
Abstract
The research team recruited eight Chinese American (seven females, one male) lay health workers (LHWs). They received 12 h of training about colorectal cancer (CRC), its screening, and basic health education techniques. Each LHW were asked to recruit ten participants and conduct two educational sessions. Of the 81 participants recruited, 73 had not received colorectal cancer screening. Their mean age was 63.0 years, and 72.6% were women. Knowledge of colorectal cancer, its causes, and its screening increased significantly. Receipt of first colorectal cancer screening test increased from 0.0% at baseline to 55.7% for fecal occult blood tests, 7.1% for sigmoidoscopy, and 7.1% for colonoscopy. LHW outreach is feasible and may be effective in promoting CRC screening among Chinese Americans.
Similar content being viewed by others


Introduction
Chinese Americans constitute the largest Asian American ethnic group with a population of about 2.8 million [1]. Nearly 70% are foreign-born, with half speaking English less than “very well” [1]. Colorectal cancer is the second most common cancer among Chinese Americans [2], who have incidence rates similar to those of non-Hispanic whites [2]. Asian immigrants have a higher risk of colorectal cancer compared to Asians in Asia, with most of the increase occurring in the first generation [3].
Five-year survival rates for colorectal cancer is greater than 90% if diagnosed at a local stage [4]. Unfortunately, only 40% of cases were diagnosed at a local stage among both Chinese and non-Hispanic whites [2]. Colorectal cancer screening reduces mortality [5–7] and is cost effective [8, 9]. The US Preventive Services Task Force (USPSTF) recommends screening with fecal occult blood test (FOBT) annually, sigmoidoscopy every 5 years, FOBT annually and sigmoidoscopy every 5 years, or colonoscopy every 10 years for average-risk persons’ aged 50 to 75 [10]. There is no reliable national data on colorectal cancer screening among Chinese Americans, but in the 2001 California Health Interview Survey, they had lower rates of ever having been screened by FOBT, sigmoidoscopy/colonoscopy, or either (40%, 43%, and 59%, respectively) than non-Hispanic whites (58%, 57%, and 75%) [11]. After controlling for socioeconomic status and access to care, Chinese Americans were significantly less likely than non-Hispanic whites to be screened [12]. There is only one published study of a health education intervention to increase CRC screening among Chinese Americans [13].
Health promotion programs have employed community health educators, often in communities with poor access to resources and information [14–17]. The World Health Organization defined “lay health workers” (LHWs) as those who live in a community, are selected by and accountable to it, and work after receiving a short, defined training [17, 18]. Despite their widespread use, there are few rigorous studies of their effectiveness. A review of the US literature reported that LHWs typically provided education and were effective in increasing access to care such as screening services [17]. A recent review in Hispanic communities reported a need for more evidence of effectiveness [19]. Among African Americans and Latinas, LHWs increased mammography but not Pap testing rates [20–22]. This research group has shown that, among Vietnamese American women, LHWs increased cervical cancer screening in a randomized controlled trial (RCT) [23] and breast cancer screening in a RCT [24]. There is only one published study on the use of LHWs among Chinese Americans [25] and one on LHW outreach for CRC screening in any ethnic group, although there have been several on the use of patient navigators [26–31].
This article reports the results of a pilot community-based participatory research (CBPR) project to implement a LHW outreach program to address colorectal cancer screening among immigrant Chinese Americans in San Francisco, CA. The goals of the pilot were to assess the feasibility of implementing LHW outreach and to evaluate its effectiveness in increasing the rate of colorectal cancer screening in that population.
