
Abstract
Cyclooxygenase-2 (COX-2) is associated with poor-prognosis breast cancer. We used a nude mouse xenograft model to determine the effects of COX-2 inhibition in breast cancer. Oestrogen receptor (ER)-positive MCF7/HER2-18 and ER-negative MDAMB231 breast cancer cell lines were injected into nude mice and allowed to form tumours. Mice then received either chow containing Celecoxib (a COX-2 inhibitor) or control and tumour growth measured. Tumour proliferation, apoptosis, COX-2, lymphangiogenesis and angiogenesis were assessed by immunohistochemistry (IHC), Western blotting or Q-PCR. Celecoxib inhibited median tumour growth in MCF7/HER2-18 (58.7%, P=0.029) and MDAMB231 (46.3%, P=0.0002) cell lines compared to control. Cyclooxygenase-2 expression decreased following Celecoxib treatment (MCF7/HER2-18 median control 65.3% vs treated 22.5%, P=0.0001). Celecoxib increased apoptosis in MCF7/HER2-18 tumours (TUNEL 0.52% control vs 0.73% treated, P=0.0004) via inactivation of AKT (median pAKTser473 57.3% control vs 35.5% treated, P=0.0001 – confirmed at Western blotting). Q-PCR demonstrated decreased podoplanin RNA (lymphangiogenesis marker) in the MCF7/HER2-18 – median 2.9 copies treated vs 66.6 control (P=0.05) and MDAMB231-treated groups – median 160.7 copies vs 0.05 control copies (P=0.015), confirmed at IHC. Cyclooxygenase-2 is associated with high levels of activated AKTser473 and lymphangiogenesis in breast cancer. Cyclooxygenase-2 inhibition decreases tumour growth, and may potentially decrease recurrence, by inactivating AKT and decreasing lymphangiogenesis.
Similar content being viewed by others

Main
Cyclooxygenase-2 (COX-2) is overexpressed in approximately 70% of cases of in situ and 60% of invasive breast cancer (Boland et al, 2004). The COX genes encode for enzymes that catalyse the rate-limiting step of conversion from arachidonic acid to prostaglandins. Two main isoforms, COX-1 and COX-2, were first demonstrated in the early 1990s (Fu et al, 1990; Xie et al, 1991). Cyclooxygenase-1 is constitutively expressed in most tissues, and is responsible for physiological housekeeping functions such as gastric cytoprotection, regulation of renal blood flow and platelet aggregation (Smith et al, 2000). Cyclooxygenase-2 is an inducible isoform, and is expressed by cells involved in the inflammatory process (Subbaramaiah et al, 1996; Smith et al, 2000) (i.e. macrophages, monocytes, synoviocytes) and also in a wide variety of solid epithelial tumours (Gasparini et al, 2003). The increased expression of COX-2 in tumourigenesis is secondary to multiple activations and as a response to growth factors and oncogenes, including those in the EGFR/HER2/RAS/MAP kinase pathway. This latter pathway is of particular interest in breast cancer as HER2 is often upregulated in both invasive and in situ disease and is associated with poor prognosis tumours (Slamon et al, 1987; Sposto and Silverstein, 2002). Conversely, COX-2 is rarely expressed in normal tissue (unless in proximity to an area of neoplasia or inflammation). When COX-2 is expressed in normal tissue, it has been found in a subpopulation of normal breast cells with silenced p16ink4a (which have been postulated as precursors of breast cancer) (Crawford et al, 2004).
Studies of transgenic mice engineered to overexpress COX-2 have shown that these mice form mammary tumours earlier and more often than wild-type mice, their mammary glands contain fewer apoptotic cells and show reduced expression of the proapoptotic proteins BAX and BCl-x(L) (Liu et al, 2001). Elevated COX-2 expression leads to increased tumour recurrence and decreased survival in invasive breast cancer (Crawford et al, 2004). The recent publication of the Women's Health Initiative results (Harris et al, 2003) suggest that the regular use of nonsteroidal anti-inflammatory drugs (NSAIDs) has a significant chemo-preventative effect against developing breast cancer, with a 28% reduction (relative risk 0.72, 95% CI 0.56–0.91) with regular NSAID use for 10 years or more.
Previous studies have shown significant decreases in various solid tumour growths following the administration of COX-2 inhibitors (Connolly et al, 2002; Howe et al, 2002), although there is still a need to clarify the mechanism of action in breast cancer and identify surrogate markers of effect.
The aims of this study were to use a xenograft model of breast cancer to confirm the effect of COX-2 inhibition on tumour growth in vivo, and to subsequently determine the mechanism of action, by studying expression of markers of cell proliferation (Ki67 and p21cip1), apoptosis (TUNEL) and AKT activation.
We also aimed to determine whether Celecoxib perturbed the production of the new lymphatic vessels (lymphangiogenesis). It has recently been demonstrated that expression of the lymphangiogenic factor VEGF-C is significantly elevated in cells overexpressing COX-2 (Su et al, 2004). The production of new lymphatic vessels by the tumour is a key step in the promotion of cancer metastasis and COX-2 inhibitors have been shown to have antimetastatic activity in a metastatic mouse model (Roche-Nagle et al, 2004). In addition, markers of tumour endothelial cell formation have been shown to correlate with prognosis in breast cancer (Davies et al, 2004). In this paper, we used podoplanin, a marker of lymphatic endothelial cells to demonstrate changes in lymphangiogenesis following treatment with Celecoxib in our xenograft model.
