methodology found 100% agreement on ratings of whether events were interpersonal (Hammen 1991), such that later research has not found it necessary to assess the reliability of this categorization. The current study applied this consensus rating method developed for interviews to questionnaire items, adopting the dichotomized approach to dependence ratings. A total of 29 items were rated as both dependent and interpersonal, and examples of items are “You fought with your parents over your personal goals, desires, or choice of friends” and “A close friend did not treat you as well as he/she used to.” The items identified as both dependent and interpersonal in the current study are consistent with those identified in previous research on adolescents (e.g., Shih et al. 2006), which similarly emphasized conflict with parents and peers. Participants were asked to indicate how often such events occurred on a Likert scale ranging from 0 (never) to 4 (always) with possible total scores ranging from 0–116, and higher scores reflect a greater number of negative life events. In the current study, Cronbach’s alphas for the dependent interpersonal items ranged from 0.88 to 0.90.
The Social Support Scale for Children and Adolescents (SSSCA; Harter 1985)
The SSSCA is an 18-item self-report questionnaire. Each item requires the participant to first choose between two statements that best reflects the type of person they are more like. Then, the participant is asked to determine whether the chosen statement is “really true for me” or “sort of true for me.” Item scores range from 0–3, and higher scores are indicative of a higher perceived quality of social support. Possible total scores range from 0–54, and for each subscale, the possible range is from 0 to 18. The SSSCA assesses perceived social support in the domains of peer, parent, and classmate relationships with lower scores representing less perceived social support. Peer support describes general non-specific friendship and questions included, “Some kids have a close friend who they can tell problems to” versus “Other kids don’t have a close friend who they can tell problems to.” In contrast, classmate support examines relationships as it relates to general support as well as peer victimization in the classroom and/or school. Questions include (a) “Some kids have classmates they can become friends with” versus “Other kids don’t have classmates that they can become friends with” and (b) “Some kids have classmates who sometimes make fun of them” versus “Other kids don’t have classmates who make fun of them.” Parent support delineates how caring, sympathetic, and accommodating an individual’s parents may be. For example, a participant indicates whether “Some kids have parents who don’t seem to want to hear about their children’s problems” or “Other kids have parents who do want to listen to their children’s problems.” The SSSCA possesses moderately high internal consistency with coefficient alphas of subscales ranging from 0.74 to 0.88 in adolescent samples, and additionally, social support subscales are moderately correlated with measures of self-worth indicating satisfactory predictive validity (Harter 1985). In the present study, the Cronbach’s alpha for each subscale was as follows: (a) Total = 0.75, (b) Peer = 0.54, (c) Classmate = 0.68, and (d) Parent = 0.70.
Overview of Data Analytic Approach
To examine our proposed mediation models (i.e., the transactional perspective), we utilized idiographic, time-lagged multilevel modeling in which time was nested within individuals and followed the guidelines for multilevel mediation analyses set forth by Bauer et al. (2006). Such an approach is ideal for examining mediation models that include repeated measures, and given that the model is estimated in a single equation, one can directly estimate the covariance of the random effects that are encompassed in different Level 1 and Level 2 models (see Auerbach et al. 2010a). Consequently, Bauer and colleagues’ (2006) data analytic approach is preferable to mediation models that utilize a step-by-step process which makes the implicit assumption that each of the steps is independent (e.g., Baron and Kenny 1986; Kenny et al. 2003). In order to examine our lower level mediation model with a single equation, it was necessary to use a selection variable, Z, by stacking Y and M (i.e., the dependent variable and mediator) for each occasion of measurement (i.e., time), indexed by i, within individuals, indexed by j (Bauer et al. 2006). By using a single outcome variable, we can then fit a multivariate model using a univariate model approach. However, given that Z may represent different outcome variables (i.e., depressive/anxious symptoms and dependent interpersonal), it is also necessary to create two separate selection variables, SM and SY. Thus, when Z represents the mediator (i.e., dependent interpersonal stress), SM is set to equal 1 while SY is set to equal 0. In contrast, if Z is the dependent variable (i.e., depressive/anxious symptoms), then SY is equal to 1 and SM is 0. An example of the single, simultaneous model is belowFootnote 1:
To examine whether dependent interpersonal stress(Time T-1) mediated the relationship between social support and depressive/anxious symptoms(Time T), analyses were carried out using SAS (version 9.2) mixed procedure and maximum likelihood estimation. Our dependent variable was either within-subject fluctuations in depressive or anxious symptoms(Time T) which is a Level 1 variable. The primary predictor of depressive or anxious symptoms(Time T) was social support, a between-subject and Level 2 variable, and the mediator was within-subject fluctuations of dependent interpersonal stress(Time T-1), a Level 1 variable. Each domain of social support was examined separately. The mediation effect of dependent interpersonal stress is given by a*bj, and the 95% confidence interval (CI) is computed following the formula presented in Bauer et al. (2006). The mediation effect is considered statistically significant if zero is not included in the CI. Five additional effects were also included in this initial mean structure. First, in order to control for individual differences in baseline levels of depressive or anxious symptoms, participant’s initial depressive or anxious symptoms was included in the model. Second, in order to provide a more conservative examination of our hypotheses, we controlled for anxious symptoms throughout the follow-up period when predicting depressive symptoms. Conversely, when estimating models for anxious symptoms, we controlled for depressive symptoms throughout the course of the study. Third, in order to account for individual variability in the average level of depressive or anxious symptoms at his/her mean level of dependent interpersonal stress a random effect for intercept was included in the model. Fourth, given that dependent interpersonal stress is a within-subject predictor whose effect is expected to vary from participant to participant, a random effect for slope was included in the model. Last, age and gender were included as covariates in all estimated models.
