
Abstract
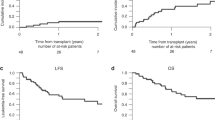
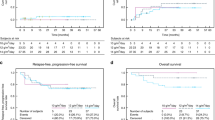
Busulfan and cyclophosphamide (BuCy) are currently the most widely used myeloablative regimen to treat malignancies with allogeneic stem cell transplantation. Fludarabine has considerable efficacy in both immunosuppression and tumor cells killing with a minimal extramedullary toxicity. We evaluated the efficacy of 40 mg/m2 fludarabine i.v. for 5 days and busulfan 4 mg/kg/day p.o. for 4 days as myeloablative conditioning regimen in 70 patients (median age 24 years) with acute leukemia or chronic phase of myelogenous leukemia. They all had human leukocyte antigen-matched sibling donors. The patients received 10 μg/kg granulocyte colony stimulating factor (GCSF), 24 h after stem cell infusion until engraftment occurred. Graft-versus-host disease (GVHD) prophylaxis included 3 mg/kg cyclosporine-A i.v. from day −2 to +6 followed by 12 mg/kg p.o. until day +60. The median time of neutrophil recovery (>0.5 × 109/l) and platelet recovery (>20 × 109/l) were 10 and 12 days, respectively. Mucositis (93%) and hepatic toxicity (16%) resolved with conservative therapy. The incidence of acute GVHD grade I-II and III-IV were 38.6 and 15.7% respectively. Overall survival and disease-free survival were 71 and 64% respectively with 17 months median follow-up for surviving patients. We conclude that FluBu may be used as a substitute for BuCy with almost the same efficacy and with a lower transplant adverse effect but to increase anti-leukemic effects, especially in acute lymphoblastic leukemia patients, it needs some modifications.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Santos GW, Tutschka PJ, Brookmeyer R, Saral R, Beschorner WE, Bias WB et al. Marrow transplantation for acute nonlymphocytic leukemia after treatment with busulfan and cyclophosphamide. N Engl J Med 1983; 309: 1347–1353.
Tutschka PJ, Copelan EA, Klein JP . Bone marrow transplantation for leukemia following a new busulfan and cyclophosphamide regimen. Blood 1987; 70: 1382–1388.
Andersson BS, Kashyap A, Gian V, Wingard JR, Fernandez H, Cagnoni PJ et al. Conditioning therapy with intravenous busulfan and cyclophosphamide (IV BuCy2) for hematologic malignancies prior to allogeneic stem cell transplantation: a phase II study. Biol Blood Marrow Transplant 2002; 8: 145–154.
McDonald GB, Hinds MS, Fisher LD, Schoch HG, Wolford JL, Banaji M et al. Veno-occlusive disease of the liver and multiorgan failure after bone marrow transplantation: a cohort study of 355 patients. Ann Intern Med 1993; 118: 255–267.
McDonald GB, Slattery JT, Bouvier ME, Ren S, Batchelder AL, Kalhorn TF et al. Cyclophosphamide metabolism, liver toxicity, and mortality following hematopoietic stem cell transplantation. Blood 2003; 101: 2043–2048.
Jones RJ, Lee KS, Beschorner WE, Vogel VG, Grochow LB, Braine HG et al. Venoocclusive disease of the liver following bone marrow transplantation. Transplantation 1987; 44: 778–783.
Vaughan WP, Dennison JD, Reed EC, Klassen L, McGuire TR, Sanger WG et al. Improved results of allogeneic bone marrow transplantation for advanced hematologic malignancy using busulfan, cyclophosphamide and etoposide as cytoreductive and immunosuppressive therapy. Bone Marrow Transplant 1991; 8: 489–495.
Kashyap A, Wingard J, Cagnoni P, Roy J, Tarantolo S, Hu W et al. Intravenous versus oral busulfan as part of a busulfan/cyclophosphamide preparative regimen for allogeneic hematopoietic stem cell transplantation: decreased incidence of hepatic venoocclusive disease (HVOD), HVOD-related mortality, and overall 100-day mortality. Biol Blood Marrow Transplant 2002; 8: 493–500.
Andersson BS, Thall PF, Madden T, Couriel D, Wang X, Tran HT et al. Busulfan systemic exposure relative to regimen-related toxicity and acute graft-versus-host disease: defining a therapeutic window for I.V. BuCy2 in chronic myelogenous leukemia. Biol Blood Marrow Transplant 2002; 8: 477–485.
Terenzi A, Aristei C, Aversa F, Perruccio K, Chionne F, Raymondi C et al. Efficacy of fludarabine as an immunosuppressor for bone marrow transplantation conditioning: preliminary results. Transplant Proc 1996; 28: 3101.
Chun HG, Leyland-Jones B, Cheson BD . Fludarabine phosphate: a synthetic purine antimetabolite with significant activity against lymphoid malignancies. J Clin Oncol 1991; 9: 175–188.
Keating MJ, O'Brien S, Lerner S, Koller C, Beran M, Robertson LE et al. Long-term follow-up of patients with chronic lymphocytic leukemia (CLL) receiving fludarabine regimens as initial therapy. Blood 1998; 92: 1165–1171.
Gandhi V, Plunkett W . Cellular and clinical pharmacology of fludarabine. Clin Pharmacokinet 2002; 41: 93–103.
