
Abstract
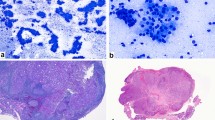
Objectives Immunohistochemistry (IHC) can be helpful in the diagnosis of minor salivary gland neoplasms including those that have been incisionally biopsied or fragmented during surgery that do not contain key diagnostic features on hematoxylin and eosin sections. IHC has been used as an adjunct to distinguish among many salivary gland neoplasms using both qualitative and quantitative methods. The objective of this study was to determine whether a distinctive immunoreactivity staining pattern to GFAP can be consistently observed among three selected minor salivary gland neoplasms and thus serve as a diagnostic adjunctive procedure. Study Design Glial fibrillary acidic protein (GFAP) reactivity was examined among 78 minor salivary gland neoplasms: 27 canalicular adenomas (CAA), 21 pleomorphic adenomas (PA) and 30 polymorphous low grade adenocarcinomas (PLGA). Each case was evaluated by two oral and maxillofacial pathologists (OMP) blinded to the diagnosis. Consensus was reached on the pattern of GFAP reactivity among the neoplastic cells and on the similarities and differences among the cases. Results Ninety-six percent (96%) of CAAs demonstrated a distinctive linear immunoreactive pattern among cells in proximity to connective tissue interface. All (100%) PAs demonstrated diffuse immunopositivity within tumor cells. All (100%) PLGAs showed little or no intralesional reactivity and no peripheral linear immunoreactivity. Additional challenge cases were examined by outside OMPs to demonstrate the utility of these findings. Conclusions This study demonstrates that the pattern of GFAP immunoreactivity may be an adjunct to diagnosis among PA, CAA and PLGA. The pattern of distinctly linear GFAP immunoreactivity at the tumor/connective tissue interface in CAA has not been reported previously. This distinctive feature may permit the pathologist to differentiate among CAA, PA and PLGA when an incisional biopsy and/or fragmentation cause key diagnostic features to be absent. Because each of these neoplasms requires a different treatment approach, this can be of major significance.






Similar content being viewed by others

Bibliography
Gnepp DR, el-Mofty S. Polymorphous low grade adenocarcinoma: glial fibrillary acidic protein staining in the differential diagnosis with cellular mixed tumors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;83:691–5.
Castle JT, Thompson LD, Frommett RA, Wenig BM, Kessler HP. Polymorphous low-grade adenocarcinoma: a clinicopathologic study of 164 cases. Cancer 1999;86:207–19.
Curran AE, White DK, Damm DD, Murrah VA. Polymorphous low-grade adenocarcinoma versus pleomorphic adenoma of minor salivary glands: resolution of a diagnostic dilemma by immunohistochemical analysis with glial fibrillary acidic protein. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:194–9.
Gould VE, Koukoulis GK, Jansson DS, Franke WW, Moll R. Co-expression patterns of vimentin and glial fibrillary acidic protein in normal, hyperplastic and neoplastic breast. Am J Surg Pathol 1990;137:1143–55.
Liuder TM, Kros JM, Sillevis Smitt PA, van den Bent MJ, Vecht CJ. Glial fibrillary acidic protein and its fragments discriminate astrocytoma from oligodenroglioma. Electrophoresis 1999;20:1087–91.
Murphy KG, Hatton JD. Role of glial fibrillary acidic protein expression in the biology of human glioblastoma U-373MG cells. J Neurosurg 1998;89:997–1006.
Zarbo RJ, Prasad AR, Regezi JA, Gown AM, Savera AT. Salivary gland basal cell and canalicular adenomas: immunohistochemical demonstration of myoepithelial cell participation and morphogenetic considerations. Arch Pathol Lab Med 2000;124:401–5.
Sharkey TE. Systematic evaluation of WHO classification of salivary gland tumors: a clinicopathologic study of 366 cases. Am J Clin Pathol 1977;67:272–8.
Ellis GL, Auclair PL. Tumors of the salivary glands. Third Series. Washington DC: Armed Forces Institute of Pathology; 1996. 100.
Nishimura T, Furukawa M, Kawahara E, Miwa A. Differential diagnosis of pleomorphic adenoma by immunohistochemical means. J Layngol Otol 1991;105:1057–60.
Rousseau A, Mock D, Dover DG, Jordan RC. Multiple canalicular adenomas: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:346–50.
Viale G, Gambacorta M, Coggi G, Dell’Orto P, Milani M, Doglioni C. Glial fibrillary acidic protein immunoreactivity in normal and diseased human breast. Virchows Arch A Pathol Anat Histopathol 1991;418:339–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Curran, A.E., Allen, C.M., Beck, F.M. et al. Distinctive Pattern of Glial Fibrillary Acidic Protein Immunoreactivity Useful in Distinguishing Fragmented Pleomorphic Adenoma, Canalicular Adenoma and Polymorphous Low Grade Adenocarcinoma of Minor Salivary Glands. Head and Neck Pathol 1, 27–32 (2007). https://doi.org/10.1007/s12105-007-0003-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12105-007-0003-8