Article Text

Abstract
Objective: To investigate the safety and efficacy of rituximab (RTX) in patients with refractory Wegener’s granulomatosis (WG).
Patients and methods: Eight consecutive patients with active refractory WG were included. In all patients disease activity had persisted despite standard treatment with cyclophosphamide and prednisolone, as well as tumour necrosis factor α blockade 3 months before inclusion in the study. Patients had particular granulomatous manifestations like retro-orbital granulomata (n = 5), nodules of the lungs (n = 1), and subglottic stenosis (n = 2). RTX was given intravenously every 4th week in combination with the standard treatment in five patients and with methotrexate in two others. Disease extent and activity were monitored clinically by interdisciplinary care, immunodiagnostics (ANCA serology, B cells by flow cytometry), and magnetic resonance imaging.
Results: Beneficial response and a reduction in disease activity were seen in three patients, two of whom went into complete remission. In three other patients, disease activity remained unchanged while the disease progressed in the remaining two patients. In all patients peripheral blood B cells fell to zero during treatment with RTX. cANCA titres remained unchanged in all except one patient.
Conclusion: In this pilot study, B lymphocyte depletion was not associated with a change of the ANCA titres or obvious clinical improvement of refractory granulomatous disease in patients with WG. Further studies are needed to evaluate the role of RTX in WG.
- ANCA, antineutrophil cytoplasmic antibody
- BVAS, Birmingham Vasculitis Activity Score
- CS, corticosteroids
- CYC, cyclophosphamide
- DEI, Disease Extent Index
- ELISA, enzyme linked immunosorbent assay
- MRI, magnetic resonance imaging
- TNFα, tumour necrosis factor α
- WG, Wegener’s granulomatosis
- Wegener’s granulomatosis
- B cells
- refractory
- rituximab
- granuloma
Statistics from Altmetric.com
- ANCA, antineutrophil cytoplasmic antibody
- BVAS, Birmingham Vasculitis Activity Score
- CS, corticosteroids
- CYC, cyclophosphamide
- DEI, Disease Extent Index
- ELISA, enzyme linked immunosorbent assay
- MRI, magnetic resonance imaging
- TNFα, tumour necrosis factor α
- WG, Wegener’s granulomatosis
Cyclophosphamide (CYC) and corticosteroids (CS) remain the preferred treatment for severe Wegener’s granulomatosis (WG), but there is some uncertainty about the rescue treatment in cases with persistent or refractory disease activity. With a better understanding of the pathogenesis of WG in the past decade, it has become possible to develop therapeutic strategies that use (biological) agents to target specific elements of the inflammatory response. Data from smaller pilot studies suggest that the addition of tumour necrosis factor α (TNFα) blocking agents like infliximab or etanercept to standard treatment, anti-CD4 antibody treatment or new agents like 15-desoxyspergualin may be successfully applied in refractory cases of WG.1–,3 Despite great efforts, most of the treatments are limited by infectious complications or the absence of a lasting response.4
The evidence for the role of antineutrophil cytoplasmic antibodies (ANCAs) in amplification of inflammatory signals in vitro has led to attempts to inhibit production of these antibodies, specifically. Rituximab (RTX), a chimeric monoclonal antibody that binds to CD20 expressed on the surface of B cells, leads to a B cell depletion by complement mediated activities and through antibody dependent cellular cytotoxicity.5 Preliminary results of the use of RTX in patients with ANCA associated vasculitides suggest that RTX-induced depletion of CD20+ B cells can inhibit ANCA production to some extent and induce disease remission.6,7 However, the results of a recent pilot study were somewhat biased by other concomitant treatments making it difficult to work out the effect of RTX in relation to other confounders.8
We report here our experience of an open label study of eight patients with WG who had mainly granulomatous manifestations refractory to standard treatment and TNFα blockade, which were subsequently treated with RTX according to a standardised protocol.
