
Abstract
Objective
Identify and describe interventions to reduce time to reperfusion for patients with ST-segment elevation myocardial infarction (STEMI).
Data Source
Key word searches of five research databases: MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), EMBASE, Web of Science, and Cochrane Clinical Trials Registry.
Interventions
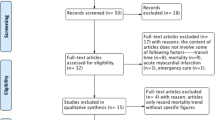
We included controlled and uncontrolled studies of interventions to reduce time to reperfusion. One researcher reviewed abstracts and 2 reviewed full text articles. Articles were subsequently abstracted into structured data tables, which included study design, setting, intervention, and outcome variables. We inductively developed intervention categories from the articles. A second researcher reviewed data abstraction for accuracy.
Measurements and Main Results
We identified 666 articles, 42 of which met inclusion criteria. We identified 11 intervention categories and classified them as either process specific (e.g., emergency department administration of thrombolytic therapy, activation of the catheterization laboratory by emergency department personnel) or system level (e.g., continuous quality improvement, critical pathways). A majority of studies (59%) were single-site pre/post design, and nearly half (47%) had sample sizes less than 100 patients. Thirty-two studies (76%) reported significantly lower door to reperfusion times associated with an intervention, 12 (29%) of which met or exceeded guideline recommended times. Relative decreases in times to reperfusion ranged from 15 to 82% for door to needle and 13–64% for door to balloon.
Conclusions
We identified an array of process and system-based quality improvement interventions associated with significant improvements in door to reperfusion time. However, weak study designs and inadequate information about implementation limit the usefulness of this literature.

Similar content being viewed by others

References
Thom T, Haase N, Rosamond W, et al. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006;113(6):e85–151.
Cannon CP, Bahit MC, Haugland JM, et al. Underutilization of evidence-based medications in acute ST elevation myocardial infarction: results of the Thrombolysis in Myocardial Infarction (TIMI) 9 registry. Critical Pathways in Cardiology. 2002;1(1):44–52.
Orlandini A, Diaz R, Wojdyla D, et al. Outcomes of patients in clinical trials with ST-segment elevation myocardial infarction among countries with different gross national incomes. Eur Heart J. 2006;27(5):527–33. Mar.
Cannon CP, Gibson M, Lambrew CT, et al. Relationship of time to treatment and door-to-balloon time to mortality in 27,080 patients with acute myocardial infarction treated with primary angioplasty. Circulation. 1999;100(18):1–360.
Cannon CP, Antman EM, Walls R, Braunwald E. Time as an adjunctive agent to thrombolytic therapy. J Thromb Thrombolysis. 1994;1(1):27–34.
Cannon CP, Gibson CM, Lambrew CT, et al. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000;283(22):2941–47.
De Luca G, van’t Hof AWJ, de Boer MJ, et al. Time-to-treatment significantly affects the extent of ST-segment resolution and myocardial blush in patients with acute myocardial infarction treated by primary angioplasty. Eur Heart J. 2004;25(12):1009–13.
Lundergan CF, Reiner JS, Ross AM. How long is too long? Association of time delay to successful reperfusion and ventricular function outcome in acute myocardial infarction: the case for thrombolytic therapy before planned angioplasty for acute myocardial infarction. Am Heart J. 2002;144(3)456–62.
McNamara RL, Wang Y, Herrin J, et al. Effect of door-to-balloon time on mortality in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2006;47(11)2180–6.
Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction; a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44(3):E1–E211.
De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction—Every minute of delay counts. Circulation. 2004;109(10):1223–5.
De Luca G, Suryapranata H, Zijlstra F, et al. Symptom-onset-to-balloon time and mortality in patients with acute myocardial infarction treated by primary angioplasty. J Am Coll Cardiol. 2003;42(6):991–7.
McNamara RL, Herrin J, Bradley EH, et al. Hospital improvement in time to reperfusion in patients with acute myocardial infarction, 1999 to 2002. J Am Coll Cardiol. 2006;47(1):45–51.