Slavin S, Nagler A, Naparstek E, Kapelushnik Y, Aker M, Cividalli G et al. Nonmyeloablative stem cell transplantation and cell therapy as an alternative to conventional bone marrow transplantation with lethal cytoreduction for the treatment of malignant and nonmalignant hematologic diseases. Blood 1998; 91: 756–763.
Giralt S, Thall PF, Khouri I, Wang X, Braunschweig I, Ippolitti C et al. Melphalan and purine analog-containing preparative regimens: reduced-intensity conditioning for patients with hematologic malignancies undergoing allogeneic progenitor cell transplantation. Blood 2001; 97: 631–637.
Li L, Liu X, Glassman AB, Keating MJ, Stros M, Plunkett W et al. Fludarabine triphosphate inhibits nucleotide excision repair of cisplatin-induced DNA adducts in vitro. Cancer Res 1997; 57: 1487–1494.
Bornhauser M, Storer B, Slattery JT, Appelbaum FR, Deeg HJ, Hansen J et al. Conditioning with fludarabine and targeted busulfan for transplantation of allogeneic hematopoietic stem cells. Blood 2003; 102: 820–826.
Russell JA, Tran HT, Quinlan D, Chaudhry A, Duggan P, Brown C et al. Once-daily intravenous busulfan given with fludarabine as conditioning for allogeneic stem cell transplantation: study of pharmacokinetics and early clinical outcomes. Biol Blood Marrow Transplant 2002; 8: 468–476.
Chaudhry MA, Duggan P, Brown CB, Stewart D, Ruether FD, Glück S et al. Myeloablative chemotherapy for allogeneic transplantation with a fludarabine/busulfan protocol (Flubup): comparison with Bucy. Biol Blood Marrow Transplant 2000; 6: 140.
Russell JA, Chaudhry AM, Duggan P, Stewart D, Ruether D, Morris D et al. Daily intravenous busulfan (BU): Comparison with conventional oral BU in combination with fludarabine as conditioning for allogeneic stem cell transplant. Blood 2000; 96: 5188.
de Lima M, Couriel D, Thall PF, Wang X, Madden T, Jones R et al. Once-daily intravenous busulfan and fludarabine: clinical and pharmacokinetic results of a myeloablative, reduced-toxicity conditioning regimen for allogeneic stem cell transplantation in AML and MDS. Blood 2004; 104: 857–864.
Pavletic ZS, Bishop MR, Tarantolo SR, Martin-Algarra S, Bierman PJ, Vose JM et al. Hematopoietic recovery after allogeneic blood stem-cell transplantation compared with bone marrow transplantation in patients with hematologic malignancies. J Clin Oncol 1997; 15: 1608–1616.
Bensinger WI, Clift R, Martin P, Appelbaum FR, Demirer T, Gooley T et al. Allogeneic peripheral blood stem cell transplantation in patients with advanced hematologic malignancies: a retrospective comparison with marrow transplantation. Blood 1996; 88: 2794–2800.
Storb R, Deeg HJ, Pepe M, Appelbaum F, Anasetti C, Beatty P et al. Methotrexate and cyclosporine versus cyclosporine alone for prophylaxis of graft-versus-host disease in patients given HLA-identical marrow grafts for leukemia: long-term follow-up of a controlled trial. Blood 1989; 73: 1729–1734.
Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J et al. Consensus conference on acute GVHD grading. Bone Marrow Transplant 1995; 15: 825–828.
Common Toxicity Criteria Version 2.0. CTEP Cancer Therapy Evaluation Program [online]. 1999 April 30 [Cited 2006 April 12]; available from: http://ctep.cancer.gov.
Hughes WT, Armstrong D, Bodey GP, Bow EJ, Brown AE, Calandra T et al. 2002 Guidelines for the use of antimicrobial agents in neutropenic patients with cancer. Clin Infect Dis 2002; 34: 730–751.
Acknowledgements
This research has been supported by Hematology- Oncology and Bone Marrow Transplantation / Tehran University of Medical Sciences grant.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Iravani, M., Evazi, M., Mousavi, S. et al. Fludarabine and busulfan as a myeloablative conditioning regimen for allogeneic stem cell transplantation in high- and standard-risk leukemic patients. Bone Marrow Transplant 40, 105–110 (2007). https://doi.org/10.1038/sj.bmt.1705685
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705685
Keywords
This article is cited by
-
Double alkylators based conditioning reduced the relapse rate after allogeneic peripheral blood stem cell transplantation in adult patients with myeloid malignancies: a single arm phase II study
Bone Marrow Transplantation (2022)
-
Preconditioning with fludarabine, busulfan and cytarabine versus standard BuCy2 for patients with acute myeloid leukemia: a prospective, randomized phase II study
Bone Marrow Transplantation (2019)
-
Toxicity and efficacy of busulfan and fludarabine myeloablative conditioning for HLA-identical sibling allogeneic hematopoietic cell transplantation in AML and MDS
Bone Marrow Transplantation (2016)
-
Reduced-intensity conditioning with fludarabine and busulfan for allogeneic hematopoietic cell transplantation in elderly or infirm patients with advanced myeloid malignancies
Annals of Hematology (2016)
-
A modified busulfan and cyclophosphamide preparative regimen for allogeneic transplantation in myeloid malignancies
International Journal of Clinical Pharmacy (2015)