PATIENTS AND METHODS
Patients were followed up by an interdisciplinary approach in a single tertiary referral centre, as previously described.9 All patients fulfilled the definitions of the Chapel Hill Consensus Conference and of the American College of Rheumatology criteria for WG. ANCA against proteinase-3 tested positive in all patients. Clinical diagnosis was confirmed by the presence of characteristic histopathological features in all patients. Patients underwent a regular set of interdisciplinary clinical, serological, immunological examinations of disease activity and extent and for treatment related side effects, as reported earlier.9 Activity was assessed by the Birmingham Vasculitis Activity Score (BVAS), which has been validated for its use in WG, as outlined elsewhere.10 Disease extent was assessed by the Disease Extent Index (DEI), as described and validated by the authors.11 Remission was defined as a BVAS score that indicated the absence of signs of new or worse disease activity, and persistent disease activity for no more than one item. Relapse was defined as the recurrence or first appearance of at least one item on the BVAS score; if indicating a life or organ threatening dysfunction of a vital organ (lung, brain, eye, motor nerve, gut, or kidney) it was defined as a major relapse.
RTX (MabThera, F Hoffmann-La Roche Ltd) was applied in addition to standard treatment with cyclophosphamide (2 mg/kg every day by mouth or 15–20 mg/kg every 18–21 days) or methotrexate (0.3 mg/kg every week intravenously). RTX dosage was calculated by body surface area (375 mg/m2) and given intravenously every 4th week. Methylprednisolone (100 mg), clemastine as antihistamine prophylaxis, and a histamine receptor antagonist were applied additionally 30–60 minutes before RTX to prevent hypersensitivity and other reactions. During, and 120 minutes after, the infusion, patients were monitored on the intensive care unit. On the day before the first RTX infusion was given, a test dosage of 50 mg RTX in 50 ml NaCl 0.9% was given to test for an allergic reaction to the protein. Patients were followed up for a median of 18 months (range 6–28) after the last RTX infusion.
B lymphocytes were counted by flow cytometry (fluorescence activated cell sorting) and ANCA were determined by indirect immunofluorescence and direct enzyme linked immunosorbent assays (ELISAs) as earlier described.12
RESULTS
Patient characteristics
The major reason for escalation of treatment in five of the eight patients was a progress of retro-orbital granulomas documented by the ophthalmologist and magnetic resonance imaging (MRI) despite standard treatment with CYC and CS for a median of 16 months (range 6–48). In one patient (No 6), pulmonary granuloma and progressive granulomatous sinusitis with osseous destruction had developed during standard treatment. Two patients had subglottic stenoses and severe dyspnoea (Nos 7 and 8). Despite the addition of infliximab (5 mg/kg/month) to CYC and CS (n = 6), etanercept (25 mg twice a week subcutaneously) to methotrexate (n = 1) or mycophenolate mofetil (n = 1) for 3 months, granulomatous inflammation progressed in seven patients and persisted in one (No 5). Concomitant scleritis improved in one patient (No 4), but persisted in three others (No 1, 2, 5). In three patients bloody nasal discharge, considered as active disease on ear, nose, and throat examination, persisted. After insufficient response to standard treatment (median cumulative CYC dosage 76 g, range 6–163 g) and four pulses of infliximab, treatment was switched to RTX in all eight patients. While CYC was continued in five, treatment was switched to methotrexate in two and to mycophenolate mofetil in one other patient despite active disease. Reasons for not continuing CYC were haemorrhagic cystitis or a toxic bone marrow after CYC treatment. The dosage of CS was raised from a median of 10 mg to 32 mg in six patients and remained unchanged in two patients (table 1⇓).
Clinical characteristics of the study population at baseline
Outcome
All patients received four pulses of RTX (375 mg/m2) in 4-weekly intervals. Treatment was well tolerated by all patients. Figures 1A and B⇓ show the disease activity (BVAS) and disease extent (DEI) during the course of treatment. Four weeks after completion of the fourth RTX pulse, two patients were in remission (Nos 6 and 8), one in partial remission (No 3), three had unchanged disease activity (Nos 1, 4, and 5), while the disease had progressed further in the remaining two patients (Nos 2 and 7). Active scleritis persisted in patients Nos 2, 3 and 7. In three of the five patients with retro-orbital granulomas a further enlargement of the retro-orbital masses was documented by MRI, while the size remained unchanged in the two other patients (fig 2⇓). Progress of retro-orbital granuloma was associated with further visual impairment and decreasing eye motility in all of the three patients. Bloody nasal discharge considered as active disease on ear, nose, and throat examination persisted in three patients. Patient No 6 showed a beneficial clinical response to RTX and had decreased disease activity after the first two courses. Constitutional symptoms disappeared and granulomatous inflammation as well as cephalgia diminished. After completion of the fourth RTX course, no new or worse disease activity was detected and only a little inflammation of the sinus persisted. Dyspnoea and subglottic stenosis improved significantly in patient No 8, but the effect was not remarkable before the fourth RTX pulse.