Nallamothu BK, Bates E, Herrin J, Wang YF, Bradley EH, Krumholz HM. Times to treatment in transfer patients undergoing primary percutaneous coronary intervention in the United States—National Registry of Myocardial Infarction (NRMI)-3/4 analysis. Circulation. 2005;111(6):761–7.
The Joint Commission. Specifications manual for national hospital quality measures. In: CMS, ed. April 2007.
Bradley EH, Nallamothu BK, Curtis JP, et al. Summary of evidence regarding hospital strategies to reduce door-to-balloon times for patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Critical Pathways in Cardiology. 2007;6(3):91–7.
Shojania K, McDonald K, Wachter R, Owens D. Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies. Overview and Methodology.: AHRQ Publication No. 04-0051-1. Rockville, MD, 2004.
Bauer MS. A review of quantitative studies of adherence to mental health clinical practice guidelines. Harv Rev Psychiatr. 2002;10(3):138–53.
Altman D. Practical Statistics for Medical Research. London England: Chapman and Hall; 1991.
Sanborn TA, Jacobs AK, Frederick PD, Every N, French WJ. Comparability of quality-of-care indicators for emergency coronary angioplasty in patients with acute myocardial infarction regardless of on-site cardiac surgery (report from the national registry of myocardial infarction). Am J Cardiol. 2004;93(11):1335–9.
Wharton TP, Grines LL, Turco MA, et al. Primary angioplasty in acute myocardial infarction at hospitals with no surgery on-site—(The PAMI-no SOS study) versus transfer to surgical centers for primary angioplasty. J Am Coll Cardiol. 2004;43(11):1943–50.
Brown SGA, Galloway DM. Effect of ambulance 12-lead ECG recording on times to hospital reperfusion in acute myocardial infarction. Med J Aust. 2000;172(2):81–4.
Henry TD, Unger BT, Sharkey SW, et al. Design of a standardized system for transfer of patients with ST-elevation myocardial infarction for percutaneous coronary intervention. Am Heart J. 2005;150(3)373–84.
Mehta RH, Montoye CK, Gallogly M, et al. Improving quality of care for acute myocardial infarction: the Guidelines Applied in Practice (GAP) Initiative. JAMA. 2002;287(10):1269–76.
Zarich SW, Sachdeva R, Fishman R, et al. Effectiveness of a multidisciplinary quality improvement initiative in reducing door-to-balloon times in primary angioplasty. J Interv Cardiol. 2004;17(4):191–5.
Kinsman L, Tori K, Endacott R, Sharp M. Guideline implementation fails to improve thrombolytic administration. Accid Emerg Nurs. 2007;15(1):27–33.
Wilmshurst P, Purchase A, Webb C, Jowett C, Quinn T. Improving door to needle times with nurse initiated thrombolysis. Heart. 2000;84(3):262–6.
Brown DC, Mogelson S, Harris R, Kemp D, Massey M. Percutaneous coronary interventions in a rural hospital without surgical backup: report of one year of experience. Clin Cardiol. 2006;29(8):337–40.
Wharton TP Jr., Grines LL, Turco MA, et al. Primary angioplasty in acute myocardial infarction at hospitals with no surgery on-site (the PAMI-No SOS study) versus transfer to surgical centers for primary angioplasty. J Am Coll Cardiol. 2004;43(11):1943–50.
Pelliccia F, Cartoni D, Verde M, Salvini P, Mercuro G, Tanzi P. Critical pathways in the emergency department improve treatment modalities for patients with ST-elevation myocardial infarction in a European hospital. Clin Cardiol. 2004;27(12):698–700.
Qasim A, Malpass K, O’Gorman DJ, Heber ME. Education and debate. Quality improvement report: safety and efficacy of nurse initiated thrombolysis in patients with acute myocardial infarction. BMJ. 2002;324(7349):1328–31.
Corfield A, Graham CA, Adams JN, Booth I, McGuffie AC. Emergency department thrombolysis improves door to needle times. Emerg Med J. 2004;21(6):676–80.