To test our diathesis-stress (i.e., moderation) hypothesis that individuals possessing lower levels of social support (i.e., minus 1.5 between-subject standard deviations) would report greater increases in depressive or anxious symptoms(Time T) following the occurrence of dependent interpersonal stressors(Time T-1) than individuals possessing higher levels of social support (i.e., plus 1.5 between-subject standard deviations), we also utilized idiographic, time-lagged, multilevel modeling. Similar to the transactional model above, each domain of social support was examined separately. Again, our dependent variable was within-subject fluctuations in depressive or anxious symptoms(Time T) during the follow-up interval. Our primary predictors/moderators of follow-up depressive or anxious symptom(Time T) scores were social support and fluctuations in dependent interpersonal stress(Time T-1) during the follow-up interval. Similar to the mediation model described above baseline symptom scores, applicable follow-up depressive or anxious symptoms, a random slope, a random intercept, age, and gender were included in the model.
Results
Descriptive Data
Means, standard deviations, and intercorrelations between all Time 1 measures are included in Table 1. Additionally, descriptive statistics for depressive and anxious symptoms during the follow-up period are presented in Table 2.
Social Support Domains as Predictors of Depressive and Anxious Symptomology
Multilevel modeling analyses were conducted to examine whether social support domains (i.e., total, peer, classmate, and parent) predicted fluctuations in depressive or anxious symptoms over the follow-up period (see Table 3). Baseline depressive/anxious symptoms, age, and gender were entered in the first step of all analyses as covariates. This first step was the same for all the analyses. In the second step, each type of social support was individually examined in a series of separate models. All models utilized an autoregressive covariance structure and a random intercept which were significant (p < 0.001). Results indicated that low total (p < 0.01), classmate (p < 0.001), and parent (p < 0.01) social support predicted high levels of depressive symptoms, however, depressive symptom levels did not vary as a function of peer social support. In contrast, none of the social support domains predicted significant changes in anxious symptoms over time. Such a relationship is essential within a mediation model, and thus, no further analyses examining anxious symptoms in the context of the transactional model were conducted.
Social Support Domains as Predictors of Dependent Interpersonal Stress
Similar to the analyses described above, main effect models examined whether social support domains predicted changes in dependent interpersonal stress throughout the follow-up period (see Table 4). In step one of the analyses, we included age and gender as covariates. This first step was the same for all the analyses. In the second step, each domain of social support was examined individually and analyzed in a series of separate models. All models utilized an autoregressive covariance structure and a random intercept which were significant (p < 0.001). Results indicated that total (p < 0.001), classmate (p < 0.001), and parent (p < 0.001) social support predicted changes in dependent interpersonal stress, however, peer social support did not predict such changes over time.
Dependent Interpersonal Stress as Predictors of Depressive Symptoms
The autoregressive covariance structure and random intercept were significant (p < 0.05), and after controlling for baseline depressive symptoms in the first step (b = 7.24, SE = 0.40, t(245) = 18.05, p < 0.001), higher levels of dependent interpersonal stress significantly predicted higher levels of depressive symptoms (b = 0.06, SE = 0.12, t(626) = 2.06, p < 0.01).