(A) Disease activity score (BVAS) and (B) disease extent index (DEI) in the course of treatment with rituximab.

Magnetic resonance imaging of orbital granulomas (patient No 1) before (A, B) and after treatment (C, D) with RTX. In T2 weighted imaging (A, C), typical hypointense masses in both retrobulbar spaces (white arrows) are found, which are enlarged at follow up after 3 months. Contrast enhanced, fat suppressed, T1 weighted MRI sequences (B, D) show persistence of diffuse bright signals in the orbitae owing to granulomatous inflammation. In addition, extensive granulomatous processes in the ethmoidal cells are not improved after treatment.
In all patients peripheral blood lymphocyte counts became undetectable after RTX treatment (fig 3⇓). Titres of cANCA and ANCA-specific direct ELISA remained unchanged in all except two patients (fig 4⇓). The mean levels of C reactive protein decreased from 38 mg/l (25th and 75th centiles 16–82 mg/l) to 14 mg/l (25th and 75th centiles 6–28 mg/l), while the mean erythrocyte sedimentation rate dropped from 70 mm/1st h to 32 mm/1st h during the course. In comparison with the period before introducing RTX, CS dosage was decreased in three patients, was stable in one, and was increased in four other patients owing to active disease. Five patients refractory to RTX were afterwards successfully treated with azathioprine pulse therapy, as published recently.13 Two patients have been followed up for more than 1 year and the results have been promising.

Percentage of B cells in the course of treatment with rituximab.
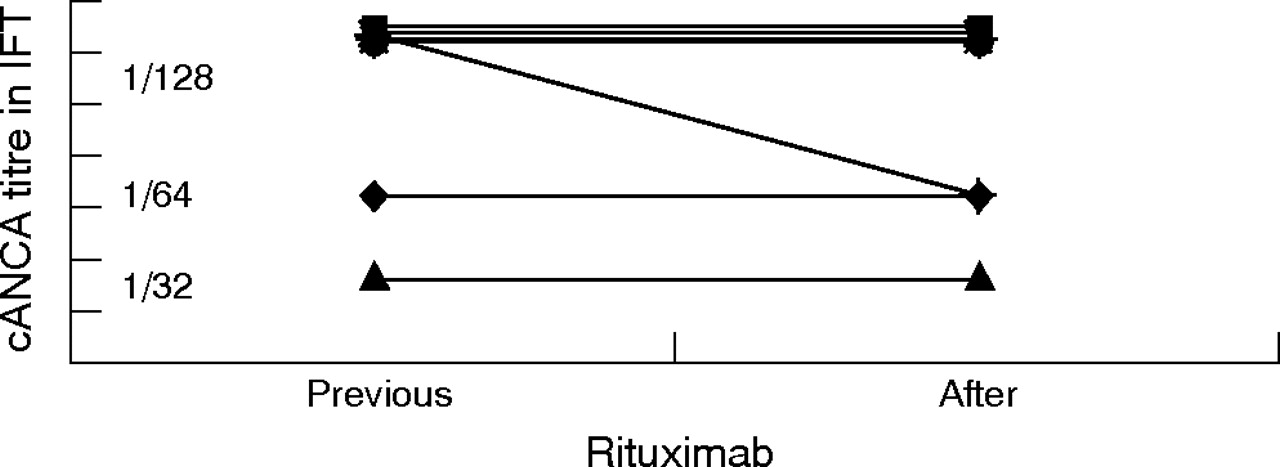
cANCA titres in the course of the treatment with rituximab.