Materials and methods
Tumour cell lines
One oestrogen receptor (ER)-positive and one ER-negative breast cancer cell line were chosen for study. MCF7/HER2-18, is an ER-positive MCF7 cell line which had been stably transfected with HER2 (EGFR negative /HER2 positive/ER positive), a gift from Professor CC Benz, University of California San Francisco, and MDAMB231 is an ER-negative breast cancer cell line which is EGFR positive /HER2 negative. All cells were routinely maintained in Dulbecco's Modified Eagle Medium with 10% foetal calf serum, 2 mM glutamine, 100 U penicillin and 100 μg streptomycin per 500 ml. The cells were incubated at 37°C in a humidified environment and passaged at near confluence.
Nude mouse xenograft model
The experimental design followed a well-established female nude mouse model from our department (Gandhi et al, 2000; Chan et al, 2002). Following ethical approval, 2–4 million cells were injected into each flank of female BLAB/c nu/nu mice, aged 6–8 weeks, and allowed to form tumours. The tumours were measured with callipers twice weekly (length × width) and the mice weighed. The mice had free access to feed, water and bedding at all time, and were housed with a 12 h light/dark cycle in filter top cages, maximum six mice per cage.
Tumour volumes (mm3) were calculated by the formula length × length × (width/2). When >75% of the tumours were palpable the mice were randomised to receive either chow containing 0.15% Celecoxib (Celecoxib donated from Pfizer/chow constituted at Purina Mills, USA) or control chow. The tumours continued to be measured and the mice weighed twice weekly. When tumours in either group reached 1 cm3, the experiment was ended in accordance with UK Home Office guidelines and the tumours were harvested. The tumours were then split, with half fixed in 4% formalin and embedded in paraffin blocks for immunohistochemistry (IHC), and the remainder snap frozen in liquid nitrogen.
Immunohistochemistry
Three micron sections of the paraffin blocks were cut onto APES-coated slides. The slides were dewaxed in xylene and rehydrated through graded alcohols to PBS. Staining for COX-2 and Ki67 (Boland et al, 2004) was as described previously. All incubations were carried out at room temperature unless otherwise stated. For p21, pAktser473 and podoplanin, endogenous peroxidase activity was blocked by immersing slides in 0.2% H2O2 in methanol for 10 min. At TUNEL staining, sections were treated with proteinase K for 15 min before quenching endogenous peroxidase activity. Antigen retrieval was performed by immersing slides in citrate buffer (pH 6), in a pressure cooker for p21 (120 s), pAktser473 (100 s) and podoplanin (120 s).
TUNEL
Sections were incubated in equilibration buffer (Apoptag Kit, Intergen, Norcross, GA, USA) for 1 h. Then working strength TdT enzyme was applied to the sections, which were incubated for 1 h at 37°C. Immersing the sections in working strength stop buffer for 10 min halted the reaction. Following washing in PBS, the sections were incubated with anti-digoxigenin conjugate for 30 min.
p21cip1
Sections were incubated with the Mouse-on-Mouse (MOM) kit blocking solution with avidin for 1 h. Following washing in PBS, the sections were incubated for 5 min with the working solution of MOM dilutent for 5 min, and then incubated with the primary mouse anti-p21 antibody (DAKO M7202 mouse monoclonal) 1 : 25 made up in MOM dilutent with biotin for 60 min. Following washing in PBS, sections were incubated with working MOM kit biotinylated anti-mouse IgG for 30 min.
Phosphorylated Aktser473
Nonspecific binding was blocked with 10% normal goat serum in PBS with avidin for 15 min. The sections were then incubated with the primary phosphor-AKT/PKBser473 antibody (rabbit polyclonal, Cell Signalling Technology, Danvers, MA, USA, #9277) 1 : 30 in 10% normal goat serum with biotin for 2 h, then with the biotinylated goat anti-rabbit secondary 1 : 200 (Vector BA1000) in 10% normal goat serum for 1 h.
Podoplanin
Nonspecific binding was blocked by incubating slides in 10% normal rabbit serum in PBS with avidin for 30 min, the slides were then incubated with the primary monoclonal antibody to podoplanin (ab11936, AbCam) 1 : 500 made up in 10% normal rabbit in PBS with biotin for 2 h. After washing in PBS, the biotinylated rabbit anti-hamster secondary was added (1 : 500 ab6782 AbCam) for 1 h.
For p21, pAktser473, and podoplanin, following the secondary antibody, sections were incubated with Vectastain Elite ABC reagent (Vector, Peterborough, UK) for 30 min. All stainings were visualised with DAB, counter-stained with haematoxylin, slides then dehydrated, cleared and mounted.
