
Abstract
Recommendations for seasonal influenza vaccination are standard in most developed countries. Many rapidly developing countries have recently begun to adopt recommendations for high-risk target groups, such as the elderly. Population-based surveys to determine use, rather than purchases, of seasonal influenza vaccine are rare outside North America and Western Europe. Such surveys can provide important information on the progress of national immunization programs and on the awareness of influenza among the general public. We report the results of a survey conducted in 10 countries in Africa, Asia Pacific, Eastern Europe, Latin America and the Middle East that aimed to determine influenza vaccination coverage among adults, the elderly, and children and to find out how influenza is perceived in these regions. Seasonal influenza vaccine coverage varied markedly across countries, and no single factor guaranteed high coverage. Our results indicate that strong recommendations appear insufficient, and that fully funded immunization programs together with high awareness in the population are key to encouraging high influenza vaccination coverage.
Similar content being viewed by others


Introduction
Seasonal influenza is a significant health problem worldwide, affecting approximately 10–20 per cent of the world population and contributing to more than 1 million deaths annually.1, 2, 3 Vaccination is the primary measure to reduce influenza-related mortality and morbidity in all age groups.4 Seasonal influenza vaccination, regardless of target group (elderly, healthy adults, or children), as has been documented, reduces disease burden and, beyond that, is associated with economic advantages.5, 6, 7, 8, 9, 10, 11, 12, 13, 14
Recommendations for influenza vaccination are a well-established component of national healthcare programs in almost all developed countries. Also, many rapidly developing countries are adopting recommendations for the immunization of high-risk target groups, such as the elderly or those with high-risk conditions.15 Globally, the World Health Organization (WHO) recommends seasonal influenza vaccination in preparation for an influenza pandemic.16 The WHO has also called for the development of tools to estimate the burden of seasonal and pandemic influenza and to monitor the progress of national influenza vaccination programs.17, 18 Such tools are needed to provide information on changes in vaccine usage and distribution patterns for use in forecasting future vaccine needs.
Macro-epidemiological studies of vaccine use (comparison of the use of influenza vaccine between different countries and regions rather than between different hospitals and physician groups) based on the number of doses of influenza vaccine purchased and distributed have proved an invaluable tool for measuring progress of national influenza awareness and vaccination programs.19 To assess adequately the effectiveness of immunization programs, additional coverage data by target group are needed. Population-based surveys can provide important complementary information on the level of vaccination coverage. Population-based studies of national influenza vaccination coverage rates (IVCRs) by target group are rare and, to our knowledge, such data have been published only for countries in North America20, 21 and Western Europe.22
Since 2003, we have conducted a series of population-based surveys to ascertain age group-specific seasonal IVCRs in several countries outside these two regions. Here we report the survey results for the period 2005–2006 in 10 countries: Argentina, Australia, Chile, China, Poland, Romania, South Africa, the Republic of Korea, Taiwan, and Turkey. We also evaluated awareness by region of influenza and perceptions of its severity in adults and children.
Methods
Survey population
A representative sample of the general population in 10 countries was interviewed: in China, Poland, Romania, the Republic of Korea, Taiwan, and Turkey in February and March 2006, following the 2005–2006 Northern Hemisphere influenza season; and in Australia, Argentina, Chile and South Africa from August to October 2006, following the 2006 Southern Hemisphere influenza season.
The interview process varied between countries, depending on available infrastructure. Interviewees were non-institutionalized individuals, aged 18 years or older, and selected by random probability procedures. Standard demographic characteristics (gender, age, education level, working and social status, income, living area, and community size) were recorded for each respondent. With the exception of China, Turkey and South Africa, both urban and rural areas were included. In China, the survey was restricted to accessible urban centers; in Turkey, and South Africa, rural populations were not included.
Except for China, Turkey, and South Africa, results were weighted and extrapolated to the global national population. The survey data from China were projected to be representative of the 350 million inhabitants living in the 60 largest cities in China. The survey data from Turkey and South Africa are applicable to the urban population only.
Information was gathered for three age groups: children (0–17 years), adults (18–64 years) and the elderly (⩾65 years), except in South Africa where children were excluded. Children were further categorized as infants and toddlers (0–3 years), young children (4–8 years) and older children (9–17 years). Information about children was obtained from parent interviewees, and the data were weighted to be representative of the national child population.
