
Abstract
BACKGROUND
Multiple factors, including patient characteristics, competing demands, and clinic type, impact delivery of depression treatment in primary care.
OBJECTIVE
Assess whether depression severity and HIV serostatus have a differential effect on time to depression treatment among depressed patients receiving primary care at Infectious Disease or General Medicine clinics.
DESIGN
Multicenter prospective cohort, (Veterans Aging Cohort Study), comparing HIV-infected to uninfected patients.
PARTICIPANTS AND MEASURES
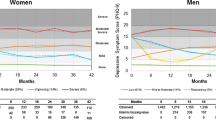
The total cohort consisted of 3,239 HIV-infected and 3,227 uninfected patients. Study inclusion criteria were untreated depressive symptoms, based on a Patient Health Questionnaire (PHQ-9) score of greater than 9, and no antidepressants or mental health visits in the 90 days prior to PHQ-9 assessment. Treatment was defined as antidepressant receipt or mental health visit within 90 days following PHQ-9 assessment. Depression severity based on PHQ-9 scores was defined as mild-moderate (greater than 9 to 19) and severe (20 or greater). Kaplan-Meier curves were used to estimate time to treatment by depression severity and HIV serostatus. Cox proportional hazards methods adjusted for covariates were used.
KEY RESULTS
Overall, 718 (11%) of the cohort met inclusion criteria, 258 (36%) of whom received treatment. Median time to treatment was 7 days [95% confidence interval (CI) = 4, 13] and was shortest for severely depressed HIV-infected patients (0.5 days; 95% CI = 0.5, 6, p = 0.04). Compared to mildly-moderately depressed uninfected patients, severely depressed HIV-infected patients were significantly more likely to receive treatment [adjusted hazard ratio (HR) 1.67, 95% CI = 1.07, 2.60), whereas mildly-moderately depressed HIV-infected patients (adjusted HR 1.10, 95% CI = 0.79, 1.52) and severely depressed uninfected patients (adjusted HR 0.93, 95% CI = 0.60, 1.44) were not.
CONCLUSIONS
In this large cohort, time to primary care treatment of depression was shortest among severely depressed HIV-infected patients. Regardless of HIV serostatus, if depression was not treated on the assessment day, then it was unlikely to be treated within a 90-day period, leading to the majority of depression being untreated.

Similar content being viewed by others
References
Katon WJ. Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biol Psychiatry. 2003;54:216–26.
Sherbourne CD, Hays RD, Fleishman JA, et al. Impact of psychiatric conditions on health-related quality of life in persons with HIV infection. Am J Psychiatry. 2000;157:248–54.
Wulsin LR, Vaillant GE, Wells VE. A systematic review of the mortality of depression. Psychosom Med. 1999;61:6–17.
Treisman G, Angelino A. Interrelation between psychiatric disorders and the prevention and treatment of HIV infection. Clin Infect Dis. 2007;45(Suppl 4):S313–7.
Sternhell PS, Corr MJ. Psychiatric morbidity and adherence to antiretroviral medication in patients with HIV/AIDS. Aust NZ J Psychiatry. 2002;36:528–33.
Paterson DL, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133:21–30.
Leserman J. HIV disease progression: depression, stress, and possible mechanisms. Biol Psychiatry. 2003;54:295–306.
Bing EG, Burnam MA, Longshore D, et al. Psychiatric disorders and drug use among human immunodeficiency virus-infected adults in the United States. Arch Gen Psychiatry. 2001;58:721–8.
Himelhoch S, Medoff DR. Efficacy of antidepressant medication among HIV-positive individuals with depression: a systematic review and meta-analysis. AIDS Patient Care ST. 2005;19:813–22.
Himelhoch S, Medoff DR, Oyeniyi G. Efficacy of group psychotherapy to reduce depressive symptoms among HIV-infected individuals: a systematic review and meta-analysis. AIDS Patient Care ST. 2007;21:732–9.
Goldman LS, Nielsen NH, Champion HC. Awareness, diagnosis, and treatment of depression. J Gen Intern Med. 1999;14:569–80.
Vitiello B, Burnam MA, Bing EG, Beckman R, Shapiro MF. Use of psychotropic medications among HIV-infected patients in the United States. Am J Psychiatry. 2003;160:547–54.
Colibazzi T, Hsu TT, Gilmer WS. Human immunodeficiency virus and depression in primary care: a clinical review. Prim Care Companion J Clin Psychiat. 2006;8:201–11.
Nutting PA, Rost K, Smith J, Werner JJ, Elliot C. Competing demands from physical problems: effect on initiating and completing depression care over 6 months. Arch Fam Med. 2000;9:1059–64.