Transactional Analyses Predicting Depressive Symptoms
Given the associations between (a) social support and depressive symptoms, (b) social support and dependent interpersonal stress, and (c) dependent interpersonal stress and depressive symptoms, we examined whether dependent interpersonal stress mediated the relationship between social support and depressive symptoms using Bauer and colleagues’ (2006) single equation simultaneous approach (see Fig. 1). It is important to note that each domain of social support was examined separately. All models included an autoregressive heterogeneous covariance structure (p < 0.0001) as well as appropriate random effects for slope and intercept. Of primary importance, a number of significant mediation models emerged. First, consistent with our preliminary main effect analyses, lower levels of total social support predicted higher levels of dependent interpersonal stress over time (path a: b = −3.19, SE = 0.73, t(1396) = 4.39, p < 0.01). When controlling for the proportion of variance accounted for by dependent interpersonal stress(Time T-1) in predicting changes in follow-up depressive symptoms(Time T) (path b j : b = 0.07, SE = 0.02, t(1396) = 3.28, p < 0.01), high levels of dependent interpersonal stress(Time T-1) partially mediated the relationship between low levels of total support and high levels of depressive symptoms(Time T) (b = −1.38, SE = 0.44, t(1396) = 3.12, p < 0.01). The 95% CI (path a*b j : b = 0.24, SE = 0.09; 0.06, 0.43) suggests that the mediation effect is significant. Second, when examining the single, simultaneous model, lower parent parental support predicted higher levels of dependent interpersonal stress over time (path a: b = −4.14, SE = 0.69, t(1406) = 5.97, p < 0.001). Additionally dependent interpersonal stress(Time T-1) (path b j : b = 0.08, SE = 0.02, t(1406) = 3.25, p < 0.01) partially mediated the relationship between parent support and depressive symptoms(Time T) (b = −1.07, SE = 0.45, t(1406) = 2.36, p < 0.05). Again, the 95% CI (path a*b j : b = 0.31, SE = 0.11; 0.09, 0.54) indicates that the mediation effect is significant. Third, lower classmate social support predicted a greater occurrence of dependent interpersonal stress over time (path a: b = −2.23, SE = 0.72, t(1410) = 3.09, p < 0.01). Further, dependent interpersonal stress(Time T-1) (path b j : b = 0.07, SE = 0.02, t(1410) = 3.07, p < 0.01) partially mediated the relationship between classmate support and depressive symptoms(Time T) (b = −1.63, SE = 0.44, t(1410) = 3.68, p < 0.001). The 95% CI (path a*b j : b = 0.15, SE = 0.07; 0.01, 0.29) suggests that the mediation model was significant. Last, as peer social support did not predict changes in depressive symptoms over time, mediation analyses were not conducted.

Sample time-lagged mediation model examining the relationship between support, dependent interpersonal stress(Time T-1), and depressive symptoms(Time T)
Examining the Diathesis-Stress Approach to Predict Depressive Symptoms
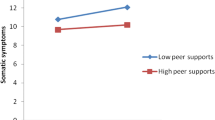
In our first set of time-lagged moderation analyses, we were interested in examining the effects of the social support scores and dependent interpersonal stress(T-1) on individual’s follow-up depressive symptoms(Time T). Each of the models was estimated separately and included a significant first-order autoregressive covariance parameter and random intercept (p < 0.001). The random slopes were not significant, and consequently, they were removed from the model prior to re-estimation. Of primary importance, a significant two-way, cross-level interaction emerged between classmate social support and follow-up dependent interpersonal stress(T-1). More specifically, while follow-up dependent interpersonal stress(T-1) was associated with increases in follow-up depressive symptoms(Time T) for individuals possessing low (b = 0.09, SE = 0.03, t(498) = −1.69, p < 0.01) and high (b = −0.14, SE = 0.06, t(498) = 2.23, p < 0.05) levels of classmate social support, the effect was strong for individuals who reported low classmate support . It is important to note that the slope of these two groups significantly differed (b = −0.08, SE = 0.03, t(498) = −2.34, p < 0.05) (see Fig. 2). In contrast, a significant two-way, cross-level interaction did not emerge between (a) total social support and dependent interpersonal stress(Time T-1) (b = −0.04, SE = 0.04, t(493) = −1.19, ns), (b) peer social support and dependent interpersonal stress(Time T-1) (b = −0.05, SE = 0.04, t(495) = −1.59, ns), and (c) parent social support and dependent interpersonal stress(Time T-1) (b = −0.03, SE = 0.04, t(496) = 0.71, ns).

Predicted depressive symptom scores as a function of classmate social support and dependent interpersonal stress
Secondary Aim: Examining the Diathesis-Stress Approach to Predict Anxious Symptoms
When examining model specificity, social support domains did not moderate the association between dependent interpersonal stress(Time T-1) and subsequent anxious symptoms(Time T). More specifically, significant two-way, cross-level interactions did not emerge between dependent interpersonal stress(Time T-1) and (a) total social support (b = 0.02, SE = 0.01, t(508) = 1.51, ns), (b) peer social support (b = −0.01 SE = 0.02, t(510) = −0.78, ns), (c) classmate social support (b = −0.002, SE = 0.02, t(513) = −0.15, ns) or (d) parent social support (b = 0.02, SE = 0.03, t(511) = 1.60, ns).
Discussion
Social support is an integral part of adolescent well-being as it addresses an individual’s need to feel loved, valued, and esteemed (Cobb 1976). However, it is unclear exactly how, or through which mechanisms, social support exerts an impact on depressive and anxious symptomology in the context of dependent interpersonal stress. To date, research has primarily relied on cross-sectional and two time point designs, and has yielded inconsistent results regarding which domains of social support buffer and/or confer vulnerability to psychopathology. The present study sought to address important empirical and methodological gaps by examining social support using two prevailing theoretical frameworks in depression research, a diathesis-stress and a transactional approach, within the context of a multi-wave, longitudinal design. More specifically, we examined whether the interplay of social support domains and dependent interpersonal stress differentially impacted the manifestation of depressive and anxious symptomology.