Questionnaire
Interviews were conducted either in person or by telephone using a standard questionnaire we developed and used since the 2003–2004 influenza season (available upon request).
Respondents were asked to rate the severity of influenza in relation to two other respiratory infections, the common cold and pneumonia, on a scale of 1–6 (1=mild disease, 6=life-threatening). Respondents who had children were asked to report whether they rated influenza in children as more, less, or equally severe compared with that in adults. They were also asked to rate the suitability of different population groups as targets for seasonal influenza vaccination on a scale of 1–4 (1=strongly disagree, 4=agree totally). These population groups were: children, the elderly, healthy adults, the working population, people working in close physical proximity (for example, those working in hospitals, nursing homes, schools), healthcare workers, people at increased risk of infection (for example, patients with asthma, diabetes, chronic cardiovascular diseases, chronic respiratory diseases) and travelers. Finally, respondents were asked if they were vaccinated against influenza during the previous influenza season. The same question was asked of parents about their children.
Classification of vaccination recommendations and immunization programs
Information on country-specific influenza recommendations and immunization programs was obtained from the appropriate government bodies (Table 1). Immunization programs were categorized as a ‘fully funded immunization program’ if vaccine was fully reimbursed or free of charge. National recommendations alone did not necessarily mean that immunization programs were in place.
Analysis
We used percentages to describe vaccination coverage rates: overall and by age group. Perceptions of influenza severity and suitability of vaccination target groups were calculated as mean values on the appropriate rating scale. Gross national income (GNI) data for 2005 were obtained from the world development indicators database of the World Bank.23 IVCRs were analyzed in relation to: national recommendations or funding, GNI, and general awareness regarding influenza and influenza vaccination.
Results
Demographic data
Overall 17 047 individuals were interviewed across the 10 countries, providing data on 17 047 adults and elderly people (aged ⩾18 years) and 7417 children (aged <18 years) (Table 2).
The governing bodies of all 10 countries issued recommendations for influenza vaccination, although target groups differed. Moreover, vaccination programs offering total reimbursement or free vaccinations were not equally available across these countries (Table 1). At the time of this study, all surveyed countries had national recommendations to vaccinate the elderly population, but only six had fully funded immunization programs: Australia, Argentina, Chile, Romania, Taiwan, and the Republic of Korea. In Turkey, a reimbursement policy for the elderly and at-risk adults and children was established in December 2005 (that is, very late in the 2005–2006 influenza season). For this study, Turkey was categorized as having only recommendations for vaccination. Only three countries had fully funded immunization programs for children: Chile, Taiwan, and Romania. Two more had issued national recommendations to vaccinate children: China and Republic of Korea. The five remaining countries did not target children.
Overall IVCRs by country
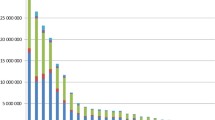
Coverage was highest in Korea (41 per cent), Australia (25 per cent) and Chile (25 per cent) and lowest in Turkey (5 per cent). In countries with fully funded immunization programs, the IVCRs ranged from 14 to 41 per cent, whereas without such programs, coverage rates were lower, around 10 per cent and below (Figure 1a).

Influenza vaccination coverage rates (IVCR) by country, by age group and in relation to the absence or presence of fully funded immunization programs for seasonal influenza. (a) Overall (all ages). (b) Adults and elderly. Data for five European countries (United Kingdom, UK; France, Fr; Italy, It; Germany, Ger; and Spain, Sp; 2004–2005 season) are reproduced from Muller and Szucs22 and the United States (2005–2006 season) from the CDC.20 *Interviewees from urban population only.
IVCRs among adults (18–64 years) and the elderly (>65 years)
Among the elderly, IVCRs were generally high in countries with fully funded immunization programs for the elderly (Argentina, Australia, Chile, Taiwan, Republic of Korea, and Romania), ranging from 10 per cent in Romania to 74 per cent in the Republic of Korea (average IVCR 48.8 per cent) (Figure 1b). In countries without such programs, but having national recommendations (China, Poland, South Africa, and Turkey), coverage rates were lower, ranging from 4 to 14 per cent (average IVCR 9.25 per cent).
Among adults, IVCRs were also generally higher in countries with fully funded immunization programs for the elderly, ranging from 7 per cent in Taiwan to 28 per cent in the Republic of Korea (average IVCR 16 per cent). In countries without such programs, adult coverage rates were lower, ranging from 4 to 13 per cent (average IVCR 5 per cent).
