
Abstract
Background
Earlier work demonstrated that ACGME duty hour reform did not adversely affect mortality, with slight improvement noted among specific subgroups.
Objective
To determine whether resident duty hour reform differentially affected the mortality risk of high severity patients or patients who experienced post-operative complications (failure-to-rescue).
Design
Observational study using interrupted time series analysis with data from July 1, 2000 - June 30, 2005. Fixed effects logistic regression was used to examine the change in the odds of mortality or failure-to-rescue (FTR) in more versus less teaching-intensive hospitals before and after duty hour reform.
Participants
All unique Medicare patients (n = 8,529,595) admitted to short-term acute care non-federal hospitals and all unique VA patients (n = 318,636 patients) with principal diagnoses of acute myocardial infarction, congestive heart failure, gastrointestinal bleeding, stroke or a DRG classification of general, orthopedic or vascular surgery.
Measurements and Main Results
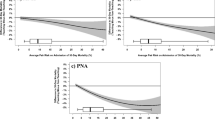
We measured mortality within 30 days of hospital admission and FTR, measured by death among patients who experienced a surgical complication. The odds of mortality and FTR generally changed at similar rates for higher and lower risk patients in more vs. less teaching intensive hospitals. For example, comparing the mortality risk for the 10% of Medicare patients with highest risk to the other 90% of patients in post-reform year 1 for combined medical an OR of 1.01 [95% CI 0.90, 1.13], for combined surgical an OR of 0.91 [95% CI 0.80, 1.04], and for FTR an OR of 0.94 [95% CI 0.80, 1.09]. Findings were similar in year 2 for both Medicare and VA. The two exceptions were a relative increase in mortality for the highest risk medical (OR 1.63 [95% CI 1.08, 2.46]) and a relative decrease in the high risk surgical patients within VA in post-reform year 1 (OR 0.52 [95% CI 0.29, 0.96]).
Conclusions
ACGME duty hour reform was not associated with any consistent improvements or worsening in mortality or failure-to-rescue rates for high risk medical or surgical patients.

Similar content being viewed by others


References
Volpp KG, Rosen AK, Rosenbaum PR, et al. Mortality among hospitalized Medicare beneficiaries in the first two years following ACGME resident duty hour reform. JAMA. 2007;298:975–83.
Volpp KG, Rosen AK, Rosenbaum PR, et al. Mortality among patients in VA hospitals in the first two years following ACGME resident duty hour reform. JAMA. 2007;298:984–92.
Shetty KD, Bhattacharya J. Changes in hospital mortality associated with residency work-hour regulations. Ann Intern Med. 2007;147(2):73–80.
Laine C, Goldman L, Soukup JR, Hayes JG. The impact of a regulation restricting medical house staff working hours on the quality of patient care. JAMA. 1993;269(3):374–8.
Drazen JM. Awake and informed. N Engl J Med. 2004;351(18):884.
Mukherjee S. A precarious exchange. N Engl J Med. 2004;351(18):1822–4.
Ofri D. Residency regulations–resisting our reflexes. N Engl J Med. 2004;351(18):1824–6.
Silber JH, Williams SV, Krakauer H, Schwartz JS. Hospital and patient characteristics associated with death after surgery: A study of adverse occurrence and failure-to-rescue. Med Care. 1992;30(7):615–29.
Silber JH, Rosenbaum PR, Ross RN. Comparing the contributions of groups of predictors: Which outcomes vary with hospital rather than patient characteristics? J Am Stat Assoc. 1995;90(429):7–18.
Silber JH, Rosenbaum PR, Schwartz JS, Ross RN, Williams SV. Evaluation of the complication rate as a measure of quality of care in coronary artery bypass graft surgery. JAMA. 1995;274(4):317–23.
Silber JH, Romano PS, Rosen AK, Wang Y, Even-Shoshan O, Volpp KG. Failure-to-rescue: Comparing definitions to measure quality of care. Med Care. 2007; 45(10):918–25.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27.
Glance LG, Dick AW, Osler TM, Mukamel DB. Does date stamping ICD-9-CM codes increase the value of clinical information in administrative data? Health Serv Res. 2006;41(1):231–51.
Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–9.
Southern DA, Quan H, Ghali WA. Comparison of the Elixhauser and Charlson/Deyo methods of comorbidity measurement in administrative data. Med Care. 2004;42(4):355–60.
Stukenborg GJ, Wagner DP, Connors AF Jr. Comparison of the performance of two comorbidity measures, with and without information from prior hospitalizations. Med Care. 2001;39(7):727–39.