Transactional Model: Exploring Social Support, Stress Generation, and Depressive Symptoms
The stress generation framework posits that individuals are not passive recipients of stress (Hammen 1991). Rather, individuals possess specific characteristics and engage in particular behaviors which actively shape the type of stressors they experience. In line with the stress generation framework, the present study found that adolescents who possess low parental, classmate, and total social support experienced a greater occurrence of dependent interpersonal stress. Further, dependent interpersonal stress partially mediated the relationship between lower social support and greater subsequent depressive symptoms. Overall, our findings underscore the importance of supportive parents and classmates. Specifically, maternal support is thought to be particularly critical in early adolescence (Vaughan et al. 2010), and additional research suggests that parental emotional and informational support buffers adolescent distress (Malecki and Demaray 2003). As school becomes more of a focus in adolescents’ lives, supportive classmates may become more critical for mental health (Demaray and Malecki 2002a). In fact, greater classmate support, which is operationalized as fostering supportive relationships in the classroom or at school, is associated with better clinical and personal adjustment as well as school-related outcomes (Demaray and Malecki 2002b). The current findings are an extension of past research as we examined the time-lagged relationship amongst social support, stress, and depressive symptomology over time as compared to examining cross-sectional or prospective main effect models (e.g., Allen et al. 2006; Stice et al. 2004). Consequently, the findings further delineate the stress generation pathway through which social support exerts its influence on depressive symptoms.
In contrast to our hypothesis, results indicated that lower peer support, or a failure to develop close peer relationships or a network of friends, is not associated with dependent interpersonal stress or depressive symptoms over time. Such findings are consistent with recent research. More specifically, Vaughan and colleagues (2010) found that lower levels of peer social support were significantly associated with higher levels of depressive symptoms at age 12, however, after controlling for maternal support, peer support no longer predicted changes in such symptoms suggesting that there may be a social support hierarchy of importance during early adolescence. Additionally, when examining the importance of peer social support across middle adolescence, such support did not account for the growth trajectory of depressive symptoms (Vaughan et al. 2010). Coupled with the present findings, these results suggest that peer support has little or no influence on the manifestation of depressive symptoms. At the same time, it is likely that social support “needs” vary as one matures through adolescence and into young adulthood. For example, Friedlander and colleagues (2007) found that perceived social support from friends as opposed to family predicted better adjustment in first-year undergraduate students who were primarily living in residence at university. Therefore, while the present study suggests that peer support does not influence symptom fluctuation, it appears that such support plays a more paramount role when young adults become more dependent on friendships to help manage interpersonal stressors.
Diathesis-Stress Framework
When examining moderation models with respect to social support, stress, and depressive symptoms, existing research has typically explored two different but related frameworks. The stress-buffering framework suggests that greater social support attenuates the relationship between stress and depressive symptoms (Wheaton 1983). To date, the stress-buffering hypothesis has received scant support as 69 of 72 prospective tests have resulted in null findings (see Burton et al. 2004). Less research has examined the diathesis-stress framework which focuses on the relationship between social support deficits, stress, and the occurrence of depressive symptoms. Burton and colleagues (2004) indicated that neither parental support nor peer support deficits interacted with stress to predict changes in depressive symptoms over time. Consistent with these past findings, our diathesis-stress results indicated that peer, parent, and total support deficits did not moderate the relationship between stress and depressive symptoms.
Conversely, lower classmate support significantly moderated the relationship between the occurrence of dependent interpersonal stress and subsequent depressive symptoms. One possible explanation for these findings is that adolescence is a period fraught with developmental and pubertal challenges rendering many individuals susceptible to experience dependent interpersonal stressors in school with classmates and teachers (Demaray and Malecki 2002a). For individuals who do not possess supportive classmates, our findings suggest that this lack of support increases the likelihood of experiencing higher levels of depressive symptoms following the occurrence of dependent interpersonal stress. Alternatively, our assessment of classmate support overlaps, in part, with victimization and bullying (e.g., “some kids have classmates who sometimes make fun of them”). Rigby (2000) suggests that there is a strong association between bullying and social support deficits. More specifically, bullying, which invariably gives rise to relational tensions in school settings, is thought to intensify social support deficits resulting in increased risk of negative psychosocial outcomes. Thus, it seems that for some, there may be an interaction effect between classmate support and bullying leaving vulnerable individuals in a double bind (i.e., poorer classmate support and greater bullying). Taken together, these findings suggest that supportive school environments likely play a critical role in maintaining adolescent well-being, and thus, provide further support for school-based prevention and intervention programs (see Spence 2008).