Pediatric IVCRs
Of the nine countries with survey data on children, Chile, Romania, and Taiwan had fully funded immunization programs for children (Table 2). A kindergarten and primary school-based vaccination policy was also in place in China, promoting influenza vaccination for attending children, and in the Republic of Korea recommendations for children encompassed ‘at-risk’ children and children aged 6–23 months (Table 2). Thus, in the five countries with at least recommendations for childhood vaccination (Chile, China, Republic of Korea, Romania, and Taiwan), IVCRs among children (0–17 years) were 23–62 per cent (Figure 2).

Influenza vaccination coverage rates (IVCR) in children by country and age group, in relation to the absence or presence of recommendations and/or fully funded pediatric immunization programs (no data available for South Africa). *Interviewees from urban population only.
In the countries with neither fully funded immunization programs nor recommendations for the vaccination of children (Australia, Argentina, Poland, and Turkey), coverage for children was low (8–10 per cent). No data were available for the seasonal influenza vaccination of children in South Africa for the season we assessed in this study.
Breaking these data down by age (0–3, 4–8, and 9–17 years) showed that the Republic of Korea consistently had the highest IVCRs among children, regardless of age group (50–83 per cent) (Figure 2). As expected, the average IVCR in the 0–3 year age group was higher (average 47.0 per cent, range 25–63 per cent) in countries with vaccination recommendations or fully funded immunization programs for 6–23-month-old children (Chile, the Republic of Korea, Romania, and Taiwan), than in countries (Argentina, Australia, China, Poland, and Turkey) without such recommendations or immunization programs (average 15.8 per cent, range 6–42 per cent). In addition, IVCRs among 4–8-year-olds were higher in Chile, the Republic of Korea, Romania, and Taiwan (44.3 per cent, range 25–83 per cent) than in Argentina, Australia, China, Poland, and Turkey (17.6 per cent, range 9–48 per cent) (Figure 2). IVCRs in children aged 9–17 years were generally less than 25 per cent, except for the Republic of Korea, where vaccination coverage in this age group was 50 per cent.
Perception and awareness of influenza
Awareness of influenza in countries without influenza immunization programs was poor. In South Africa and Turkey in 2005–2006, influenza was not distinguished in severity from the common cold. There was also little knowledge about target groups for vaccination in Poland, Turkey, and South Africa – countries without immunization programs. Children were not considered an important vaccination target by respondents in Australia, Argentina, Chile, and Turkey. The elderly were considered as legitimate vaccination targets in all countries, except Poland, Romania, and Turkey.
Overall, influenza was perceived as more severe in children than in adults, for example by 84 per cent of surveyed parents in the Republic of Korea, but also by 71 per cent of parents in Turkey and 40 per cent in Poland. These last two countries have no local recommendations or vaccination programs for influenza in children and comparatively low IVCRs for children.
IVCR in relation to GNI, income and educational level
There was no clear relationship between GNI per capita and overall IVCR. Countries with the highest GNI (Australia, Taiwan, and Republic of Korea) had relatively high IVCRs, but so did countries with the much lower GNIs (Chile, Argentina, and Romania) (Figure 3). Similarly, at an individual household level, income and educational attainment appeared to affect vaccine uptake in some countries, but there was no consistent or clear relationship (data not shown). In South Africa, China, Chile, Poland, and Australia, vaccination coverage among adults tended to increase with increasing income and educational level, whereas in Korean adults and Turkish elderly adults, lower income was associated with higher coverage.

Influenza vaccination coverage rates (IVCR) compared with gross national income for each country. *Interviewees from urban population only.
Discussion
There was considerable variation in seasonal influenza vaccination coverage across the 10 countries we investigated. Immunization programs funded nationwide and strong recommendations appeared to improve vaccination uptake in adults, the elderly, and children.
