Article Text

Statistics from Altmetric.com
We describe three cases of bilateral adrenal masses with different aetiologies. Their clinical details are provided in table 1.
Clinical details

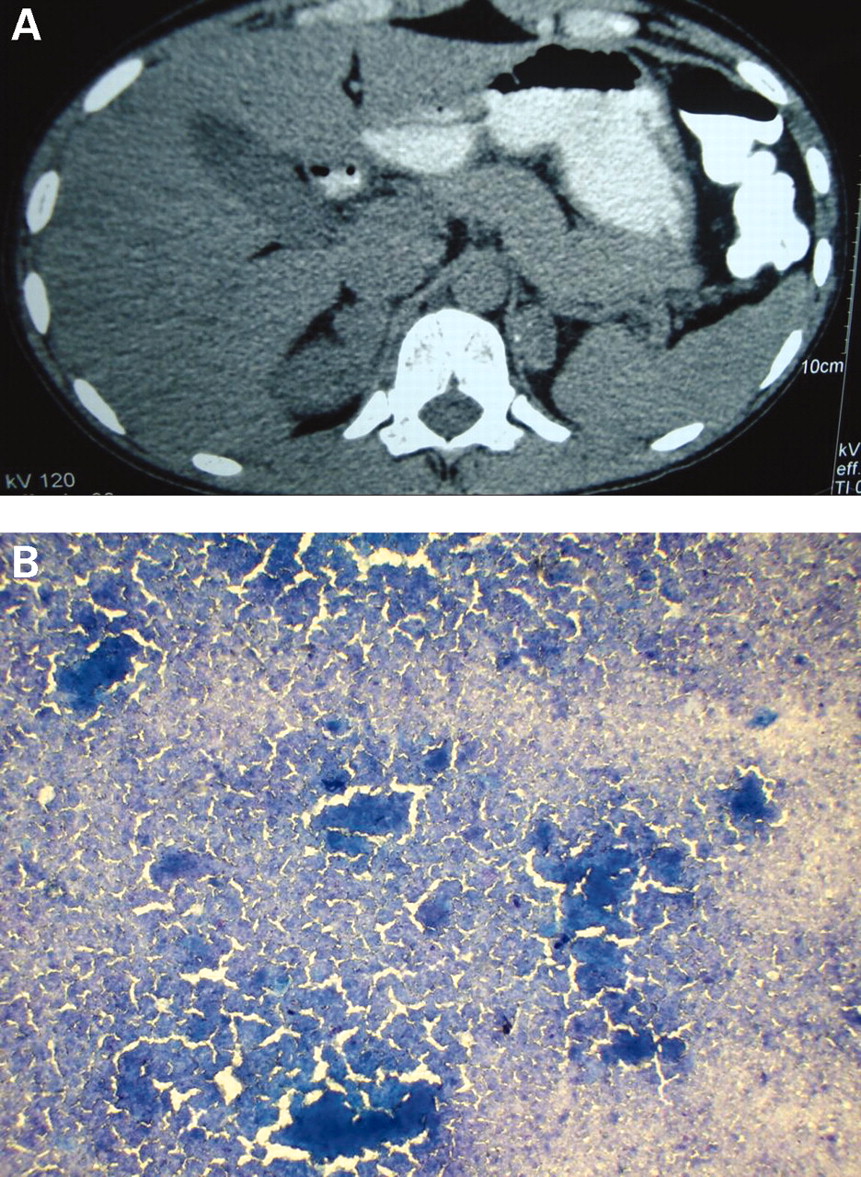
(A) Contrast enhanced abdominal computed tomography (CT) scan showing bilateral adrenal masses (right adrenal 4.4×2.2 cm and left adrenal 2.2×1.6 cm) with a speck of calcification. (B) Fine needle aspiration cytology smear showing granulomatous lesion consistent with tuberculosis; AFB stain is positive.

(A) Contrast enhanced abdominal CT scan showing bilateral adrenal masses (right adrenal 4.3×2 cm and left adrenal 4.9×3 cm); no lymphadenopathy. (B) Fine needle aspiration cytology smear showing periodic acid-Schiff (PAS) positive rounded structures consistent with histoplasmosis.