Model Specificity: An Examination of Anxious Symptoms
Research indicates that there are common etiological pathways that may account for the emergence of depressive and anxious symptoms (Seligman and Ollendick 1998), thus highlighting the importance of examining model specificity. In line with our hypothesis, the present findings indicate that social support does not influence anxiety symptom fluctuation when examining such support in the context of either a transactional or a diathesis-stress perspective. One possibility for these findings is that individuals who report greater levels of anxiety have a tendency to engage in more avoidant-based behaviors. Such behaviors may have three important consequences: (a) the tendency to avoid social interactions, (b) a greater likelihood of having smaller social networks, and (c) a pattern of isolation (see Turk et al. 2001). Given these consequences, individuals may have fewer social interactions resulting in less opportunity to generate dependent interpersonal stress and subsequent anxiety. Further, as a result of this self-imposed isolation, an individual’s reported anxiety may be “artificially low.” Rather it is likely a reflection of one’s symptom level while avoiding as opposed to engaging with his/her environment. While the present study focused on the occurrence of dependent interpersonal stress, which is consistent with the stress generation framework, it is likely that avoidance triggers or is associated with different types of stressors in one’s life. Therefore, it may be important to re-examine the interplay of social support, stress, and anxious symptoms and include achievement and evaluative stressors that are not contingent on social interactions but may benefit from social support.
Limitations
There are a number of strengths to the current study including a large sample size retained over repeated follow-up assessments, a multi-wave methodology, and a rigorous data analytic approach. At the same time, there are several limitations that merit additional attention. First, the present study utilizes self-report measures in order to assess social support, depressive symptoms, and anxious symptoms. As self-report measures are prone to response bias, future research would benefit from utilizing peer and/or parent ratings as well as semi-structured interviews. Additionally, as the internal consistency of perceived social support, specifically, peer support was lower than previous studies, it may be beneficial to utilize experimental or observational techniques to assess such support in future studies. Second, Hammen and Shih (2008) posit that there are a number of methodological problems that arise when using self-report measures of stress including but not limited to difficulties disentangling objective versus subjective threat and potential gender biases regarding women’s tendency to report an event as more stressful as compared to men. Further, it is recommended that researchers utilize a contextual threat rating system to determine whether these events crossed a specific threshold regarding objective severity. Past research suggests that such an approach is a reliable way to address potential methodological confounds (Brown and Harris 1978), and in doing so, one can ascertain whether stressors were dependent interpersonal or independent. Such a distinction is critical as the stress generation framework asserts that individuals are particularly vulnerable to dependent interpersonal stressors as opposed to independent stressors. As the present study utilized a negative event checklist, future research would benefit from using a contextual threat rating system in order to better examine the relationship between social support and stress generation. Third, the present study examined symptom fluctuation, and therefore, we could not delineate the relationship between social support and diagnoses of depression or anxiety. As diagnoses of depression and anxiety are associated with a multitude of negative short- and long-term outcomes (e.g., Avenevoli et al. 2008; Hammen et al. 2008), further research is warranted. Last, the present sample was recruited from several schools in the Montreal area, and participation was based on consent from both the student and parent/guardian. All students were encouraged to participate, however, reasons for nonparticipation were not assessed. While the present sample is in line with the greater demographic distribution of Quebec, it is not possible to determine if there were other differences between the participants and those who opted out of the present study. As these differences may have influenced our current findings, future research should include data regarding reasons for nonparticipation.
Future Directions and Clinical Implications
As twice as many adolescent girls will have experienced a depressive episode as compared to boys by the age of 14 (Hankin et al. 2007), research is warranted to better understand whether social support deficits contribute to such differences. In general, Landman-Peeters and colleagues (2005) found that social support may be more important to adolescent girls as interpersonal stressors have been found to be stronger predictors of negative psychological outcomes in adolescent girls relative to boys. Similarly, research has indicated that adolescent girls report larger social networks (Henrich et al. 2001), and further, in comparison to boys, girls are more likely to utilize such networks for emotional support to attenuate stress and depressive symptoms (Taylor et al. 2000). Therefore, future research would benefit from a more in depth examination of how gender shapes social support, stress, and subsequent symptoms.
Overall, the present study sought to examine an interpersonal model of depression using divergent theoretical approaches. The findings indicate that stress generation plays a primary role in the manifestation of depressive, but not anxious, symptoms. Specifically, classmate and parental support deficits appear to be particularly important vulnerability factors. These results have important clinical implications, as building adequate support networks in these specific domains may help to reduce one’s interpersonal stress, subsequently reducing the likelihood of experiencing distressing, depressive symptoms. In contrast, when examining social support within the context of a diathesis-stress framework, only classmate support deficits moderated the relationship between dependent interpersonal stress and depressive symptoms. While the diathesis-stress approach did not yield robust findings, it underscores the importance of classmate support. Consequently, helping vulnerable adolescents develop a more supportive interpersonal infrastructure in school may be an important target in school-based prevention and intervention programs.