Deyo R, Cherkin D, Ciol M. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–619.
Silber J, Rosenbaum P, Schwartz J, Ross R. Comparing the contributions of groups of predictors: which outcomes vary with hospital rather than patient characteristics? J Am Stat Assoc. 1995;90(429):7–18.
Haberman SJ. Generalized residuals for log-linear models. Proceedings of the 9th International Biometric Conference. 1st ed. Boston: The Biometric Society; 1976:104–23.
Haberman SJ. The analysis of frequency data. Chicago: The University of Chicago Press; 1974.
Ayanian JZ, Weissman JS. Teaching hospitals and quality of care: a review of the literature. Milbank Q. 2002;80(3):569–93.
Keeler EB, Rubenstein LV, Kahn KL, et al. Hospital characteristics and quality of care. JAMA. 1992;268(13):1709–14.
Allison JJ, Kiefe CI, Weissman NW, et al. Relationship of hospital teaching status with quality of care and mortality for Medicare patients with acute MI. JAMA. 2000;284(10):1256–62.
Taylor DH, Whellan DJ, Sloan FA. Effects of admission to a teaching hospital on the cost and quality of care for medicare beneficiaries. N Engl J Med. 1999;340(4):293–9.
Cox DR. Note on grouping. J Am Stat Assoc. 1957;52(280):543–7.
Cochran WG. The effectiveness of adjustment by subclassification in removing bias in observational studies. Biometrics. 1968;24(2):295–313.
Campbell DT, Stanley JC. Experimental and quasi-experimental designs for research. Dallas: Houghton Mifflin Company; 1963.
Shadish WR, Cook TD, Campbell DT. Experimental and quasi-experimental designs for generalized causal inference. Boston: Houghton-Mifflin; 2002.
Rosenbaum PR. Stability in the absence of treatment. J Am Stat Assoc. 2001;96:210–9.
Lawthers AG, McCarthy EP, Davis RB, Peterson LE, Palmer RH, Iezzoni LI. Identification of in-hospital complications from claims data. Is it valid? Med Care. 2000;38:785–95.
McCarthy EP, Iezzoni LI, Davis RB, et al. Does clinical evidence support ICD-9-CM diagnosis coding of complications? Med Care. 2000;38:868–76.
Weingart SN, Iezzoni LI, Davis RB, et al. Use of administrative data to find substandard care. Validation of the complications screening program. Med Care. 2000;38:796–806.
California Office of Statewide Health Planning and Development. (OSHPD). Second report of the California Hospitals Outcomes Project. Acute myocardial infarction. 1996 May.
Institute of Medicine. Optimizing graduate medical trainee (resident) hours and work schedules to improve patient safety. 2007.
Myers JS, Bellini LM, Morris JB, et al. Internal medicine and general surgery residents’ attitudes about the ACGME duty hours regulations: A multicenter study. Acad Med. 2006;81(12):1052–8.
Jagsi R, Shapiro J, Weissman JS, Dorer DJ, Weinstein DF. The educational impact of ACGME limits on resident and fellow duty hours: A pre–post survey study. Acad Med. 2006;81:1059–68.
Rosen AK, Loveland SA, Romano PS, et al. Effects of resident duty hour reform on patient safety among hospitalized VA and medicare patients. Med Care. 2009. in press.
Silber J, Rosenbaum PR, Rosen AK, et al. Prolonged hospital stays and the resident duty hour rules of 2003. Med Care. 2009. in press.
Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns’ work hours on serious medical errors in intensive care units. N Engl J Med. 2004;351(18):1838–48.
Lockley SW, Cronin JW, Evans EE, et al. Effect of reducing interns’ weekly work hours on sleep and attentional failures. N Engl J Med. 2004;351(18):1829–37.
Acknowledgements
This work was supported primarily by grant VA HSR&D IIR 04.202.1 and NHLBI R01 HL082637, with additional support from National Science Foundation grant SES-0646002. The sponsors/funders have had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript. Dr. Volpp had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. We also thank Yun Teng for her assistance with the analyses. Everyone who contributed significantly to this work has been acknowledged.
Conflict of Interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Volpp, K.G., Rosen, A.K., Rosenbaum, P.R. et al. Did Duty Hour Reform Lead to Better Outcomes Among the Highest Risk Patients?. J GEN INTERN MED 24, 1149–1155 (2009). https://doi.org/10.1007/s11606-009-1011-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-009-1011-z