Article Text

Statistics from Altmetric.com
Description
An 80-year-old diabetic and hypertensive lady was admitted with fever associated with chills and pain in the right hypochondrium of 5 days duration. On examination, she was febrile, drowsy and had asterixis. She was icteric and had tenderness with guarding in the right hypochondrium. There was no history of any pre-existing liver disease. Her haemoglobin was 9 g/dl, total leucocyte count was 11 700/mm3, platelets were 1.4 lac/mm3, total bilirubin of 3.3 mg/dl, albumin of 1.9 mg/dl, alkaline phosphatase – 227 U/l (normal 30–150 U/l), SGOT-327 U/l, SGPT-178 U/l and international normalised ratio (INR) was 2.1. Viral markers for A, B, C and E were negative. Ultrasonography showed a hypoechoic lesion in the right hepatic lobe. A CECT abdomen revealed a single 8×7 cm hypodense lesion in segments 5, 6, 7 and 8 with thrombosis of the right portal vein (figure 1A), normal left portal vein (figure 1B) with decreased enhancement of the right lobe and compressed retrohepatic inferior vena cava (IVC) (figure 2). Her serum indirect haemagglutination for Entamoeba histolytica had a titre of 1:2560 (significant titre >1:400) suggestive of an amoebic liver abscess (ALA) and was started on metronidazole. Anchovy sauce-like pus was aspirated (600 ml) from the abscess which did not grow any organism. She improved in terms of consciousness, inotrope requirements and INR (1.4) and bilirubin (1.8 mg/dl). She had started taking oral diet gradually, but had a large vomit following which she developed aspiration pneumonia, went into acute respiratory distress and succumbed.

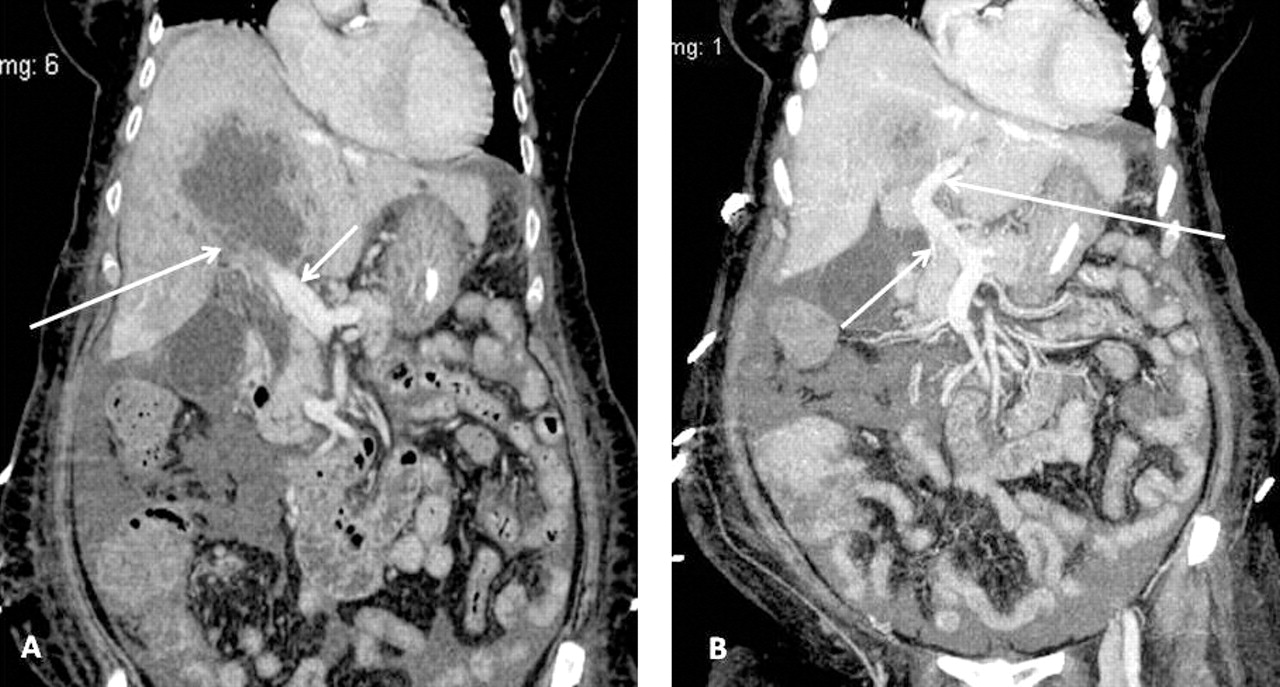
(A) Coronal section of CECT abdomen showing abscess in the segment 5, 6,7 and 8 of right lobe of the liver with thrombosis of the right portal vein (long arrow) with normal main portal vein (short arrow). (B) Coronal section of CECT of abdomen showing abscess cavity normal main portal vein (short arrow) and left portal vein (long arrow).

{kind=link}
{kind=link}
Coronal section of CECT of abdomen showing abscess cavity (short arrow) mainly in the right lobe of the liver with compressed IVC (long arrow).
Vascular complications with ALA have been described in the form of involvement of hepatic veins and IVC causing Budd–Chiari syndrome either by compression or thrombosis.1 2 Jaundice is uncommon and could be due to obstruction of biliary radicles,3 or as in this case was secondary to the liver failure. ALA presenting as liver failure is rare and is not because of hepatocyte dysfunction, but due to compromised blood flow either from portal vein, hepatic vein or IVC compression, as was seen in our patient. In literature, an autopsy series of 79 patients with ALA described portal vein thrombosis in 27% of patients.4 However, literature is scarce in the form of clinical case reports or imaging studies, documenting portal vein thrombosis in an ALA as a cause of liver failure.
Learning points
In a patient of ALA presenting with liver failure, vascular involvement should be suspected and CECT scan should be done, as it is the most sensitive investigation.
Patients with ALA and liver failure need to be treated on an emergency basis either by ultrasound-guided aspiration or open laparotomy and drainage depending on the clinical condition and the site of the abscess.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.