{kind=link}
{kind=link}
{kind=link}
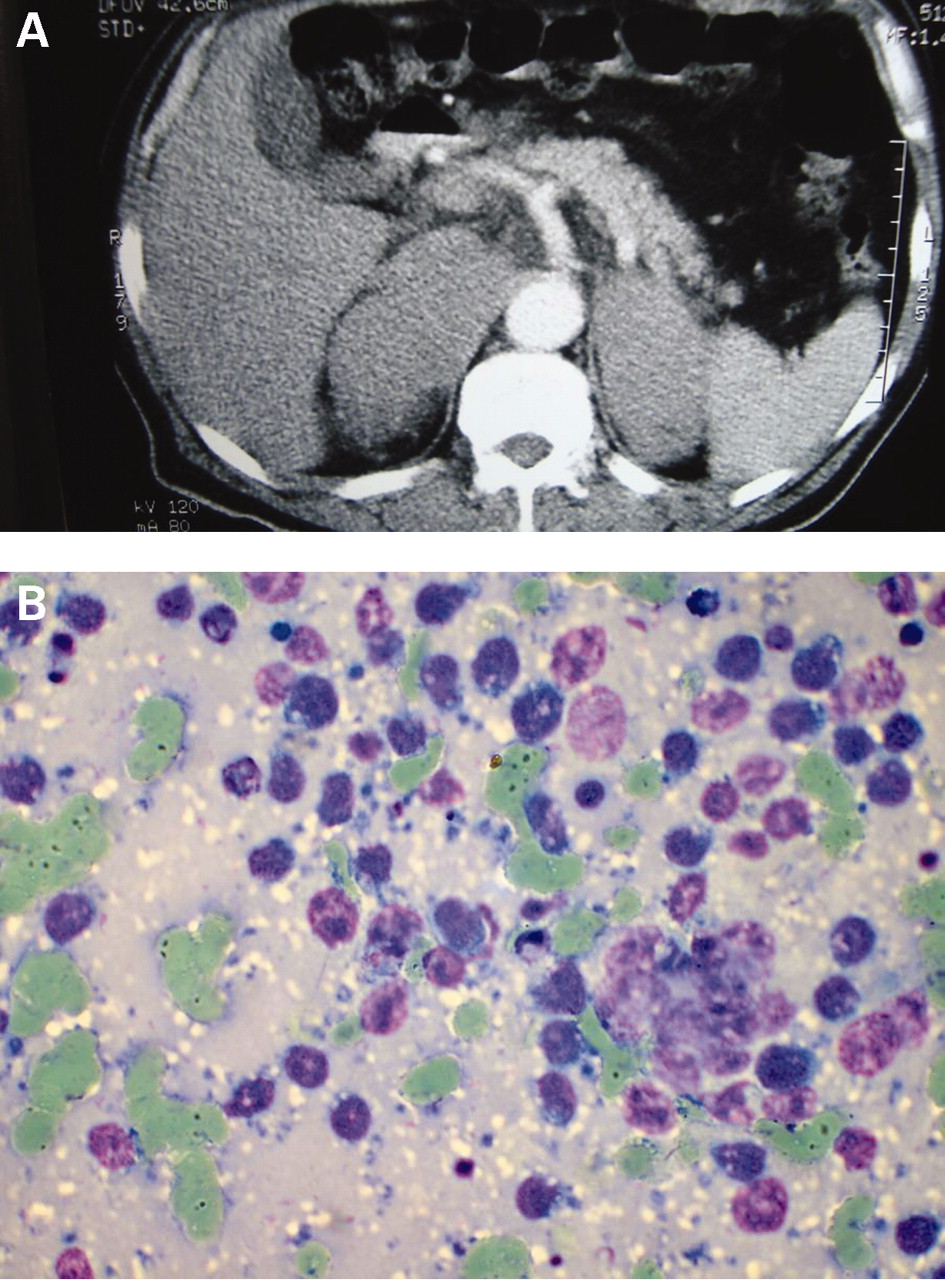
(A) Contrast enhanced abdominal CT scan showing bilateral adrenal masses (right adrenal 9.2×5 cm and left adrenal 7.5×4.9 cm) with periaortic lymphadenopathy. (B) Fine needle aspiration cytology smear showing discrete immature lymphoid cells with scanty vacuolated cytoplasm and mildly pleomorphic nuclei and fine nuclear chromatin. (May-Grunwald-Giemsa stain × 440)
The differential diagnosis of bilateral adrenal masses1 include infective aetiologies such as tuberculosis and histoplasmosis2; infiltrative disorders such as metastasis from an unknown primary, non-Hodgkin’s lymphoma3; amyloidosis and neoplasias such as bilateral pheochromocytoma and adrenocortical carcinoma. Rarely, longstanding untreated congenital adrenal hyperplasia and macronodular adrenal hyperplasia may also be associated with bilateral adrenal masses. Imaging is usually unrewarding for establishing the aetiological diagnosis, except for the presence of calcification which may point towards the diagnosis of tuberculosis or histoplasmosis. Fine needle aspiration cytology is useful in patients with bilateral adrenal masses, especially in the presence of adrenal insufficiency.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.