Methods
Phase 1: Planning
Identification of Research Question, Intervention, and Collaborations
In 2000, the National Cancer Institute’s Center to Reduce Cancer Health Disparities funded the Asian American Network for Cancer Awareness, Research, and Training (AANCART) to develop capacity for cancer control among Asian Americans. San Francisco was an AANCART site with two partners, the Vietnamese Community Health Promotion Project (VCHPP) and the Chinese Community Health Care Association (CCHCA). In 2004, CCHCA and its network of community partners, the Chinese Council, chose colorectal cancer as a health priority. VCHPP presented the concept of using LHWs to promote colorectal cancer screening among Chinese Americans in San Francisco to the Council, which evaluated the concept and agreed that it was culturally appropriate and desirable and had the potential to build outreach and research capacity. The target population was identified as limited English proficient Chinese Americans. The Council appointed one of its members, NICOS Chinese Health Coalition, to work with VCHPP to submit a grant application. A third partner, the Community Health Works program at San Francisco City College and San Francisco State University (SFSU), was involved since it has experience in training community health educators and provided a potential career development option for successful lay health workers. The three partners successfully submitted a research grant application to the SFSU-UCSF Minority-Serving Institution/Cancer Center Partnership. The scope of work and funding were evenly split among the partners. The Institutional Review Boards at SFSU and UCSF approved the research protocols.
Focus Groups
The research team conducted two focus groups (one male, one female) among Chinese Americans age 50 and older in Cantonese. A gender concordant bilingual member (LCF, CW) of the research team led each group. Respondents gave their opinions about colorectal cancer, its prevention, colorectal cancer screening, and the concept of learning about such screening from peers. The results of the focus groups informed the development of the LHW materials and training.
Educational Materials
Due to time constraint, a bilingual English–Vietnamese colorectal cancer brochure, developed in the English language, translated to Vietnamese, and tested with focus groups as well as in a study, was used. A bilingual team member translated the brochure into traditional Chinese characters. The translation was reviewed by two other bilingual staff and revised. The text along with findings from the focus groups was then incorporated into a LHW manual and a bilingual flipchart. The flipchart was created with appropriate cultural images and pictures of Chinese Americans. It included information about colorectal cancer, its symptoms, its risk factors, and its prevention. The flipchart focused on targeted information such as the high rates of colorectal cancer among the Chinese and included a section of responses to frequently asked questions and beliefs, such as the role of diet in prevention, the need of screening when asymptomatic, and cultural factors such as traditional (herbal) medicine and concepts such as fate. The flipchart emphasized that any of the colorectal cancer screening tests recommended by the USPSTF could be used to screen for colorectal cancer. However, during the developmental process, it was clear that there were access problems preventing or delaying timely endoscopic screening in San Francisco. Thus, the flipchart focused on FOBT receipt as an easily accessible test. The flipchart was reviewed by bilingual community members, health care providers, and researchers at a meeting of the Chinese Council and revised prior to printing.
Phase 2: Lay Health Worker Recruitment and Training
LHW Recruitment
Recruitment for LHWs was done primarily through Chinese language newspapers and fliers distributed to community organizations. Of the 111 inquiries, 40 reported finding out through newspaper, 44 from flyers, and 23 from emails and/or word of mouth. Those recruited through newspapers expressed the most interest. Among the inquiries with significant interest, 28 were women and nine were men. Seven women and one man were selected based on their level of interest, communication ability, commitment to the project, and size of their social network. Each LHW could be expected to spend about 50–60 h in recruitment, training, outreach, and research activities and thus was paid $1,000 for their participation in this research project. This amount was chosen based on a CBPR consideration that participants with skills from the community should be adequately compensated for their time on a research project.
LHW Training
The training program was developed based on prior training activities done by the SFSU Community Health Works team and incorporating lessons learned by the UCSF team in previous LHW projects. A training manual was also developed in English and translated to traditional written Chinese. The LHWs were trained in two 6-hour training sessions over 2 days. The first day focused on providing an overview of the project, understanding the scope of practice, introduction to basic colorectal cancer information, and basic health and presentation skills, while the second day focused primarily on the logistics to recruitment and outreach, and role play. LHWs were taught how each of the screening tests was done and the preparation needed. They watched a video on how to perform an FOBT. Each LHW completed three FOBT cards at home and then returned them to a physician. On the second training day, the LHWs visited a gastroenterologist’s office to become familiar with the equipment and setting for sigmoidoscopy and colonoscopy. Surveys administered before and after the training evaluated the LHWs’ understanding of the materials presented in the training.