In the context of pandemic preparedness, the WHO has recommended in its Global Agenda on Influenza Surveillance and Control a worldwide IVCR target of at least 50 per cent of elderly people by 2006 and 75 per cent by 2010.4 In this survey (performed during 2005–2006), the WHO 2006 target was met by Australia, the Republic of Korea, and Chile, and the 2010 target was almost met by the Republic of Korea (74 per cent). Interestingly, vaccination coverage among the elderly in these three countries, which all have long-standing fully funded immunization programs for the elderly, was above or similar to that reported for the elderly in the United States in 2004 (65 per cent) and 2005–2006 (69.3 per cent).20, 24 It is difficult to explain the lower coverage in countries such as Romania, where fully funded immunization programs also exist for the elderly – possibly differences in health priorities, such as a bias towards children, or budget limitations. Notably, the lowest coverage among the elderly was reported principally from countries with national recommendations, but where no immunization program exists (South Africa, Turkey, Poland, and China). The evident lack of vaccination uptake in these four countries suggests that, as a public health measure, recommendations alone are insufficient. Only comprehensive, widely endorsed, government-funded programs can effectively achieve an increased coverage.
An overarching trend emerging from our survey was that the majority of countries appeared to be aligning their healthcare policies for the elderly with those of Europe and North America, in terms of funding influenza vaccination programs. This is not yet the case for children.
Pediatric influenza vaccination has the potential to reduce the impact of influenza epidemics25, 26 and a number of cost-effectiveness analyses have estimated substantial cost benefits associated with the vaccination of pre-school and school-age children, including a review by Savidan et al.27 Despite this evidence, few countries have established public immunization programs for children and, in our survey, IVCRs for children varied substantially between countries. Differences in health priorities or limitations of health budgets may explain restrictions in the use of influenza vaccine in young children. Again, and unsurprisingly, countries with strong recommendations or funded programs for children had the highest pediatric coverage rates. Conversely, pediatric coverage was low in the absence of national vaccination programs or recommendations. Among the youngest age group of children (0–3-year-olds), the highest levels of coverage were reported in the Republic of Korea, Taiwan, China, and Chile – likely the result of national guidelines, which recommend or stipulate vaccination for children aged 6–23 months, or, in the case of China, from the arrangement to vaccinate kindergarten attendees (which amounts de facto to an immunization program for young children).
Three countries in our survey with the highest coverage rates among children are in Asia, indicating the importance attached to pediatric vaccination in this region. Several factors may contribute to this, including first-hand experience with influenza A H5N1 outbreaks in poultry and wildfowl, particularly those associated with human fatalities. These have heightened awareness of seasonal influenza. Compared with other regions, increased influenza-related morbidity among children and increased rates of childhood hospitalization have been reported in Asia.28, 29 Local infrastructure for delivery of vaccine to children also plays a role: in China, immunizations are given to children while they attend kindergarten. In the Republic of Korea, although the vaccine has to be paid for, its administration by medical staff is free.
With public immunization programs for specific age groups, coverage not only increased in those groups, but seemed to increase coverage in the adjacent age groups. In three of the six countries with fully funded immunization programs for the elderly, adult IVCRs were markedly higher than in the countries without immunization programs for the elderly. Similarly, funded immunization programs or strong recommendations targeting 6–23-month-olds were associated with higher IVCRs in 4–8-year-olds.
Increased coverage in the age groups flanking a vaccination program target group may be explained in two ways: immunization programs, even if restricted to a narrow group, may encourage the medical community to recommend influenza vaccination more widely; such programs are likely to raise awareness about influenza in the general lay public. Indeed, the survey findings relating to how influenza was perceived indicate that funded immunization programs and strong governmental recommendations are associated with increased local knowledge and awareness of the severity of seasonal influenza. Countries with no immunization programs tended to have the lowest IVCRs and also poor influenza awareness.
Immunization programs appear to be the main driver of increased vaccination uptake. National wealth is one factor facilitating implementation of such programs. A direct correlation between vaccination coverage and GNI was, however, not observed. Other likely factors are health system maturity and awareness of the epidemiology of influenza, as well as that of other infectious disease competing for healthcare resources.
The overall coverage levels recorded in our survey are in broad agreement with previous reports. Korea had the highest IVCR, followed by Chile, Australia and Taiwan. These findings tally closely with the countries’ ranking in 2003 for the number of doses of influenza vaccine distributed per 1000 total population, with the Republic of Korea on top of the list (311 doses/1000 population), with Chile (126 doses/1000 population), Australia (214 doses/1000 population) and Taiwan (145 doses/1000 population).19 Coverage rates we observed for countries with fully funded immunization programs compared favorably with those reported in a population-based survey of over-14-year-olds across five European countries during the 2003–2004 influenza season, when 23 per cent of the study population received influenza vaccination.22 In the United States, a random-digit-dialed telephone survey revealed that for the 2005–2006 influenza season, the IVCR among people aged between 18 and 49 years with identified high-risk conditions was 30.5 per cent, and 18.3 per cent among those without risk factors.20 The IVCR among the elderly was 69.3 per cent, comparable to the results of our study.