IHC scoring
All scorings were carried out blind to the treatment group. For Ki67, p21cip1 and pAktser473, the percentage of positive nuclei out of at least 1000 counted, was determined over representative tumour areas. At least 3000 cells were counted when determining the TUNEL score, as there were few apoptotic cells in each specimen. Reproducibility and accuracy of the scoring was ensured by repeat scoring and multiple observer scoring of the initial samples. For pAktser473 the cytoplasmic staining intensities were scored on a rating 0–3+. The COX-2 cytoplasmic staining was scored on both the percentage of positive cells and the staining intensity for the MCF7/HER2-18. The grading of intensity for each section was determined following reference to sections taken to be representative for each grade of intensity; 0=no staining, 1=mild staining, 2=moderate staining, 3=strong, 4=very strong. At least 1000 cells were also counted for each section, and the percentage of positively staining cells determined, and assigned a numerical score; 1=no staining, 2=<10%, 3=11–50%, 4⩾50%. It was considered inappropriate to use the intensity score for the MDAMB231 cells, as COX-2 expression was localised to cytoplasmic vesicles, and there was no discernable difference in intensity. Scoring was therefore calculated from the proportion of cells containing cytoplasmic vesicles. All scorings were carried out using a light microscope, grid graticule and cell counter at × 400 magnification. For podoplanin, vessel density was calculated using a Chalkley point graticule. Scoring was taken as the median number of vessels crossing the points, from six separate fields of high vessel density, at × 400 magnification.
Western blotting
Snap frozen tumour samples were utilised for Western blotting. Crushing the tissue samples in liquid nitrogen created tumour powder. Lysis buffer was then added to create cell lysates, which were left on ice for 40 min before centrifugation (at 13 000 r.p.m. for 10 min at 4°C) and protein estimation (using the Biorad protein assay solution and a GeneQuant pro machine).
Following the addition of sample buffer to the lysates, 50 μg of protein was resolved onto SDS gel and transferred to Hybond membranes using a TRIS/glycine/SDS electrode tank buffer, run overnight. Membranes were blocked with 5% skimmed milk–TBS-Tween for 1 h and then probed with the primary antibodies; pPKB/pAKTser473 (1 : 1000 #9271 Cell Signaling Technology) and then total PKB/AKT (1 : 1000 #9272 Cell Signaling Technology) as a loading control.
After washing in TBS-Tween, the membranes were incubated with a donkey anti-rabbit HRP-linked secondary antibody (1 : 1000 Amersham Biosciences NA934V, Piscataway, NJ, USA) for 1 h. Following thorough washing in TBS-Tween for 6 × 10 min, the level of specific protein was visualised by chemiluminescence (Supersignal West Dura extended duration substrate; Pierce Biotechnology, Rockford, IL, USA). Both total PKB/AKT and pPKB/AKTser473 bring up single bands of 60 kDa. Quantification of protein levels was estimated at subsequent densitometry using GeneTools from Syngene version 3.05.
Q-RT-PCR
The assessment of lymphangiogenesis (podoplanin) and angiogenesis (CD31) was determined by quantitative PCR utilising snap-frozen tumour samples, which were stored in liquid nitrogen until use. Samples were homogenised to extract RNA using RNA-Zol reagent (Abgene homogenisation kit, Epsom, UK) as per manufacturer's instructions. cDNA was subsequently generated from 1 μg of RNA using the Enhanced Avian Reverse Transcriptase kit (Abgene, UK). Levels of podoplanin and CD31 transcripts were estimated using the Ampliflour Uni Primer detection kit (Intergen, UK) and 2 × Q-PCR master mix according to manufacturers instructions. Quantification was carried out using the iCycler iQ™ (Bio-Rad, Hemel Hempstead, UK). Detection of the fluorescence was carried out during the annealing step. Copy numbers for podoplanin and CD31 expression in the samples were determined from in-house standard curves.
Statistical analysis
Statistical analysis was performed using the Stats Direct statistical software package and the Mann–Whitney U test for continuous variables. All tests were two-tailed with a 5% significance level used throughout.
Results
Tumour growth
There was decreased tumour growth following Celecoxib treatment in both the MCF7/HER2-18 (P=0. 029) and MDAMB231 breast cancer cell lines (P=0.0003) (Table 1). These results represent the median values from a total of 43 controls and 41 treated tumours in the MCF7/HER2-18 cell line and 19 controls and 20 treated tumours in the MDAMB231 cell line. The median tumour growth inhibition (TGI) was calculated by comparing the median control growth to the individual treated tumour growth as shown by the equation:

The median TGI was 58.7% in the MCF7/HER2-18 tumours and 46.3% in the MDAMB231 tumours (Table 1). No differences in weight between control and treated mice were seen.
Celecoxib does not perturb cell proliferation
The differences in tumour growth were not a product of alterations in cell proliferation as there was no change in the median number of proliferating cells in the cell lines between the control and the treated samples as assessed by Ki67 (Table 1). Also, the p21cip1 pathway was not perturbed by the administration of Celecoxib, as there were no significant changes in the median number of cells in each cell line expressing p21cip1 (Table 1).
Apoptosis significantly increased following Celecoxib treatment
There was a significant increase in cell apoptosis in the ER-positive MCF7/HER2-18 cell line following treatment with Celecoxib (median control TUNEL staining 0.52% (IQR 0.46–0.68), median treated TUNEL staining 0.77 (IQR 0.46–0.68) (Table 1)). There was also an increase in apoptosis in the MDAMB231 cell line that did not reach statistical significance.