Phase 3: Intervention Implementation
Participant Recruitment and Retention
Each LHW was expected to recruit ten participants, and the eight LHWs recruited 82 participants. Eligibility criteria for participants in the intervention included age 50 and older, self-identification as Chinese or Chinese American, resident of San Francisco, Chinese or English speaking, and never having received colorectal cancer screening. Recruitment was easy for some LHWs and difficult for others. Those with extensive social networks had little trouble. Out of 355 people approached, 203 were interested. Among those not interested, 18 did not have time, 12 were suspicious or afraid, 15 had other reasons, and the others gave no reason. There were 121 ineligibles (seven aged <50 and 114 already had screening). Of the 82 participants, one woman dropped out while filling out the pre-intervention survey. The other 81 completed the first LHW session. One participant died between the first and second session due to an unrelated cause. Of the remaining 80 participants, 77 completed both small group sessions.
LHW Intervention
Each participant attended two LHW outreach sessions. The first session focused on knowledge about colorectal cancer, its screening, and recommendations as LHWs presented using the flipchart. The eight LHWs held a total of 21 first sessions with two to eight participants each. The second session, occurring approximately 6–8 weeks later, was to reinforce knowledge, identify problems, and assist in problem solving. There were 18 second sessions. LHWs also made follow-up telephone calls after each session. The purpose of the calls were to (1) remind the participants of the next event (either the second outreach session or the post-intervention survey; (2) assess if the participant had obtained screening yet, and if not, why not; and (3) assist the participant in obtaining screening, either by answering questions or providing encouragement.
Survey Instrument Development and Administration
The team developed a survey instrument using item pools from other published studies and incorporating findings from the focus groups. The survey was reviewed in English by all members of the research team and then translated into traditional written Chinese. Two bilingual members of the team reviewed the survey for linguistic and conceptual accuracy. The post-intervention survey repeated knowledge, attitudes, and outcomes measures as well as questions about the program and the participants’ dissemination of the information to others. A member of the research team administered the pre-intervention survey at the first LHW session for each participant. The post-intervention survey was administered in person (66 participants) or by telephone (11 participants) by a member of the research team approximately 5–6 months after the pre-intervention survey.
Measurements
The primary outcome was self-reported receipt of first FOBT. Secondary outcomes included first receipt of sigmoidoscopy and first receipt of colonoscopy. Participants were also asked if they thought about obtaining an FOBT, a sigmoidoscopy, or a colonoscopy if he/she never had one and whether the participant planned on obtaining an FOBT or a sigmoidoscopy/colonoscopy in the next 12 months. Other variables collected included sociodemographics (age, sex, years in the USA, English fluency, educational attainment, marital status, employment, household income), self-reported health, health care access (usual place for care, health insurance), use of Chinese herbalists, and family history of colorectal cancer. Participants were also asked if they had ever heard of colorectal cancer, colon polyp, FOBT, sigmoidoscopy, or colonoscopy, if they knew the factors associated with colorectal cancer, ways to prevent colorectal cancer, and attitudes about colorectal cancer and its screening.
Analyses
Descriptive statistics including means, percents, and 95% confidence intervals were computed for each variable. Despite the screening process, six participants stated on the pre-intervention survey that they already had an FOBT, one already had sigmoidoscopy, and one both tests prior to participation, leaving 73 participants in the final analyses. To examine the pairwise differences between the pre- and the post-intervention data, McNemar’s Chi-square tests for categorical variables and Student’s paired t test for continuous variables were used. For knowledge and attitude regarding colorectal cancer, other than those for the screening tests, only those who had heard of colorectal cancer at the time of the survey were included in the analyses. A significance level of p < 0.05 was used for all statistical tests. Analyses were performed with SAS, Version 9 (SAS Institutes, Cary, NC).
Results
LHW Characteristics and Training Results
The male LHW was 66 years old while the ages of the seven female LHWs ranged from 37 to 60 years. Four LHWs were fully employed, one was working part-time and in school, and two were not working. All spoke both Cantonese and Mandarin, and none had any prior health education experience.