Population-based studies, such as ours, provide important information on the number of vaccine doses that have been administered rather than simply purchased. As with all surveys, there are limitations. Survey methods may introduce a selection bias, as it is not possible to control for individuals refusing to be interviewed. Furthermore, data from hospitalized and institutionalized individuals are often not captured by nationwide surveys. Limitations specific to our survey include the lack of rural data from China, Turkey and South Africa. The data for China are projected to be representative of 350 million urban residents, capturing only the total urban population. Access to vaccination would be expected to be lower in rural areas; therefore, the coverage determined in this survey is likely to be an overestimate for China as a whole. Similarly for Turkey and South Africa, vaccination coverage estimated from our survey needs to be adjusted downwards to reflect the true level of vaccine coverage. The lack of child data is likely to affect the coverage rate for South Africa. Nonetheless, by employing different sampling methods across the 10 countries we endeavored to ensure that people were interviewed in a fashion best suited to local conditions, to optimize participation in the survey.
Conclusions
Global and age-specific seasonal influenza vaccine coverage rates varied markedly across the 10 countries studied, with higher rates generally observed in countries with ongoing recommendations or immunization programs. Differences observed in perception of seasonal influenza risks, about vaccination, and between national and age-related coverage rates may in part be attributable to disparities in economic and healthcare system maturity. The results of this study support the widespread adoption of vaccination programs and reimbursement schemes to bring the world closer to recent WHO objectives to increase IVCRs in countries and globally.
Disclaimer
All authors are employees of Sanofi Pasteur, a manufacturer of influenza vaccine. They declare no other conflicts of interest.
References
Pan American Health Organization (PAHO). (2004) Final Report of the XVI Meeting on Vaccine Preventable-Diseases of the Pan American Health Organization.
Stephenson, I. and Zambon, M. (2002) The epidemiology of influenza. Occupational Medicine (London) 52: 241–247.
Viboud, C., Alonso, W.J. and Simonsen, L. (2006) Influenza in tropical regions. PLoS Medicine 3: e89.
World Health Organization. (2005) Influenza vaccines. Weekly Epidemiological Record 80: 279–287.
Esposito, S. et al (2006) Clinical and economic impact of influenza vaccination on healthy children aged 2–5 years. Vaccine 24: 629–635.
Hui, S.L., Chu, L.W., Peiris, J.S., Chan, K.H., Chu, D. and Tsui, W. (2006) Immune response to influenza vaccination in community-dwelling Chinese elderly persons. Vaccine 24: 5371–5380.
Morales, A., Martinez, M.M., Tasset-Tisseau, A., Rey, E., Baron-Papillon, F. and Follet, A. (2004) Costs and benefits of influenza vaccination and work productivity in a Colombian company from the employer's perspective. Value Health 7: 433–441.
Nichol, K.L. and Goodman, M. (2002) Cost effectiveness of influenza vaccination for healthy persons between ages 65 and 74 years. Vaccine 20 (Suppl. 2): S21–S24.
Plun-Favreau, J., Tasset-Tisseau, A., Lundkvist, J., Jonsson, L., de la Llave, G. and Marty, A. (2004) Influenza vaccination of the at-risk adults and elderly: Measuring the long-term cost-effectiveness in an Argentinian managed care organization. International Congress Series 1263: 605–609.
Principi, N., Esposito, S., Marchisio, P., Gasparini, R. and Crovari, P. (2003) Socioeconomic impact of influenza on healthy children and their families. The Pediatric Infectious Disease Journal 22: S207–S210.
Samad, A.H. et al (2006) Workplace vaccination against influenza in Malaysia: Does the employer benefit? Journal of Occupational Health 48: 1–10.
Scuffham, P.A. and West, P.A. (2002) Economic evaluation of strategies for the control and management of influenza in Europe. Vaccine 20: 2562–2578.
Wang, C.S., Wang, S.T. and Chou, P. (2002) Efficacy and cost-effectiveness of influenza vaccination of the elderly in a densely populated and unvaccinated community. Vaccine 20: 2494–2499.