Notes
The single, simultaneous models is from Bauer et al. (2006, p. 146).
References
Abela, J. R. Z., & Hankin, B. L. (2008). Handbook of depression in children and adolescents. New York: Guilford Press.
Allen, J. P., Insabella, G., Porter, M. R., Smith, F. D., Land, D., & Phillips, N. (2006). A social-interactional model of the development of depressive symptoms in adolescence. Journal of Consulting and Clinical Psychology, 74, 55–65.
Angold, A., Costello, E. J., & Erkanli, A. (1999). Comorbidity. Journal of Child Psychology and Psychiatry, 40, 57–87.
Auerbach, R. P., Eberhart, N. K., & Abela, J. R. Z. (2010a). Cognitive vulnerability to depression in Canadian and Chinese adolescents. Journal of Abnormal Child Psychology, 38, 57–68.
Auerbach, R. P., Webb, C. A., McWhinnie, C. M., Xiongzhao Zhu, & Shuqiao Yao. (Submitted November 2010b). Deconstructing the mechanism through which materialism impacts depressive and anxious symptoms. Journal of Clinical Child and Adolescent Psychology.
Avenevoli, S., Knight, E., Kessler, R. C., & Merikangas, K. R. (2008). Epidemiology of depression in children and adolescents. In J. R. Z. Abela & B. L. Hankin (Eds.), Handbook of depression in children and adolescents (pp. 6–32). New York: Guilford.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182.
Bauer, D. J., Preacher, K. J., & Gil, K. M. (2006). Conceptualizing and testing random indirect effects and moderated mediation in multilevel models: new procedures and recommendations. Psychological Methods, 11, 142–163.
Bogard, K. L. (2005). Affluent adolescents, depression, and drug use: the role of adults in their lives. Adolescence, 40, 281–306.
Boutelle, K., Eisenberg, M. E., Gregory, M. L., & Neumark-Sztainer, D. (2009). The reciprocal relationship between parent-child connectedness and adolescent emotional functioning over 5 years. Journal of Psychosomatic Research, 66, 309–316.
Brown, G. W., & Harris, T. (1978). Social origins of depression: a reply. Psychological Medicine, 8, 577–588.
Burton, E., Stice, E., & Seeley, J. R. (2004). A prospective test of the Stress-Buffering Model of depression in adolescent girls: no support once again. Journal of Consulting and Clinical Psychology, 72, 689–697.
Cobb, S. (1976). Social support as a moderator of life stress. Psychosomatic Medicine, 38, 300–314.
Crocker, A. D., & Hakim-Larson, J. (1997). Predictors of pre-adolescent depression and suicidal ideation. Canadian Journal of Behavioural Science/Revue canadienne des sciences du comportement, 29, 76–82.
Demaray, M. K., & Malecki, C. K. (2002a). Criticla levels of perceived social support associated with student adjustment. School Psychology Quarterly, 17, 213–241.
Demaray, M. K., & Malecki, C. K. (2002b). The relationship between perceived social support and maladjustment for students at risk. Journal of Clinical Child Psychology, 18, 52–64.
Eberhart, N. K., & Hammen, C. L. (2009). Interpersonal predictors of stress generation. Personality and Social Psychology Bulletin, 35, 544–556.
Eberhart, N. K., & Hammen, C. L. (2010). Interpersonal style, stress, and depression: an examination of transactional and diathesis-stress models. Journal of Social and Clinical Psychology, 29, 23–38.
Eldeleklio•lu, J. Kuram ve Uygulamada, E. B. (2006). The relationship between the perceived social support and level of depression and anxiety in university students. Kuram ve Uygulamada Egitim Biljmleri, 6, 742–752.
Ellonen, N., Kääriäinen, J., & Autio, V. (2008). Adolescent depression and school support: a multilevel analysis of a Finnish sample. Journal of Community Psychology, 36, 552–567.
Field, T., Diego, M., & Sanders, C. (2001). Adolescent depression and risk factors. Adolescence, 36, 491–498.
Friedlander, L. J., Reid, G. J., Shupak, N., & Cribbie, R. (2007). Social support, self-esteem, and stress as predictors of adjustment to university among first-year undergraduates. Journal of College Student Development, 48, 259–274.
Gibb, B., & Coles, M. (2005). Cognitive vulnerability-stress models of psychopathology: A developmental perspective. In: Development of psychopathology: A vulnerability-stress perspective (pp. 104–135). Thousand Oaks, CA: Sage Publications.
Grant, K. E., Compas, B. E., Stuhlmacher, A. F., Thurm, A. E., McMahon, S. D., & Halpert, J. A. (2004). Stressors and child and adolescent psychopathology: measurement issues and prospective effects. Journal of Clinical Child and Adolescent Psychology, 33, 412–425.