All LHWs knew at pre- and post-training that colorectal cancer was preventable and that age 50 was the recommended age for initiation of screening. From pre- to post-training, more LHWs knew that colorectal cancer was the second most common cancer among Chinese Americans (75% to 100%) and that screening tests included FOBT (63% to 88%), sigmoidoscopy (0% to 88%), and colonoscopy (63% to 88%). One LHW did not identify any of the tests at post-intervention and received additional training. At post-training, there was an increase to 100% from varying levels at pre-training for knowledge of the frequency recommended for screening tests and the risk factors for colorectal cancer.
Results from the LHW Outreach Intervention
The average age of the 73 participants was 63.0 years, with 53 (72.6%) women (Table 1). The average number of years residing in the USA was 11.8. Most (81.7%) had less than 12 years of education, and 61.6% had a household income less than $20,000 per year. About two thirds had health insurance (63.2%) and usual place of health care (63.0%). More than half (58.9%) went to Chinese herbalist for some health care. Seventy participants completed both the pre- and post-intervention surveys. The three who did not were women. Compared to those who completed the study, they were similar in age, marital status, employment, and having health insurance and place of care but had shorter US residence (3.3 years), spoke English poorly/not at all (100%), were more educated (33% had less than 12 years of education), had more household income (none with household income <$20,000), and had better self-reported health (66.7% very good/excellent).
Knowledge about colorectal cancer was limited at pre-intervention and increased significantly by post-intervention (Table 2). Only 56.9% and 45.2% had heard of colon cancer and polyps, respectively, at pre-intervention, but 100.0% had heard of both by post-intervention. Knowledge of causes of colorectal cancer increased for fatty diet (36.6% to 82.9%), heredity (24.4% to 70.7%), and older age (12.2% to 61.0%; all p ≤ 0.0001).
There was a statistically significant increase from pre- to post-intervention in the proportion who believed that screening tests could prevent colorectal cancer (39.0% to 82.9%, p = 0.0002). There were no other significant changes from pre- to post-intervention in attitudes and beliefs except an increase in those who were concerned about colorectal cancer (31.7% to 65.9%, p = 0.0005).
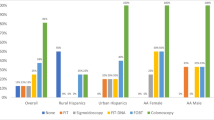
Awareness of all screening tests increased from 31.7% to 97.1% for FOBT (p < 0.0001), 0% to 97.1% for sigmoidoscopy, and 38.4% to 97.1% for colonoscopy (p < 0.0001). Receipt of FOBT increased from 0% to 55.7%, sigmoidoscopy from 0% to 7.1%, and colonoscopy from 0% to 7.1%. There was an increase in those who thought about obtaining an FOBT (33.3% to 53.3%, p = 0.03) or colonoscopy (24.7% to 43.3%, p = 0.008) among those who had never had the test. The proportion who planned on obtaining an FOBT in the next 12 months also increased from 42.5% to 60.0% (p = 0.02).
There was no difference by sex in the demographics and health care variables, except that men were more likely than women to be married (90.0% vs 67.9%, p = 0.04). There was no difference in the variables presented in Table 2 by sex except for one variable. Men were less likely than women to plan on obtaining an FOBT in the next 12 months at pre-intervention (20.0% vs 50.9%, p = 0.02) and at post-intervention (40.0% vs 68.0%, p = 0.057). Among those who remained unscreened, men were less likely to think about obtaining an FOBT (12.5% vs 68.2%, p = 0.012).
Nearly all (96.1%) participants reported that the LHWs helped with colorectal cancer prevention, with 73.0% reporting that LHWs helped to inform about the tests, 67.6% that LHWs showed where to go for the tests, 78.4% that LHWs encouraged to get tests, and 40.5% that LHWs answered questions. Characteristics in LHWs that participants liked were being knowledgeable (67.5%), helpful (88.3%), friendly (83.1%), accessible (66.2%), and respectful (71.4%).