Kellett J. Decision support and the appropriate use of fibrinolysis in myocardial infarction. Eff Clin Pract. 2001;4(1):1–9.
Kelion AD, Banning AP, Shahi M, Bell JA. The effect of reduction of door-to-needle times on the administration of thrombolytic therapy for acute myocardial infarction. Postgrad Med J. 1998;74(875):533–6.
Thomas D, Cooper L, Cooper J, Taylor D, Robb A. Direct fast track admission to a coronary care unit. J R Coll Physicians Lond. 1997;31(2):188–91.
MacCallum AG, Stafford PJ, Jones C, Vincent R, Perez-Avila C, Chamberlain DA. Reduction in hospital time to thrombolytic therapy by audit of policy guidelines. Eur Heart J. 1990;11(Suppl F)48–52.
Chan WK, Lam KN, Lau FL, Tang HM. Starting thrombolytic therapy for patients with acute myocardial infarction in Accident and Emergency Department: from implementation to evaluation. Chin Med J (Engl). 1998;111(4):291–4.
Edhouse JA, Sakr M, Wardrope J, Morris FP. Thrombolysis in acute myocardial infarction: the safety and efficiency of treatment in the accident and emergency department. J Accid Emerg Med. 1999;16(5):325–30.
Hourigan CT, Mountain D, Langton PE, et al. Changing the site of delivery of thrombolytic treatment for acute myocardial infarction from the coronary care unit to the emergency department greatly reduces door to needle time. Heart. 2000;84(2)157–63.
Irwani I, Seet CM, Manning PG. Emergency physician versus cardiologist-initiated thrombolysis for acute myocardial infarction: a Singapore experience. Singapore Med J. 2004;45(7):313–7, Jul.
Kendall JM, McCabe SE. The use of audit to set up a thrombolysis programme in the accident and emergency department. J Accid Emerg Med. 1996;13(1):49–53.
Lane G, Cuddihy J, Wright P, Doherty D, McShane A. Efficacy of fibrinolysis in the emergency department for acute myocardial infarction. Ir J Med Sci. 2005;174(3):9–12.
McLean S, O’Reilly M, Doyle M, Rathaille M. Improving door-to-drug time and ST segment resolution in AMI by moving thrombolysis administration to the Emergency Department. Accid Emerg Nurs. 2004;12(1):2–9.
Heath SM, Bain RJ, Andrews A, Chida S, Kitchen SI, Walters MI. Nurse initiated thrombolysis in the accident and emergency department: safe, accurate, and faster than fast track. Emerg Med J. 2003;20(5):418–20.
Somauroo JD, McCarten P, Appleton B, Amadi A, Rodrigues E. Effectiveness of a ‘thrombolysis nurse’ in shortening delay to thrombolysis in acute myocardial infarction. J R Coll Physicians Lond. 1999;33(1):46–50.
Kuppuswamy VC, Webbe D, Gupta S. Meeting the NSF targets for door-to-needle time in acute myocardial infarction—The role of a bolus thrombolytic. Br J Cardiol. 2006;13(1):36–41.
Lloyd G, Roberts A, Bashir I, Mumby M, Kamalvand K, Cooke R. An audit of clinical nurse practitioner led thrombolysis to improve the treatment of acute myocardial infarction. J Public Health Med. 2000;22(4):462–5.
Jacoby J, Axelband J, Patterson J, Belletti D, Heller M. Cardiac cath lab activation by the emergency physician without prior consultation decreases door-to-balloon time. J Invasive Cardiol. 2005;17(3):154–5.
Thatcher JL,Gilseth TA, Adlis S. Improved efficiency in acute myocardial infarction care through commitment to emergency department-initiated primary PCI. J Invasive Cardiol. 2003;15(12):693–8.
Chongtham DS, Vivekananda SG, Grover A, et al. Utilization of telefax system for early detection, interpretation and management of acute ST-elevation myocardial infarction: an initial experience from rural Punjab telecardiology rapid access project. Indian Heart J. 2006;58(6):409–16.