Celecoxib inactivates Akt
Akt (PKB) is a member of the serine/threonine kinases, which in its activated state, is antiapoptotic. Phosphorylation of Akt at the ser473 site was significantly decreased in the MCF7/HER2-18 cell line following treatment with Celecoxib, this was shown at both Western blotting (Figure 1A) and IHC (Figures 2A and B). In the control samples, pAktser473 was found to be in both the cytoplasmic and nuclear areas of the cell, and was distributed throughout the specimen. Celecoxib decreased both the nuclear and cytoplasmic components of pAktser473 (Figures 2A and B). The median number of nuclei that stained positive for pAKTser473 dropped from 57.3% (IQR 54.1–61.1) in the MCF7/HER2-18 controls to 35.7% (IQR 24.4–47.6%); P=0.0001. In the ER-negative MDAMB-231 cell line, no changes in pAktser473 were seen at either Western blotting (Figure 1B) or IHC (Figure 2C), but as can be seen from the IHC sections, the distribution of pAktser473 in the MDAMB231 cell line differed from the MCF7/HER2-18 cell line in that there was very low levels of nuclear pAktser473 (Figure 2C). It therefore appears that the subcellular location of pAktser473 is an important determinant of Celecoxib signalling effect.

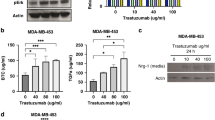
Western blot MCF7/HER2-18 pAktser473, total Akt. (A) Representative Western blots from MCF7/MCF7/HER2-18 control and Celecoxib-treated tumours. The top blot shows a decrease in pAKTser473 in the treated samples (60 kDa). At the bottom, no change was seen in total AKT (60 kDa) as a loading control. The median arbitrary quantity from the control to treated tumours showed a decrease of 28.2% (IQR −1.5–89.1%) at densitometry over all of the tumours studied. (B) A representative Western blot using lysates from the MDAMB231 cell line. There was no overall pattern seen. Total AKT was used as a loading control (60 kDa), bottom blot.

The MCF7/HER2-18 control tumours showed expression of pAKTser473 in both the cell nucleus and the cell cytoplasm (A). Following Celecoxib treatment both the nuclear and cytoplasmic components of pAKTser473 decreased, this was predominantly seen as a decrease in nuclear pPAKTser473 (B), which decreased from a median of 57.3% (IQR 54.1–61.6) in the control tumours to 35.7% (IQR 24.4–47.6) in the treated tumours, P=0.0001. The MDAMB231 cell line expressed predominantly cytoplasmic pAKTser473 (C), which did not significantly decrease following Celecoxib treatment. Decreases in lymphatic vessel density were seen in the MCF7/HER2-18 xenografts (D and E) from a median of 12 Chalkley counts to 9 Chalkley counts (P=0.0001). The MDAMB231 xenografts (F and G) also showed a decrease in podoplanin expression from a median of 7 Chalkley counts to 4 Chalkley counts, P=0.0001) following COX-2 inhibition. Representative IHC staining for pAKTser473 and podoplanin in the harvested xenografts: (A) pAKTser473 staining in MCF7/HER2-18 control xenografts (× 400); (B) pAKTser473 staining in MCF7/HER2-18 treated xenografts (× 400); (C) pAKTser473 staining in MDAMB231 control xenografts (× 400); (D) Podoplanin staining in MCF7/HER2-18 control xenografts (× 400); (E) Podoplanin staining in MCF7/HER2-18 treated xenografts (× 400); (F) Podoplanin staining in MDAMB231 control xenografts (× 100); (G) Podoplanin staining in MDAMB231 treated xenografts (× 100).
COX-2 protein expression
The pattern of COX-2 expression varied between the cell lines. The MCF7/HER2-18 cell line showed homogeneous cytoplasmic staining across the majority of cells. Celecoxib treatment decreased both the median number of positive cells (median control 65.3% (IQR 60.3–77.4), median treated 22.5 (IQR 1.1–60.3)) and median staining intensity (Table 1), reflecting a significantly reduced median immunoscore (Figure 3) of 3 in the treated group, compared to 6 in the control group (P=0.0001). However, the MDAMB231 cell line showed staining that was confined to cytoplasmic vesicles, and therefore staining intensity could not be determined and the scoring was based solely on the number of cells that contained the vesicles. Tumours that had been exposed to Celecoxib again showed a significantly decreased staining for COX-2 protein expression (median control 26.6% (IQR 12.0–32.4), treated 9.4% (IQR 3.9–18.1) (Table 1)). In the ER-positive MCF7/HER2-18 tumours, the percentage of cells that expressed COX-2 in the cytoplasm was significantly correlated to growth; correlation co-efficient 0.4 (P=0.02).

Cyclooxygenase-2 immunoscore in control and Celecoxib-treated MCF7/HER2-18 tumours. Cyclooxygenase-2 immunoscore was calculated as the sum of the intensity score 0–4 (0=none, 1=mild, 2=moderate, 3=strong, 4=very strong) and the percent positivity score (0=nil, 1⩽10%, 2=10–50%, 3⩾50%). No intensity score and therefore immunoscore could be calculated for the MDAMB231 cell line as the staining was confined in cytoplasmic vesicles.