After participating in the LHW program, 26.0% of participants discussed colorectal cancer screening with one to two other people, 31.2% with three to four other people, and 36.4% with five or more other people. After the program, two LHWs participated in health fairs held by NICOS Chinese Health Coalition and taught over 100 participants about colorectal cancer screening using the flipchart. Through the LHW program, one LHW became interested in health outreach and was hired by NICOS to conduct other health-related outreach.
Discussion
The results of this pilot study indicate that the use of lay health worker outreach to promote colorectal cancer screening is feasible among Chinese Americans and is effective, albeit in an uncontrolled study, in increasing the rate of colorectal cancer screening in this population. Other important findings from this study include preliminary information about how LHW outreach may work in this population and the acceptability of LHW outreach among Chinese American men.
There has been increasing interest on how to increase uptake of health interventions that have been proven effective [32]. Despite the size of the Chinese American population and the lack of adequate colorectal cancer screening, there has been only one published intervention to increase this proven modality in this population—a clinic-based intervention in Seattle, WA using a professional health educator, bilingual materials, and direct provision of FOBT cards [13]. That study found that the intervention was superior to usual care for FOBT receipt. The intervention group had an increase of 69% in the receipt of colorectal cancer screening, a rate that is slightly higher than the increase of 55% in this LHW outreach study. The results of both studies show that culturally and linguistically appropriate health education, whether community- or clinic-based, can lead to large increases in the rate of colorectal cancer screening among Chinese Americans.
In addition to the effect on increasing colorectal cancer screening, the LHW outreach participants also increased their knowledge about the known risk factors of colorectal cancer. There was an increase in the knowledge that screening prevents colorectal cancer, although there was no change in knowledge of other prevention modalities such as eating fibers and vegetables or taking aspirin to prevent colorectal cancer. This was because, for simplicity, the intervention focused on screening, and thus, the LHWs did not discuss other modalities other than to acknowledge that they were valid. The lack of emphasis may have led the participants to believe that the other preventive methods may not be effective. Since those other behaviors should be encouraged, this would be an issue to address in future studies.
There was an increase in concern about colorectal cancer, but no changes in the perception of logistical barriers. This is likely a result of the way this LHW outreach program was structured, with the main focus on knowledge and risk, and, other than providing participants with referral to places to go to obtain screening, less focus on providing navigation support. This feature separates the type of outreach conducted by LHWs from patient navigators, one of whose main functions is to provide navigation and logistical support. Future studies with LHWs could include additional components that address logistical problems.
Rogers argued that, among the five stages of diffusion theory’s adoption process—knowledge, persuasion, decision, trial, and adoption—interpersonal contact and social networks are more influential than other modalities, such as mass media, in driving the last two or three phases [33]. Lay health workers in this study successfully transmitted knowledge about colorectal cancer and its screening to their participants. Most participants acknowledged that knowledge delivery was a key component of the LHW outreach, but they reported that the LHWs also helped to provide other important information such as logistics (e.g., where to go to obtain screening) and emotional support to encourage the participants to get screened. Participants also selected the characteristics of being helpful, friendly, and respectful more frequently than being knowledgeable as what they liked about their LHWs. Although this study was not designed to address the question of how LHW outreach works, these interpersonal qualities may have been as important as knowledge diffusion in increasing adoption of colorectal cancer screening among the participants. LHW outreach should be strongly considered in programs that work with minority populations such as Chinese Americans because LHWs have natural cultural and linguistic competence, because LHWs fit the needs of diffusion theory, and there is increasing empirical evidence, including this study, for the effectiveness of LHW outreach [20–24, 34].
A recent review of LHW outreach reported a need for studies with male participants [19]. This study showed that it is feasible to implement LHW outreach for Chinese American men on the topic of colorectal cancer screening. Interestingly, even though some female LHWs worked with male participants, there were minimal differences in the effect of the intervention on knowledge and uptake of colorectal cancer screening between male and female participants. However, men did have lower rates of intention to obtain screening in the future. It was also harder to find qualified men interested in becoming LHWs. These findings suggest that concerns remain about the applicability of LHW outreach methods to ethnic minority men and that LHW outreach with these men should be tested in a larger study.