Caputo RP, Ho KK, Stoler RC, et al. Effect of continuous quality improvement analysis on the delivery of primary percutaneous transluminal coronary angioplasty for acute myocardial infarction. Am J Cardiol. 1997;79(9):1159–64.
Caputo RP, Kosinski R, Walford G, et al. Effect of continuous quality improvement analysis on the delivery of primary percutaneous revascularization for acute myocardial infarction: a community hospital experience. Catheter Cardiovasc Interv. 2005;64(4):428–33. discussion 34–5.
Bonetti PO, Waeckerlin A, Schuepfer G, Frutiger A. Improving time-sensitive processes in the intensive care unit: the example of ‘door-to-needle time’ in acute myocardial infarction. Int J Qual Health Care. 2000;12(4):311–7.
Saturno PJ, Felices F, Segura J, Vera A, Rodriguez JJ. Reducing time delay in the thrombolysis of myocardial infarction: an internal quality improvement project. ARIAM Project Group. Analisis del Retraso en Infarto Agudo de Miocardio. Am J Med Qual. 2000;15(3):85–93.
Gilutz H, Battler A, Rabinowitz I, Snir Y, Porath A, Rabinowitz G. The “door-to-needle blitz” in acute myocardial infarction: the impact of a CQI project. Jt Comm J Qual Improv. 1998;24(6):323–33.
Bharat V, Tripathy S, Guha AK, Mitra A. Fast track thrombolysis in acute myocardial infarction: a quality improvement project. Indian Heart J. 1998;50(2):167–71.
Guidry UA, Paul SD, Vega J, et al. Impact of a simple inexpensive quality assurance effort on physician’s choice of thrombolytic agents and door-to-needle time: implication for costs of management. J Thromb Thrombolysis. 1998;5(2):151–7.
Porter G, Doughty R, Gamble G, Sharpe N. Thrombolysis in acute myocardial infarction: reducing in hospital treatment delay. N Z Med J. 1995;108(1002):253–4.
Owen A, Husk J. An audit of acute myocardial infarction in a district general hospital: results and recommendations. J Clin Excell. 2000;2(2):111–8.
Maxey C. A case map reduces time to administration of thrombolytic therapy in patients experiencing an acute myocardial infarction. Nurs Case Manag. 1997;2(5):229–37.
Cannon CP, Johnson EB, Cermignani M, Scirica BM, Sagarin MJ, Walls RM. Emergency department thrombolysis critical pathway reduces door-to-drug times in acute myocardial infarction. Clin Cardiol. 1999;22(1):17–20.
Bestul MB, McCollum M, Stringer KA, Burchenal J. Impact of a critical pathway on acute myocardial infarction quality indicators. Pharmacotherapy. 2004;24(2):173–8.
Senior J, Patel N. Reducing thrombolytic therapy time delays in the emergency department. J Qual Clin Pract. 1998;18(2):99–107.
Eccles M, Grimshaw J, Walker A, Johnston M, Pitts N. Changing the behavior of healthcare professionals: the use of theory in promoting the uptake of research findings. J Clin Epidemiol. 2005;58:107–12.
ICEBeRG. Designing theoretically informed implementation interventions. Implementation Science. 2006;1(1):4.
Acknowledgment
This work was supported by the Office of Research and Development, Health Services R&D Service, Department of Veterans Affairs, project number IHD 04–0001. The views expressed are those of the authors and do not reflect the views of the Department of Veterans Affairs.
Conflict of Interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary materials
Below is the link to the electronic supplementary materials.
Rights and permissions
About this article
Cite this article
McDermott, K.A., Helfrich, C.D., Sales, A.E. et al. A Review of Interventions and System Changes to Improve Time to Reperfusion for ST-Segment Elevation Myocardial Infarction. J GEN INTERN MED 23, 1246–1256 (2008). https://doi.org/10.1007/s11606-008-0563-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-008-0563-7