Hammen, C. (1991). Generation of stress in the course of unipolar depression. Journal of Abnormal Psychology, 100, 555–561.
Hammen, C. (2006). Stress generation in depression: reflections on origins, research, and future directions. Journal of Clinical Psychology, 62, 1065–1082.
Hammen, C., & Shih, J. H. (2008). Stress generation and depression. In K. S. Dobson & D. J. A. Dozois (Eds.), Risk factors in depression (pp. 409–428). New York: Elsevier.
Hammen, C., Rudolph, K., Weisz, J., Rao, U., & Burge, D. (1999). The context of depression in clinic-referred youth: neglected areas in treatment. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 64–71.
Hammen, C., Brennan, P. A., & Keenan-Miller, D. (2008). Pattern of adolescent depression to age 20: the role of maternal depression and youth interpersonal dysfunction. Journal of Abnormal Child Psychology, 36(8), 1189–1198.
Hankin, B. L., & Abramson, L. Y. (2002). Measuring cognitive vulnerability to depression in adolescence: reliability, validity, and gender differences. Journal of Clinical Child and Adolescent Psychology, 31, 491–504.
Hankin, B. L., Kassel, J. D., & Abela, J. R. Z. (2005). Adult attachment dimensions and specificity of emotional distress symptoms: prospective investigations of cognitive risk and interpersonal stress generation as mediating mechanisms. Personality and Social Psychology Bulletin, 31, 136–151.
Hankin, B. L., Mermelstein, R., & Roesch, L. (2007). Sex differences in adolescent depression: stress exposure and reactivity models. Child Development, 78, 279–295.
Harkness, K. L., Bruce, A. E., & Lumley, M. N. (2006). The role of childhood abuse and neglect in the sensitization to stressful life events in adolescent depression. Journal of Abnormal Psychology, 115, 730–741.
Harter, S. (1985). Manual for the social support scale for children and adolescents. Denver: University of Denver.
Henrich, C. C., & Shahar, G. (2008). Social support buffers the effects of terrorism on adolescent depression: findings from Sderot, Israel. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 1073–1076.
Henrich, C. C., Blatt, S. J., Kuperminc, G. P., Zohar, A., & Leadbeater, B. J. (2001). Levels of interpersonal concerns and social functioning in early adolescent boys and girls. Journal of Personality Assessment, 76, 48–67.
Kenny, D. A., Korchmaros, J. D., & Bolger, N. (2003). Lower level mediation in multilevel models. Psychological Methods, 8, 115–128.
Kendler, K. S., Kuhn, J., & Prescott, C. A. (2004). The interrelationship of neuroticism, sex, and stressful life events in the prediction of episodes of major depression. The American Journal of Psychiatry, 161, 631–636.
Kendler, K. S., Myers, M. S., & Prescott, C. A. (2005). Sex differences in the relationship between social support and risk for major depression: a longitudinal study of opposite-sex twin pairs. The American Journal of Psychiatry, 162, 250–256.
Landman-Peeters, K., Hartman, C., van der Pompe, G., den Boer, J., Minderaa, R., & Ormel, J. (2005). Gender differences in the relation between social support, problems in parent-offspring communication, and depression and anxiety. Social Science & Medicine, 60, 2549–2559.
Leadbeater, B. J., Kuperminc, G. P., Blatt, S. J., & Hertzog, C. (1999). A multivariate model of gender differences in adolescents’ internalizing and externalizing problems. Developmental Psychology, 35, 1268–1282.
Lewinsohn, P. M., & Essau, C. A. (2002). Depression in adolescents. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (pp. 541–559). New York: Guilford Press.
Lewinsohn, P. M., Roberts, R. E., Seeley, J. R., Rohde, P., Gotlib, I. H., & Hops, H. (1994). Adolescent psychopathology: II. Psychosocial risk factors for depression. Journal of Abnormal Psychology, 103, 302–315.
Malecki, C. K., & Demaray, M. K. (2003). What type of support do they need? Investigating student adjustment as related to emotional, informational, appraisal, and instrumental support. School Psychology Quarterly, 18, 231–252.
March, J. S. (1997). Multidimensional anxiety scale for children: Technical manual. Toronto: Multi-Health Systems.
March, J. S., Sullivan, K., & Parker, J. (1999). Test-retest reliability of the multidimensional anxiety scale for children. Journal of Anxiety Disorders, 13, 349–358.
Mazure, C. M., Bruce, M. L., Maciejewski, P. K., & Jacobs, S. C. (2000). Adverse life events and cognitive-personality characteristics in the prediction of major depression and antidepressant response. The American Journal of Psychiatry, 157, 896–903.
Needham, B. L. (2008). Reciprocal relationships between symptoms of depression and parental support during the transition from adolescence to young adulthood. Journal of Youth and Adolescence, 37, 893–905.
Radloff, L. S. (1977). The CES-D scale: a self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401.