An important and often underappreciated feature of LHW outreach programs is the building of community capacity to address health concerns. In this study, this occurred in three ways. First, existing social networks, which were probably channels of communication about a variety of issues, including health concerns, were utilized to spread the word about an evidence-based effective intervention, colorectal cancer screening. The message did not stop after the participants listened to the LHWs because many participants reported discussing colorectal cancer screening with others in their networks. Utilizing the social networks in this way may prepare for future health-related outreach by setting the norm for those in the network that this is an acceptable content for communication. Secondly, the LHWs become ready resources for further linguistically and culturally competent interventions on health. This did occur in a direct way, when NICOS utilized trained LHWs to provide teaching about colorectal cancer screening to large numbers of participants at health fairs. The presentation and research skills that they learned will also prepare them to conduct similar work on other health topics. On a more fundamental level, some LHWs become activated to work in health outreach, as in the example of the LHW who then seeked and obtained further employment with NICOS. Finally, the capacity of a community organization such as NICOS to work in research and in cancer prevention also increased, and it is currently working with this team of researchers on other funded projects to carry out community-based participatory research among Chinese Americans.
This study has several important limitations. As a feasibility study, the sample size was small, and there was no control group. The outcome of colorectal cancer screening was based on self-reports, not on medical record validation, and little is known about the validity of self-reports for colorectal cancer screening among Asian Americans.
The findings from this study show that LHW outreach to promote colorectal cancer screening among Chinese American men and women is feasible and possibly effective. Further studies are needed to document the effectiveness of this culturally appropriate intervention and to describe the mechanisms through which this intervention works.
References
US Census Bureau, The American Community-Asians (2004) The American Community Survey Reports 2007. US Department of Commerce, Washington DC
Miller BA, Chu KC, Hankey BF et al (2008) Cancer incidence and mortality patterns among specific Asian and Pacific Islander populations in the US. Cancer Causes Control 19(3):227–256
Le Marchand L, Wilkens LR, Kolonel LN et al (1997) Associations of sedentary lifestyle, obesity, smoking, alcohol use, and diabetes with the risk of colorectal cancer. Cancer Res 57(21):4787–4794
Vernon SW (1997) Participation in colorectal cancer screening: a review. J Natl Cancer Inst 89(19):1406–1422
Selby JV, Friedman GD, Quesenberry CP Jr et al (1992) A case-control study of screening sigmoidoscopy and mortality from colorectal cancer. N Engl J Med 326(10):653–657
Mandel JS, Bond JH, Church TR et al (1993) Reducing mortality from colorectal cancer by screening for fecal occult blood. Minnesota Colon Cancer Control Study. N Engl J Med 328(19):1365–1371
Hardcastle JD, Chamberlain JO, Robinson MH et al (1996) Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet 348(9040):1472–1477
Maciosek MV, Solberg LI, Coffield AB et al (2006) Colorectal cancer screening: health impact and cost effectiveness. Am J Prev Med 31(1):80–89
Maciosek MV, Coffield AB, Edwards NM et al (2006) Priorities among effective clinical preventive services: results of a systematic review and analysis. Am J Prev Med 31(1):52–61
US Preventive Services Task Force (2008) Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 149(9):I44
Wong ST, Gildengorin G, Nguyen T et al (2005) Disparities in colorectal cancer screening rates among Asian Americans and non-Latino whites. Cancer 104(12 Suppl):2940–2947
Kandula NR, Wen M, Jacobs EA et al (2006) Low rates of colorectal, cervical, and breast cancer screening in Asian Americans compared with non-Hispanic whites: cultural influences or access to care? Cancer 107(1):184–192