Sueoka K, Goulet JL, Fiellin DA, et al. Depression symptoms and treatment among HIV infected and uninfected veterans. AIDS Behav. Epub 2008 Jul 22.
Ani C, Bazargan M, Hindman D, Bell D, Rodriguez M, Baker RS. Comorbid chronic illness and the diagnosis and treatment of depression in safety net primary care settings. J Am Board Fam Med. 2009;22:123–35.
Justice AC, Dombrowski E, Conigliaro J, et al. Veterans Aging Cohort Study (VACS): Overview and description. Med Care. 2006;44:S13–24.
Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Intern Med. 1998;158:1789–95.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Fultz SL, Goulet JL, Weissman S, et al. Differences between infectious diseases-certified physicians and general medicine-certified physicians in the level of comfort with providing primary care to patients. Clin Infect Dis. 2005;41:738–43.
Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282:1737–44.
Rollman BL, Weinreb L, Korsen N, Schulberg HC. Implementation of guideline-based care for depression in primary care. Adm Policy Ment Health. 2006;33:43–53.
Gilbody S, Richards D, Brealey S, Hewitt C. Screening for depression in medical settings with the Patient Health Questionnaire (PHQ): a diagnostic meta-analysis. J Gen Intern Med. 2007;22:1596–602.
U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. Clinical Practice Guideline, Number 5. Depression guideline panel: Depression in primary care: Volume 2. Treatment of major depression. 1993; AHCPR Publication No. 93-0551: http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=hsarchive&part=A15593. Accessed February 15, 2010.
Gaynes BN, Rush AJ, Trivedi MH, Wisniewski SR, Spencer D, Fava M. The STAR*D study: treating depression in the real world. Cleve Clin J Med. 2008;75:57–66.
Block SD. Assessing and managing depression in the terminally ill patient. ACP-ASIM End-of-Life Care Consensus Panel. American College of Physicians—American Society of Internal Medicine. Ann Intern Med. 2000;132:209–18.
Linden M, Lecrubier Y, Bellantuono C, Benkert O, Kisely S, Simon G. The prescribing of psychotropic drugs by primary care physicians: an international collaborative study. J Clin Psychopharmacol. 1999;19:132–40.
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC, American Psychiatric Association, 2000.
Katon WJ. The comorbidity of diabetes mellitus and depression. Am J Med. 2008;121:S8–15.
Lippi G, Montagnana M, Favaloro EJ, Franchini M. Mental depression and cardiovascular disease: a multifaceted, bidirectional association. Semin Thromb Hemost. 2009;35:325–36.
Borowsky SJ, Rubenstein LV, Meredith LS, Camp P, Jackson-Triche M, Wells KB. Who is at risk of nondetection of mental health problems in primary care? J Gen Intern Med. 2000;15:381–8.
Das AK, Olfson M, McCurtis HL, Weissman MM. Depression in African Americans: breaking barriers to detection and treatment. J Fam Pract. 2006;55:30–9.
Nelligan JA, Loftis JM, Matthews AM, Zucker BL, Linke AM, Hauser P. Depression comorbidity and antidepressant use in veterans with chronic hepatitis C: results from a retrospective chart review. J Clin Psychiatry. 2008;69:810–6.
Hance M, Carney RM, Freedland KE, Skala J. Depression in patients with coronary heart disease. A 12-month follow-up. Gen Hosp Psych. 1996;18:61–5.
Klinkman MS. Competing demands in psychosocial care. A model for the identification and treatment of depressive disorders in primary care. Gen Hosp Psych. 1997;19:98–111.
Acknowledgements
This work was funded by National Institute on Alcohol and Alcohol Abuse (U01 AA 13566 and U10 AA 13566), National Institute of Aging (K23 AG00826), Robert Wood Johnson Generalist Faculty Scholar Award, an Inter-agency Agreement between NIA, National Institute of Mental Health, and VA HSR&D Research Enhancement Award Program (REAP) PRIME Project (REA 08-266).
Conflict of Interest
None disclosed.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
The views expressed here are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
Funding
National Institute on Alcohol and Alcohol Abuse (U01 AA 13566 and U10 AA 13566), National Institute of Aging (K23 AG00826), Robert Wood Johnson Generalist Faculty Scholar Award, an Inter-agency Agreement between NIA, National Institute of Mental Health, and VA HSR&D Research Enhancement Award Program (REAP) PRIME Project (REA 08-266).
Rights and permissions
About this article
Cite this article
Hooshyar, D., Goulet, J., Chwastiak, L. et al. Time to Depression Treatment in Primary Care Among HIV-infected and Uninfected Veterans. J GEN INTERN MED 25, 656–662 (2010). https://doi.org/10.1007/s11606-010-1323-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-010-1323-z