Lymphangiogenesis
Q-PCR showed a significant decrease in median podoplanin RNA from the control to the treated tumours. This was seen in both the MCF7/HER2-18 and the MDAMB231 cell lines. The median number of RNA copies per μl was 66.61 (IQR 27.87–330.50) in the MCF7/HER2-18 control and fell to 2.94 copies (IQR 0.27–18.50) in the treated tumours (P=0.05) (Table 2). In the MDAMB231 tumours the median number of RNA copies per μl was 160.65 in the control tumours (2.14–174.75) and 0.05 (IQR 0.00–2.99) in the treated group (P=0.015). CD31, a marker of angiogenesis also showed reduced numbers of RNA following Celecoxib treatment (Table 2). Our findings were confirmed at the protein level following immunohistochemical staining for podoplanin (Figures 2D–G). At IHC the median number of Chalkley counts in the MCF7/HER2-18 cell line fell from 12 (IQR 9—14) in the control tumours to 9 (IQR 6–10) in the treated samples (P=0.0001), and from 7 (IQR 5–19) in the MDAMB231 tumours, to 4 (IQR 3–6) in the treated samples (P=0.0001) (Table 2). At IHC it could clearly be seen that the majority of lymphatics were in clusters around the periphery of the tissue; therefore, Western blots for podoplanin were not performed.
Discussion
COX-2 inhibition decreases tumour growth
High rates of tumour growth and metastasis lead to death from breast cancer. In the nude mice, median tumour growth was inhibited by 58.7% in the ER-positive MCF7/HER2-18 tumours and by 46.3% in the ER-negative MDAMB231 tumours, following treatment with Celecoxib. Oestrogen receptor-negative tumours are unresponsive to hormonal manipulation, by way of aromatase inhibitors and tamoxifen, and conventional treatment options are therefore limited. Perturbing the COX-2 signalling pathway may prove to be an important novel therapeutic strategy in both ER-positive and ER-negative tumours reducing the rate of tumour growth.
Celecoxib increases apoptosis via inactivation of Akt
The mechanism of action of Celecoxib in inhibiting tumour growth was by increasing apoptosis. In the MCF7/HER2-18 cell line, the median number of cells showing apoptosis increased by 40% from the control to the treated tumours. The fine balance between apoptosis and proliferation is crucial for regulating growth; therefore, even the small numerical changes in apoptosis translate to a large percentage difference, and a significant effect on growth. There were no discernable changes in cell proliferation. This has important implications for current and future trials utilising Celecoxib in breast cancer, as apoptosis, not proliferation should be used as the primary endpoint. Mechanistically, the increase in apoptosis was mediated by inactivation of Akt in the MCF7/HER2-18 cell line. The decrease in pAktser473 that we demonstrated was predominantly nuclear with a median decease of nuclear expression from 57 to 36%. Akt (also known as PKB) is a serine threonine kinase that acts downstream of PI3 kinase in the prosurvival pathway. It is thought that activation follows recruitment to the plasma membrane and phosphorylation of both its serine and threonine residues. It has been demonstrated that within 30 min of activation, Akt detaches from the cytoplasm and relocates to the nucleus. In the nucleus there is modulation of the phosphorylation of a variety of transcription factors (Andjelkovic et al, 1997), including phosphorylation of FKHR1 (Rena et al, 1999) and the forkhead transcription factor AFX (Kops et al, 1999) promoting their cytoplasmic retention – distancing them from their nuclear targets. It has previously been shown that the growth factors PDGF and IGF-1 both cause an increase in the amounts of intra nuclear Akt (Borgatti et al, 2000). There is still, however, some debate as to whether activation occurs solely in the cytoplasm with subsequent translocation to the nucleus, or whether there is a nuclear component to the event itself (Borgatti et al, 2000). The subcellular localisation of pAkt is therefore important for its signalling effect which in the MCF7/HER2-18 cell line was both cytoplamic and nuclear, but predominantly cytoplasmic in the MDAMB231's. This lack of nuclear activated Akt could explain why there was no decrease in phosphorylation seen in the MDAMB231 tumours (and a less substantial increase in apoptosis). Reduced Akt activation following Celecoxib treatment has also been seen in prostate (Hsu et al, 2000) and hepatocellular (Leng et al, 2003) cancer cells. The importance of Akt inactivation in increasing apoptosis was confirmed in PC-3 prostate cancer cells that were engineered to constitutively overexpress Akt which showed reduced apoptosis following Celecoxib treatment compared to cells without constitutively active Akt (Hsu et al, 2000).
Celecoxib reduces lymphatic vessel formation
Celecoxib reduced levels of the lymphatic endothelial cell marker, podoplanin RNA by 87% in the MCF7/HER2-18 and 99.9% in the MDAMB231 tumours. The control samples showed variable levels of podoplanin RNA (as seen by the interquartile range values), showing that lymphatic response is specific to the individual tumour/host. Following Celecoxib treatment this range was much less variable, with in some cases a complete lack of expression of podoplanin RNA. The decrease in expression was also seen at a protein level following Chalkley vessel counts; where the lymphatic vessels were predominantly clustered around the tumour periphery. In addition, there was a reduction in the median number of RNA copies of CD31 (an angiogenic marker) by 84% in the MCF7/HER2-18 and 91% in the MDAMB231 tumours. The antiangiogenic properties of the COX-2 inhibitors have already been demonstrated (Masferrer et al, 2000). As CD31 and podoplanin RNA were both greatly reduced in the MDAMB231 tumours, this may account for the fact that there was decrease in growth of the MDAMB231 tumours following Celecoxib, even though the increase in apoptosis failed to reach statistical significance. Review of the IHC sample sections showed large areas of central necrosis in the MDAMB231-treated tumours, which again would be consistent with an insufficient blood supply in these Celecoxib-treated tumours.
