
Abstract
OBJECTIVE: To assess the level of modification by local primary care doctors of key aspects of the National Asthma Education Program (NAEP) Guidelines for the Diagnosis and Management of Asthma.
DESIGN: A random sample of primary care physicians participating in local asthma guideline development.
SETTING: Two hospital systems, one based in an urban environment, and a second in a community and rural environment.
PARTICIPANTS: Primary care physicians.
INTERVENTION: Design of consensus-based local asthma guidelines using a modified Delphi approach.
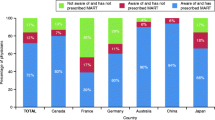
MEASUREMENTS AND MAIN RESULTS: A total of 42 physicians participated in the local guideline development. With few exceptions, the primary care physicians modified in major ways the NAEP Guidelines regarding the role of pulmonary function testing and spirometry. Specifically, the local guidelines did not require peak flow and spirometry measurements as the basis for initiating inhaled steroids as did the national guidelines. All 42 physicians emphasized a clinical diagnosis versus one based on a pulmonary function. Peak flow monitoring was recommended by 35 (83%) of physicians in selected patients only, in contrast to the national guidelines, which emphasized monitoring for all patients routinely and during exacerbations. There was strong agreement with the national guidelines on the role and importance of patient education, and on the indications for the use of inhaled steroids.
CONCLUSIONS: Disagreement by primary care doctors with parts of the NAEP guideline is a potential cause for poor compliance and lack of influence on patient care. Recognizing the need to modify or customize guidelines through field testing with local primary care physicians will improve acceptance of national guidelines.
Similar content being viewed by others

References
National Heart, Lung, and Blood Institute. Executive Summary: Guidelines for the Diagnosis and Management of Asthma. Bethesda, Md: U.S. Department of Health and Human Services; 1991. NIH publication 91-3042.
Hartert TV, Windom HH, Peebles S Jr, et al. Inadequate outpatient medical therapy for patients with asthma admitted to two urban hospitals. Am J Med. 1996;100:386–94.
Editors. NIH asthma treatment guidelines not being utilized in patient care. W V Med J. 1993;89:292.
Lewis LM, Lasater LC, Ruoff BE. Failure of a chest pain clinical policy to modify physician evaluation and management. Ann Emerg Med. 1995;25:9–14.
Brand DA, Newcomer LN, Freiburger A, Tian H. Cardiologists’ practices compared with practice guidelines: use of beta-blockade after acute myocardial infarction. J Am Coll Cardiol. 1995;26:1432–6.
Cline DM, Welch KJ, Cline LS, Brown CK. Physician compliance with advanced cardiac support guidelines. Ann Emer Med. 1995;25:52–7.
Browner WS, Baron RB, Solkowitx S, Adler LJ, Gullion DS. Physician management of hypercholesterolemia. A randomized trial of continuing medical education. West J Med. 1994;161:572–8.
Tunis S, Hayward RS, Wilson MC, et al. Internists’ attitudes about clinical practice guidelines. Ann Intern Med. 1994;120:956–64.
Audet AM, Greenfield S, Field M. Medical practice guidelines: current activities and future directions. Ann Intern Med. 1990;113:709–14.
Jones J, Hunter D. Consensus methods for medical and health services research. BMJ. 1995;311:376–80.
Fink A, Kosecoff J, Chassin M, Brook RH. Consensus methods: characteristics and guidelines for use. Am J Public Health. 1984;74:979–83.
Chassin MR, Kosecoff J, Solomon DH, Brook RH. How coronary angiography is used: clinical determinants of appropriateness. JAMA. 1987;258:2543–7.
Leape LL, Hilborne LH, Park RE, et al. The appropriateness of use of coronary artery bypass graft surgery in New York State. JAMA. 1993;269:753–60.
Emerman CL, Cydulka RK, Skobeloff E. Survey of asthma practice among emergency physicians. Chest. 1996;109:708–12.
Fried RA, Miller RS, Green LA, Sherrod P, Nutting PA. The use of objective measures of asthma severity in primary care: a report from ASPN. J Fam Pract. 1995;41:139–43.
Selker HP. Criteria for adoption on practice of medical practice guidelines. Am J Cardiol. 1993;71:339–41.
Kravitz RL, Greenfield S, Rogers W, et al. Differences in the mix of patients among medical specialties and systems of care. JAMA. 1992;267:1617–23.
Woolf SH. Paractice guidelines, a new reality in medicine, II: methods of developing guidelines. Arch Intern Med. 1992;152:946–52.
Diagnosis and treatment of idiopathic thrombocytopenic purpura: recommendations of the American Society of Hematology. The American Society of Hematoloy ITP Practice Guideline Panel. Ann Intern Med. 1997;126:319–26.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Picken, H.A., Greenfield, S., Teres, D. et al. Effect of local standards on the implementation of national guidelines for asthma. J GEN INTERN MED 13, 659–663 (1998). https://doi.org/10.1046/j.1525-1497.1998.00200.x
Issue Date:
DOI: https://doi.org/10.1046/j.1525-1497.1998.00200.x