Article Text

Statistics from Altmetric.com
Description
A 34-year-old man with diabetes mellitus, but otherwise healthy and with no previous record of drug addiction, had two molars of the upper jaw removed. Three days later he developed a swelling and redness in his left temple and periorbital region. He was tender to palpation and not able to open his left eye (figure 1). His general condition was good with no fever, but C reactive protein was 301 when he was admitted to hospital 7 days after surgery. MRI scan showed an abscess located lateral to the alveolar crista of the upper jaw and upwards deep to the temporal fascia (figure 2). Eye functioning was unaffected and the MRI scan did not show any orbital involvement. The abscess was drained through a temporal incision, with excellent clinical and laboratory response. Microbiological samples showed Streptococcus milleri and Prevotella species, typical for an odontogenic abscess.

Redness and swelling periorbital and in the temple region. Only minor trismus and very modest symptoms from the jaw and oral cavity.

{kind=link}
{kind=link}
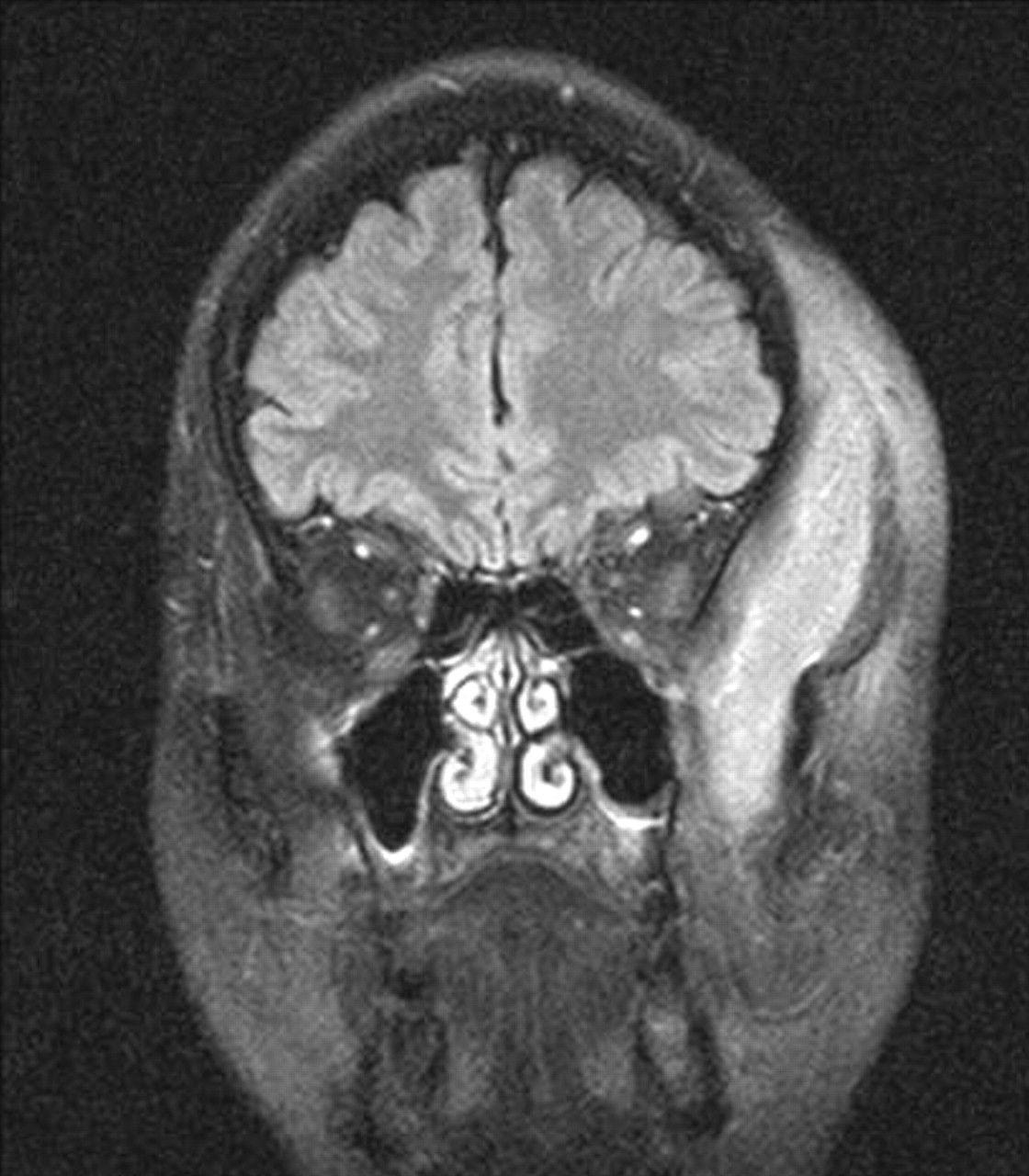
MRI scan showing an elongated abscess probably originating from the left side alveolar crista occupying a large space deep to the temporal fascia.
Even before admission to hospital he was treated with penicillin and metronidazole. Pending microbiological analyses, penicillin was substituted with cefotaxime for a short time.
Odontogenic infections may easily spread along muscles and fasciae,1 and may also cause parapharyngeal abscesses or pus accumulation deep to the cervical fasciae as, for example, Ludwig's angina. They can enter the masticatory space,2 but rarely invade tissue superior to this, as in this case. In this location, the origin of the abscess may be difficult to reveal. It may cause risk of thrombosis of the cavernous sinus and even jeopardise the orbit.3 Surgical drainage, elimination of infection focus, antibiotics and antithrombotic drugs is the treatment of choice.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.