In breast cancer the primary mode of metastasis is via the lymphatics and COX-2 expression correlates with lymph node metastasis in breast cancer (Ranger et al, 2004). Taken altogether the cumulating data regarding COX-2 inhibition and lymphangiogenesis indicate that there is interesting potential of COX-2 inhibitors being used as antimetastatic agents.
Celecoxib decreases COX-2 protein expression
Celecoxib treatment decreased the levels of COX-2 protein expression in both cell lines. Therefore, Celecoxib is not simply blocking the effect of COX-2, but is also perturbing COX-2 protein production; a finding noted in previous studies (Cheng et al, 2002; Agarwal et al, 2003). In COX-2 expressing HT29 colon cancer cell lines, COX-2 inhibition with another selective COX-2 inhibitor SC236 (a structural analogue of Celecoxib) showed that at high levels of inhibitor (concentrations greater than 75 μm), COX-2 enzyme activity was completely inactivated. Decreased levels of COX-2 protein expression and increases in apoptosis were seen. Whereas Sulindac sulphide (an inhibitor of COX-1 and COX-2) did not promote any changes in apoptosis and also showed no decrease in COX-2 protein expression) (Agarwal et al, 2003). The antiapoptotic effects of COX-2 were better correlated to decreases in COX-2 protein expression than inhibition of enzymatic activity (Agarwal et al, 2003). It has been suggested that the prostaglandin products of COX-2, mainly PgE2, positively feed back to produce enhanced COX-2 protein expression (Faour et al, 2001). Therefore blocking COX-2, and hence prostaglandin production, would decrease this positive feedback loop. NFκB also regulates the COX-2 gene. Celecoxib abrogates TNF-induced activation of NFκB with inhibition of Akt (Shishodia et al, 2004), and therefore another possible explanation for the decrease in COX-2 protein levels seen could be that there is inhibition of NFκB-induced promoter activity of the COX-2 gene, with subsequent decreases in COX-2 protein expression.
COX-2 independent mechanisms of Celecoxib action
In the ER-positive MCF7/HER2-18 treated tumours, the percentage of residual COX-2 expression significantly correlated with tumour growth, but in the ER-negative MDAMB231-treated tumours, there was no correlation between residual COX-2 expression and growth. This raises the possibility of COX-2 independent effects of Celecoxib in these ER-negative tumours. Further work needs to be carried out to explore the possible COX-2 independent effects of these inhibitors and possible different modes of action in ER-positive vs ER-negative cases. New generation products, which are structurally similar to the COX-2 inhibitors, but lack COX-2 inhibiting effects, are currently under development.
Future direction
We have shown that Celecoxib significantly decreases breast tumour growth in this nude mouse model and clinical studies are underway to investigate the effect in patient populations. Cyclooxygenase-2 inhibitors are showing great promise for their potential therapeutic benefit in a range of cancers; however there has been recent concern over potential cardiotoxicity. This was due to an increased risk of cardiovascular events following treatment with another COX-2 inhibitor Rofecoxib (Vioxx® – now withdrawn) that was highlighted following the publication of the APPROVe trial (Bombardier et al, 2000; Bresalier et al, 2005). In 2005 the New England Journal of Medicine published a review of Celecoxib cardiac safety which raised concerns over prolonged high-dose COX-2 inhibition (Solomon et al, 2005). A review of the data by Kimmel et al (2005) stated that patients who had been taking Rofecoxib had a three times greater risk of developing a myocardial infarction than patients taking Celecoxib, but the overall safety of Celecoxib is still under debate. As Celecoxib has now been shown to significantly decrease tumour growth, there is an urgency to develop new inhibitors that do not have the potential cardiotoxicity. We must maintain the momentum for further investigation of this class of drug, and its descendents, in relationship to their chemotherapeutic potential and mechanisms of action.