DISCUSSION
We report on eight patients with WG refractory to standard treatment and TNFα blockade, of whom five also failed to respond to the treatment with RTX. In this pilot study, B lymphocyte depletion was not associated with a change of the ANCA titres or obvious clinical improvement of refractory granulomatous disease. Recently, and in contrast with the results presented here, the successful use of RTX in 11 patients with ANCA associated vasculitis (WG (n = 10), microscopic polyangiitis (n = 1)), who had either refractory disease or contraindication for the further use of CYC, has been reported.6 The results of the recent study suggest that B cell depletion by RTX leads to a decrease of cANCA titres and correlates directly with remission of the disease. Because of the varied concomitant immunosuppressive treatments, the possibility that the potential effect of RTX might have been influenced in the patients reported in the present study cannot be ruled out. But two major factors are more likely to account for the striking differences between the outcome in our study and the results in the cohort reported by Keogh and coworkers.
Firstly, it should be noted, that unlike other published series of refractory WG, the patients reported here had granulomatous manifestations which were more prominent than vasculitis or glomerulonephritis. In contrast, in the vast majority of patients reported by Keogh and coworkers, active organ involvement at the time of initiation of RTX treatment was mainly related to severe vasculitis (for example, alveolar haemorrhage) or glomerulonephritis.
The lack of response to CYC, infliximab, and RTX in the patients we reported suggests that patients with refractory granulomatous disease represent a subset of patients who are particularly difficult to treat and are likely to be pathogenetically different from the vast majority of patients with WG with predominantly vasculitic manifestations.
Granulomatous lesions in WG are made up of monocyte derived tissue macrophages, giant cells, neutrophils, CD4+CD28− T cells and B cells.14,15 Immunohistochemical studies have shown that those CD4+CD28− T cells appear to be the major source of interferon γ and TNFα secreted in the granulomatous lesions.16 CD4+CD28− T cells may be recruited into granulomatous lesions from the blood via CD18 interaction and may subsequently promote monocyte accumulation and granuloma formation through their cytokine secretion in WG. Additionally, we were able to prove follicle-like B lymphocytic infiltrates within the granulomatous lesions of endonasal specimens of patients with WG.17 The respective immunoglobulin-encoding genes indicated that these B cells are potential proteinase-3-ANCA producers. However, despite the local presence of CD20 positive B cell clusters within the granulomatous lesions of patients with untreated WG, there is as yet no direct evidence that B cells or ANCA play a pathogenic part in the granulomatous inflammation in WG; in a recently published animal model, local inflammation induced by intradermal injection of TNFα triggered a strong subcutaneous panniculitis in the presence of passively transferred systemic murine proteinase-3-ANCAs, but granulomatous inflammation was not seen.18
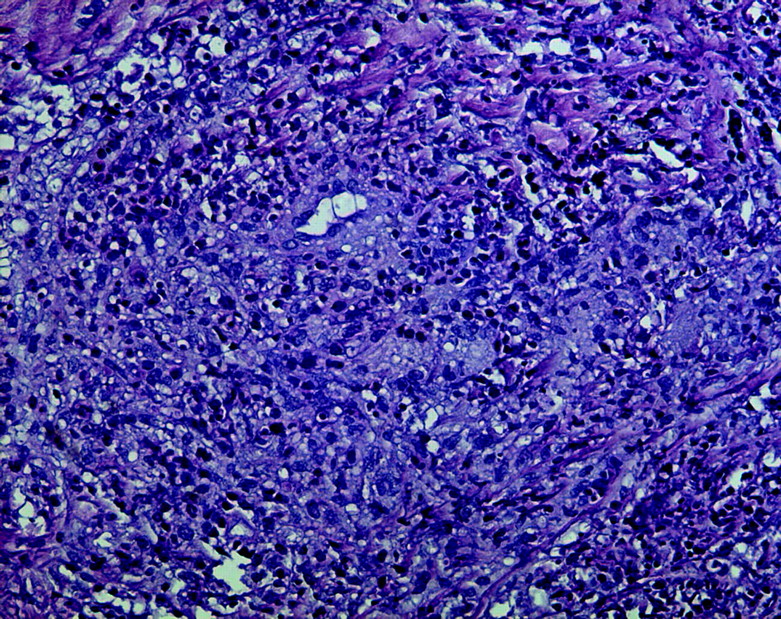
In our reported patients, it has to be assumed that the granulomata reflect a variable histopathological picture of inflammation, fibrinoid necrosis and, in particular, excessive fibrosis, but exceptional vasculitis.19 Fibrous tissue might replace areas of acute inflammation and necrosis in a healing response that temporarily exceeds the normal amount. In contrast with most granuloma found in other organ systems, the unusual amount of fibrosis might explain why granulomatous lesions of the orbita shrink to a certain extent during immunosuppressive treatment in some patients, but sometimes do not vanish entirely. Orbital socket contracture is a complication of inflammatory orbital disease and the excessive fibrosis.19 However, in the cases reported here, the new development or rapid increase of the circumference, as well as an obvious enhancement in the MRI scan, suggests a continuing active