Wang, S.T., Lee, L.T., Chen, L.S. and Chen, T.H. (2005) Economic evaluation of vaccination against influenza in the elderly: An experience from a population-based influenza vaccination program in Taiwan. Vaccine 23: 1973–1980.
van Essen, G.A., Palache, A.M., Forleo, E. and Fedson, D.S. (2003) Influenza vaccination in 2000: Recommendations and vaccine use in 50 developed and rapidly developing countries. Vaccine 21: 1780–1785.
World Health Organization. (2005) Responding to the avian influenza pandemic threat: Recommended strategic actions. http://www.who.int/csr/resources/publications/influenza/WHO_CDS_CSR_GIP_05_8-EN.pdf.
World Health Organization. (2002) Adoption of the global agenda on influenza. Part II. Weekly Epidemiological Record 77: 179–182.
World Health Organization. (2005) WHO global influenza preparedness plan: The role of WHO and recommendations for national measures before and during pandemics. Accessed on 20 November 2008 at http://www.who.int/csr/resources/publications/influenza/GIP_2005_5Eweb.pdf.
The Macroepidemiology of Influenza Vaccination Study Group. (2005) The macro-epidemiology of influenza vaccination in 56 countries, 1997–2003. Vaccine 23: 5133–5143.
Centers for Disease Control and Prevention. (2007) State-specific influenza vaccination coverage among adults aged > or=18 years – United States, 2003–04 and 2005–06 influenza seasons. MMWR Morbidity and Mortality Weekly Report 56: 953–959.
National Advisory Committee on Immunization. (2007) Statement on influenza vaccination for the 2007–2008 season. An Advisory Committee Statement (ACS). Canadian Communicable Disease Report 33: 1–38.
Müller, D. and Szucs, T.D. (2007) Influenza vaccination coverage rates in 5 European countries: A population-based cross-sectional analysis of the seasons 02/03, 03/04 and 04/05. Infection 35: 308–319.
World Bank. World Development Indicators Database. http://web.worldbank.org/WBSITE/EXTERNAL/DATASTATISTICS/0,,contentMDK:20535285~menuPK:1192694~pagePK:64133150~piPK:64133175~theSitePK:239419,00.html, accessed December 2007.
Smith, N.M., Bresee, J.S., Shay, D.K., Uyeki, T.M., Cox, N.J. and Strikas, R.A. (2006) Prevention and control of influenza: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recommendations and Report 55 (RR-10): 1–42.
Jordan, R. et al (2006) Universal vaccination of children against influenza: Are there indirect benefits to the community? A systematic review of the evidence. Vaccine 24: 1047–1062.
Reichert, T.A., Sugaya, N., Fedson, D.S., Glezen, W.P., Simonsen, L. and Tashiro, M. (2001) The Japanese experience with vaccinating schoolchildren against influenza. New England Journal of Medicine 344: 889–896.
Savidan, E., Chevat, C. and Marsh, G. (forthcoming) Economic evidence of influenza vaccination in children. Health Policy, 86: 142–152. Available online 3 December 2007.
Chiu, S.S., Lau, Y.L., Chan, K.H., Wong, W.H. and Peiris, J.S. (2002) Influenza-related hospitalizations among children in Hong Kong. New England Journal of Medicine 347: 2097–2103.
Wong, C.M. et al (2006) Influenza-associated hospitalization in a subtropical city. PLoS Medicine 3: e121.
Acknowledgements
We would like to thank the representatives of the market research agencies who helped to collect the data reported here. We also thank Nathalia Rivas for her help in the data collection, and Grenville Marsh at Sanofi Pasteur for editing the manuscript.
Author information
Authors and Affiliations
Additional information
Can industrial world strategies to vaccinate annually be imported to lower income countries and, if so, what strategic elements ensure success?
Rights and permissions
About this article
Cite this article
de Lataillade, C., Auvergne, S. & Delannoy, I. 2005 and 2006 seasonal influenza vaccination coverage rates in 10 countries in Africa, Asia Pacific, Europe, Latin America and the Middle East. J Public Health Pol 30, 83–101 (2009). https://doi.org/10.1057/jphp.2008.40
Published:
Issue Date:
DOI: https://doi.org/10.1057/jphp.2008.40