Tu SP, Taylor V, Yasui Y et al (2006) Promoting culturally appropriate colorectal cancer screening through a health educator: a randomized controlled trial. Cancer 107(5):959–966
Israel BA (1985) Social networks and social support: implications for natural helper and community level interventions. Health Educ Q 12(1):65–80
Brownstein JN, Cheal N, Ackermann SP et al (1992) Breast and cervical cancer screening in minority populations: a model for using lay health educators. J Cancer Educ 7(4):321–326
Schulz AJ, Israel BA, Becker AB et al (1997) “It's a 24-hour thing... a living-for-each-other concept”: identity, networks, and community in an urban village health worker project. Health Educ Behav 24(4):465–480
Swider SM (2002) Outcome effectiveness of community health workers: an integrative literature review. Public Health Nurs 19(1):11–20
WHO (1987) Community health workers: working document for the WHO study group. World Health Organization, Geneva
Rhodes SD, Foley KL, Zometa CS et al (2007) Lay health advisor interventions among Hispanics/Latinos: a qualitative systematic review. Am J Prev Med 33(5):418–427
Sung JF, Blumenthal DS, Coates RJ et al (1997) Effect of a cancer screening intervention conducted by lay health workers among inner-city women. Am J Prev Med 13(1):51–57
Navarro AM, Senn KL, McNicholas LJ et al (1998) Por La Vida model intervention enhances use of cancer screening tests among Latinas. Am J Prev Med 15(1):32–41
Slater JS, Ha CN, Malone ME et al (1998) A randomized community trial to increase mammography utilization among low-income women living in public housing. Prev Med 27(6):862–870
Mock J, McPhee SJ, Nguyen T et al (2007) Effective lay health worker outreach and media-based education for promoting cervical cancer screening among Vietnamese American women. Am J Public Health 97(9):1693–1700
Nguyen TT, Le G, Nguyen T et al (2009) Breast cancer screening among Vietnamese Americans: a randomized controlled trial of lay health worker outreach. Am J Prev Med 37(4):306–313
Engelstad LP, Stewart S, Otero-Sabogal R et al (2005) The effectiveness of a community outreach intervention to improve follow-up among underserved women at highest risk for cervical cancer. Prev Med 41(3–4):741–748
Campbell MK, James A, Hudson MA et al (2004) Improving multiple behaviors for colorectal cancer prevention among African American church members. Health Psychol 23(5):492–502
Nash D, Azeez S, Vlahov D et al (2006) Evaluation of an intervention to increase screening colonoscopy in an urban public hospital setting. J Urban Health 83(2):231–243
Chen LA, Santos S, Jandorf L et al (2008) A program to enhance completion of screening colonoscopy among urban minorities. Clin Gastroenterol Hepatol 6(4):443–450
Christie J, Itzkowitz S, Lihau-Nkanza I et al (2008) A randomized controlled trial using patient navigation to increase colonoscopy screening among low-income minorities. J Natl Med Assoc 100(3):278–284
Myers RE, Hyslop T, Sifri R et al (2008) Tailored navigation in colorectal cancer screening. Med Care 46(9 Suppl 1):S123–S131
Lasser KE, Murillo J, Medlin E et al (2009) A multilevel intervention to promote colorectal cancer screening among community health center patients: results of a pilot study. BMC Fam Pract 10:37
Green LW, Ottoson JM, Garcia C et al (2009) Diffusion theory, and knowledge dissemination, utilization, and integration in public health. Annu Rev Public Health 30:151–174
Rogers EM (2003) Diffusion of innovations, 5th edn. Free Press, New York
Bird JA, McPhee SJ, Ha NT et al (1998) Opening pathways to cancer screening for Vietnamese-American women: lay health workers hold a key. Prev Med 27(6):821–829
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
This project was supported by the National Cancer Institute through the SFSU-UCSF Minority-Serving Institution/Cancer Center Partnership (U56CA96216). Dr. Nguyen was also supported by the National Cancer Institute through the Asian American Network for Cancer Awareness, Research, and Training (U01CA114640).
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Nguyen, T.T., Love, M.B., Liang, C. et al. A Pilot Study of Lay Health Worker Outreach and Colorectal Cancer Screening Among Chinese Americans. J Canc Educ 25, 405–412 (2010). https://doi.org/10.1007/s13187-010-0064-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13187-010-0064-3