Radloff, L. (1991). The use of the Center for Epidemiologic Studies Depression Scale in adolescents and young adults. Journal of Youth and Adolescence, 20, 149–166.
Rigby, K. (2000). Effects of peer victimization in schools and perceived social support on adolescent well-being. Journal of Adolescence, 23, 57–68.
Risch, N., Herrell, R., Lehner, T., Liang, K., Eaves, L., Hoh, J., et al. (2009). Interaction between the serotonin transporter gene (5-HTTLPR), stressful life events, and risk of depression: a meta-analysis. JAMA, the Journal of the American Medical Association, 301, 2462–2471.
Riskind, J. H., & Alloy, L. B. (2006). Cognitive vulnerability to emotional disorders: Theory and research design/methodology. In L. B. Alloy & J. H. Riskind (Eds.), Cognitive vulnerability to emotional disorders (pp. 1–32). New Jersey: Erlbaum.
Rudolph, K. D. (2008). Developmental influences on interpersonal stress generation in depressed youth. Journal of Abnormal Psychology, 117, 673–679.
Rudolph, K. D., & Hammen, C. (1999). Age and gender as determinants of stress exposure, generation, and reactions in youngsters: A transactional perspective. Child Development, 70, 660–677.
Seligman, L. D., & Ollendick, T. H. (1998). Comorbidity of anxiety and depression in children and adolescents: an integrative review. Clinical Child and Family Psychology Review, 1, 125–144.
Shahar, G., Joiner, T. E., Zuroff, D. C., & Blatt, S. J. (2004). Personality, interpersonal behavior, and depression: co-existence of stress-specific moderating and mediating effects. Personality and Individual Differences, 36, 1583–1596.
Sheeber, L., Hops, H., Alpert, A., Davis, B., & Andrews, J. (1997). Family support and conflict: prospective relations to adolescent depression. Journal of Abnormal Child Psychology, 25, 333–344.
Shih, J. H., Eberhart, N. K., Hammen, C. L., & Brennan, P. A. (2006). Differential exposure and reactivity to interpersonal stress predict sex differences in adolescent depression. Journal of Clinical Child and Adolescent Psychology, 35, 103–115.
Shih, J. H., Abela, J. R. Z., & Starrs, C. (2009). Cognitive and interpersonal predictors of stress generation in children of affectively ill parents. Journal of Abnormal Child Psychology, 37, 195–208.
Shu-Guang, W., Yue-Juan, Z., & Ming-Jing, X. (2006). The functioning mechanisms of social support and self-efficacy between stress and depression. Chinese Journal of Clinical Psychology, 14(3), 300–302.
Spence, S. (2008). Integrating individual and whole-school change approaches in the prevention of depression in adolescents. In J. R. Z. Abela & B. L. Hankin (Eds.), Handbook of depression in children and adolescents (pp. 333–353). New York: The Guilford Press.
Stice, E., Ragan, J., & Randall, P. (2004). Prospective relations between social support and depression: differential direction of effects for parent and peer support? Journal of Abnormal Psychology, 113, 155–159.
Taylor, S. E., Cousino-Klein, L., Lewis, B. P., Gruenewald, T. L., Gurung, R. A. R., & Updegraff, J. A. (2000). Biobehavioral responses to stress in females: tend-and-befriend, not fight-or-flight. Psychological Review, 107, 411–429.
Turk, C. L., Heimberg, R. G., & Hope, D. A. (2001). Social Anxiety Disorder. In D. H. Barlow (Ed.), Clinical handbook of psychological disorders (pp. 114–153). New York: The Guilford Press.
Vaughan, C. A., Foshee, V. A., & Ennett, S. A. (2010). Protective effects of maternal and peer support on depressive symptoms during adolescence. Journal of Abnormal Child Psychology, 38, 261–272.
Wheaton, B. (1983). Stress, personal coping resources, and psychiatric symptoms: an investigation of interactive models. Journal of Health and Social Behavior, 24, 208–229.
Windle, M. (1992). A longitudinal study of stress buffering for adolescent problem behaviors. Developmental Psychology, 28, 522–530.
Wingate, L. R., & Joiner, T. E. (2004). Depression-related stress generation: a longitudinal study of black adolescents. Behavior Therapy, 35, 247–261.
Author information
Authors and Affiliations
Corresponding author
Additional information
The research reported in this article was supported by a McGill University Social Sciences and Humanities Student Research Grant Awarded to Randy P. Auerbach and a Canadian Psychiatric Research Foundation (CPRF) awarded to John R.Z. Abela.
Rights and permissions
About this article
Cite this article
Auerbach, R.P., Bigda-Peyton, J.S., Eberhart, N.K. et al. Conceptualizing the Prospective Relationship Between Social Support, Stress, and Depressive Symptoms Among Adolescents. J Abnorm Child Psychol 39, 475–487 (2011). https://doi.org/10.1007/s10802-010-9479-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10802-010-9479-x