In summary, Celecoxib significantly decreased ER-positive and ER-negative breast tumour growth in our nude mouse xenograft model. The mechanism of action was via inactivation of AKT permitting increased cell death in the ER-positive tumours. The primary mode of breast tumour spread is via the lymphatics. Increasing evidence suggests that COX-2 has an important role in lymphangiogenesis and we have shown that COX-2 inhibition decreases new lymphatic vessel formation with the potential decrease in metastatic spread of both ER-positive and ER-negative breast tumours.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Agarwal B, Swaroop P, Protiva P, Raj SV, Shirin H, Holt PR (2003) Cox-2 is needed but not sufficient for apoptosis induced by Cox-2 selective inhibitors in colon cancer cells. Apoptosis 8: 649–654
Andjelkovic M, Alessi DR, Meier R, Fernandez A, Lamb NJ, Frech M, Cron P, Cohen P, Lucocq JM, Hemmings BA (1997) Role of translocation in the activation and function of protein kinase B. J Biol Chem 272: 31515–31524
Boland GP, Butt IS, Prasad R, Knox WF, Bundred NJ (2004) COX-2 expression is associated with an aggressive phenotype in ductal carcinoma in situ. Br J Cancer 90: 423–429
Borgatti P, Martelli AM, Bellacosa A, Casto R, Massari L, Capitani S, Neri LM (2000) Translocation of Akt/PKB to the nucleus of osteoblast-like MC3T3-E1 cells exposed to proliferative growth factors. FEBS Lett 477: 27–32
Bombardier C, Laine L, Reicin A, Shapiro D, Burgos-Vargas R, Davis B, Day R, Ferraz MB, Hawkey CJ, Hochberg HC, Kvien TK, Schnitzer TJ, VIGOR Study Group (2000) Comparison of upper Gastrointestinal toxicity of Rofecoxib and Naproxen in patients with rheumatoid arthritis. N Eng J Med 343: 1520–1528
Bresalier RS, Sandler RS, Quan H, Bolognese JA, Oxenius B, Horgan K, Lines C, Riddell R, Morton D, Lanas A, Konstam MA, Baron JA (2005) Adenomatous Polyp Prevention on Vioxx (APPROVe) Trial Investigators. N Engl J Med 352: 1092–1107
Chan KC, Knox WF, Gee JM, Morris J, Nicholson RI, Potten CS, Bundred NJ (2002) Effect of epidermal growth factor receptor tyrosine kinase inhibition on epithelial proliferation in normal and premalignant breast. Cancer Res 62: 122–128
Cheng HF, Wang CJ, Moeckel GW, Zhang MZ, McKanna JA, Harris RC (2002) Cyclooxygenase-2 inhibitor blocks expression of mediators of renal injury in a model of diabetes and hypertension. Kidney Int 62: 929–939
Connolly EM, Harmey JH, O'Grady T, Foley D, Roche-Nagle G, Kay E, Bouchier-Hayes DJ (2002) Cyclo-oxygenase inhibition reduces tumour growth and metastasis in an orthotopic model of breast cancer. Br J Cancer 87: 231–237
Crawford YG, Gauthier ML, Joubel A, Mantei K, Kozakiewicz K, Afshari CA, Tlsty TD (2004) Histologically normal human mammary epithelia with silenced p16(INK4a) overexpress COX-2, promoting a premalignant program. Cancer Cell 5: 263–273
Davies G, Cunnick GH, Mansel RE, Mason MD, Jiang WG (2004) Levels of expression of endothelial markers specific to tumour-associated endothelial cells and their correlation with prognosis in patients with breast cancer. Clin Exp Metastasis 21: 31–37
Faour WH, He Y, He QW, de Ladurantaye M, Quintero M, Mancini A, Di Battista JA (2001) Prostaglandin E(2) regulates the level and stability of cyclooxygenase-2 mRNA through activation of p38 mitogen-activated protein kinase in interleukin-1 beta-treated human synovial fibroblasts. J Biol Chem 276: 31720–31731
Fu JY, Masferrer JL, Seibert K, Raz A, Needleman P (1990) The induction and suppression of prostaglandin H2 synthase (cyclooxygenase) in human monocytes. J Biol Chem 265: 16737–16740
Gandhi A, Holland PA, Knox WF, Potten CS, Bundred NJ (2000) Effects of a pure antiestrogen on apoptosis and proliferation within human breast ductal carcinoma in situ. Cancer Res 60: 4284–4288
Gasparini G, Longo R, Sarmiento R, Morabito A (2003) Inhibitors of cyclo-oxygenase 2: a new class of anticancer agents? Lancet Oncol 4: 605–615
Harris RE, Chlebowski RT, Jackson RD, Frid DJ, Ascenseo JL, Anderson G, Loar A, Rodabough RJ, White E, McTiernan A (2003) Breast cancer and nonsteroidal anti-inflammatory drugs: prospective results from the Women's Health Initiative. Cancer Res 63: 6096–6101
Howe LR, Subbaramaiah K, Patel J, Masferrer JL, Deora A, Hudis C, Thaler HT, Muller WJ, Du B, Brown AM, Dannenberg AJ (2002) Celecoxib, a selective cyclooxygenase 2 inhibitor, protects against human epidermal growth factor receptor 2 (HER-2)/neu-induced breast cancer. Cancer Res 62: 5405–5407
Hsu AL, Ching TT, Wang DS, Song X, Rangnekar VM, Chen CS (2000) The cyclooxygenase-2 inhibitor celecoxib induces apoptosis by blocking Akt activation in human prostate cancer cells independently of Bcl-2. J Biol Chem 275: 11397–11403