inflammatory process rather than predominant fibrosis. Additionally, a significant decrease of the granulomatous inflammation after changing to high dose azathioprine pulse therapy or desoxyspergualine in four patients who also did not respond to RTX, confirms a prevailing inflammatory process.13 One other patient who also did not respond to azathioprine pulse therapy had finally to be enucleated. The histological specimen of the enucleated eye and retro-orbital tissue showed a relevant retro-orbital active granulomatous inflammation in addition to a dense fibrosis, as was seen in other studies of patients with WG and inflammatory orbital disease.19 (fig 5⇓)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Retro-orbital granuloma (patient No 1 after treatment with RTX). Typically ill defined Wegener’s granuloma with multiple epithelioid cells centred around a capillary within a dense background of granulocytes, lymphocytes, and plasma cells (haematoxylin and eosin, ×200).
Secondly, the data presented here do not support the hypothesis that anti-CD20 mediated B cell blockade via RTX results in an effective suppression of ANCA production by plasma cells. As was seen in previous studies, peripheral B lymphocytes became undetectable in all our patients during treatment. However, ANCA titres remained mostly unchanged in our patients during and after treatment with RTX. Moreover, no correlation of the percentage of B cells and ANCA titre, and disease activity was found. Thus, the sustained or increased vasculitic manifestations in five of our patients might be a result of the unchanged ANCA titre despite peripheral B cell depletion. Careful analysis of the data reported by Keogh and coworkers raises additional concern about the potential of RTX to abolish ANCA production. In three of the five patients with WG presented by Keogh et al the ANCA titre did not become undetectable after re-treatment with RTX alone, suggesting that the previous decline of the ANCA titre in these and other patients might not solely be due to RTX, but rather be related to the simultaneously increase of GC (1 g methylprednisolone per day for 3 days) or concomitant plasma exchange. Persistence of ANCA production after one or more cycles of RTX might indicate an incomplete B cell depletion. Other reasons might be the persistence of long living plasma cells, that do not get harmed by RTX because of the lack of CD20 expression.20–,23 There is mounting evidence that long lived plasma cells with lifespans of months to years are an important source of autoantibody production in different autoimmune diseases.24,25 The existence of ANCA titres despite cytotoxic treatment in patients with WG and the persistence of normal immunoglobulin levels after treatment with RTX imply the existence of long lived plasma cells.26
The lack of efficacy of the previous treatment with infliximab in seven of our patients is in contrast with results from a previous pilot study, suggesting a beneficial effect in patients with refractory WG.1 The individually different responses to TNFα blockade and other treatments suggests the existence of pathogenically distinct disease subsets. The exceptional amount of fibrosis distinguishes retro-orbital granulomata from other granulomatous manifestations of WG and may significantly influence the response to treatment. Our data show that certain subsets (or disease stages) of WG are particularly difficult to treat, although the underlying differences of responders and non-responders have, for the most part, been not well defined in clinics, up to now.
In summary, the data presented here do not provide evidence that B cell depletion using RTX is sufficiently effective for the treatment of retro-orbital granulomata in WG that are refractory to standard treatment. In view of the small number of patients studied, our data do not exclude the possibility of a potentially beneficial effect on vasculitic manifestations or less aggressive disease courses as has been reported by others before. Thus, further studies are needed to assess the role of B cells in the pathogenesis of WG and the effect of RTX.
REFERENCES
Footnotes
Published Online First 3 November 2006