Kimmel SE, Berlin JA, Reilly M, Jaskowiak J, Kishel L, Chittams J, Strom BL (2005) Patients exposed to Rofecoxib and Celecoxib have different odds of non fatal myocardial infarction. Ann Intern Med 142: 157–164
Kops GJ, de Ruiter ND, De Vries-Smits AM, Powell DR, Bos JL, Burgering BM (1999) Direct control of the Forkhead transcription factor AFX by protein kinase B. Nature 398: 630–634
Leng J, Han C, Demetris AJ, Michalopoulos GK, Wu T (2003) Cyclooxygenase-2 promotes hepatocellular carcinoma cell growth through Akt activation: evidence for Akt inhibition in celecoxib-induced apoptosis. Hepatology 38: 756–768
Liu CH, Chang SH, Narko K, Trifan OC, Wu MT, Smith E, Haudenschild C, Lane TF, Hla T (2001) Overexpression of cyclooxygenase-2 is sufficient to induce tumorigenesis in transgenic mice. J Biol Chem 276: 18563–18569
Masferrer JL, Leahy KM, Koki AT, Zweifel BS, Settle SL, Woerner BM, Edwards DA, Flickinger AG, Moore RJ, Seibert K (2000) Antiangiogenic and antitumor activities of cyclooxygenase-2 inhibitors. Cancer Res 60: 1306–1311
Ranger GS, Thomas V, Jewell A, Mokbel K (2004) Elevated cyclooxygenase-2 expression correlates with distant metastases in breast cancer. Anticancer Res 24: 2349–2351
Rena G, Guo S, Cichy SC, Unterman TG, Cohen P (1999) Phosphorylation of the transcription factor forkhead family member FKHR by protein kinase B. J Biol Chem 274: 17179–17183
Roche-Nagle G, Connolly EM, Eng M, Bouchier-Hayes DJ, Harmey JH (2004) Antimetastatic activity of a cyclooxygenase-2 inhibitor. Br J Cancer 91: 359–365
Shishodia S, Koul D, Aggarwal BB (2004) Cyclooxygenase (COX)-2 inhibitor celecoxib abrogates TNF-induced NF-kappa B activation through inhibition of activation of I kappa B alpha kinase and Akt in human non-small cell lung carcinoma: correlation with suppression of COX-2 synthesis. J Immunol 173: 2011–2022
Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL (1987) Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 235: 177–182
Smith WL, DeWitt DL, Garavito RM (2000) Cyclooxygenases: structural, cellular, and molecular biology. Annu Rev Biochem 69: 145–182
Solomon SD, McMurray JJ, Pfeffer MA, Wittes J, Fowler R, Finn P, Anderson WF, Zauber A, Hawk E, Bertagonolli M, Adenoma prevention with Celecoxib (APC) study investigators (2005) Cardiovascular risk associated with Celecoxib in a clinical trial for Colorectal Adenoma Prevention. N Eng J Med 352: 1071–1080
Sposto R, Silverstein MJ (2002) Predicting local recurrence in pateints with ductal carcinoma in situ. In Ductal Carcinoma In Situ of the Breast, MJ Silverstein (ed) Chapter 21, pp. 255–263. Lippncott, Williams and Wilkins: Philadelphia, USA
Su JL, Shih JY, Yen ML, Jeng YM, Chang CC, Hsieh CY, Wei LH, Yang PC, Kuo ML (2004) Cyclooxygenase-2 induces EP1- and HER-2/Neu-dependent vascular endothelial growth factor-C up-regulation: a novel mechanism of lymphangiogenesis in lung adenocarcinoma. Cancer Res 64: 554–564
Subbaramaiah K, Telang N, Ramonetti JT, Araki R, DeVito B, Weksler BB, Dannenberg AJ (1996) Transcription of cyclooxygenase-2 is enhanced in transformed mammary epithelial cells. Cancer Res 56: 4424–4429
Xie WL, Chipman JG, Robertson DL, Erikson RL, Simmons DL (1991) Expression of a mitogen-responsive gene encoding prostaglandin synthase is regulated by mRNA splicing. Proc Natl Acad Sci USA 88: 2692–2696
Acknowledgements
We would like to thank Professor CC Benz for his kind gift of the MCF7/HER2-18 cell line. We would like to thank Pfizer for the donation of the Celecoxib. NLP Barnes was assisted by a Royal College of Surgeons of England Research Grant. This study was funded by an educational grant from Pfizer/Pharmacia.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Barnes, N., Warnberg, F., Farnie, G. et al. Cyclooxygenase-2 inhibition: effects on tumour growth, cell cycling and lymphangiogenesis in a xenograft model of breast cancer. Br J Cancer 96, 575–582 (2007). https://doi.org/10.1038/sj.bjc.6603593
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6603593
Keywords
This article is cited by
-
Cyclooxygenase activity mediates colorectal cancer cell resistance to the omega-3 polyunsaturated fatty acid eicosapentaenoic acid
Cancer Chemotherapy and Pharmacology (2021)
-
Role of platelets and platelet receptors in cancer metastasis
Journal of Hematology & Oncology (2018)
-
The Emerging Roles of Steroid Hormone Receptors in Ductal Carcinoma in Situ (DCIS) of the Breast
Journal of Mammary Gland Biology and Neoplasia (2018)
-
Synergistic effect between celecoxib and luteolin is dependent on estrogen receptor in human breast cancer cells
Tumor Biology (2015)
-
COX-2 expression is predictive for early relapse and aromatase inhibitor resistance in patients with ductal carcinoma in situ of the breast, and is a target for treatment
British Journal of Cancer (2014)
