Article Text

Statistics from Altmetric.com
Description
A 23-year-old previously healthy male soldier presented with intermittent fever, generalised skin rashes, and a history of right earache for 11 days. He had recently performed military training on grass before his presentation. Initially, otitis media was diagnosed, but his earache did not improve after antibiotic treatment (amoxicillin/clavulanate, then imipenem/cilastatin sodium). The patient’s condition progressed to acute respiratory distress syndrome, and requirement for endotracheal intubation for respiratory failure. Physical examination revealed generalised morbiliform skin rashes, subconjunctival haemorrhage, but no eschar was found on the trunk, extremity, axilla, or groin area. Laboratory data showed elevated glutamic oxaloacetic transaminase/glutamic pyruvic transaminase (GOT/GPT) and thrombocytopenia. Otoscopic examination revealed an eschar lesion over the right external ear canal (figs 1 and 2). The proteus OX titre was 1:1280. Defervescence occurred in 24 h after intravenous minocycline administration, with gradual subsidence of the skin rashes. Scrub typhus was confirmed by the following serology data (IFA-IgG 1:640, IFA-IgM >1:160).
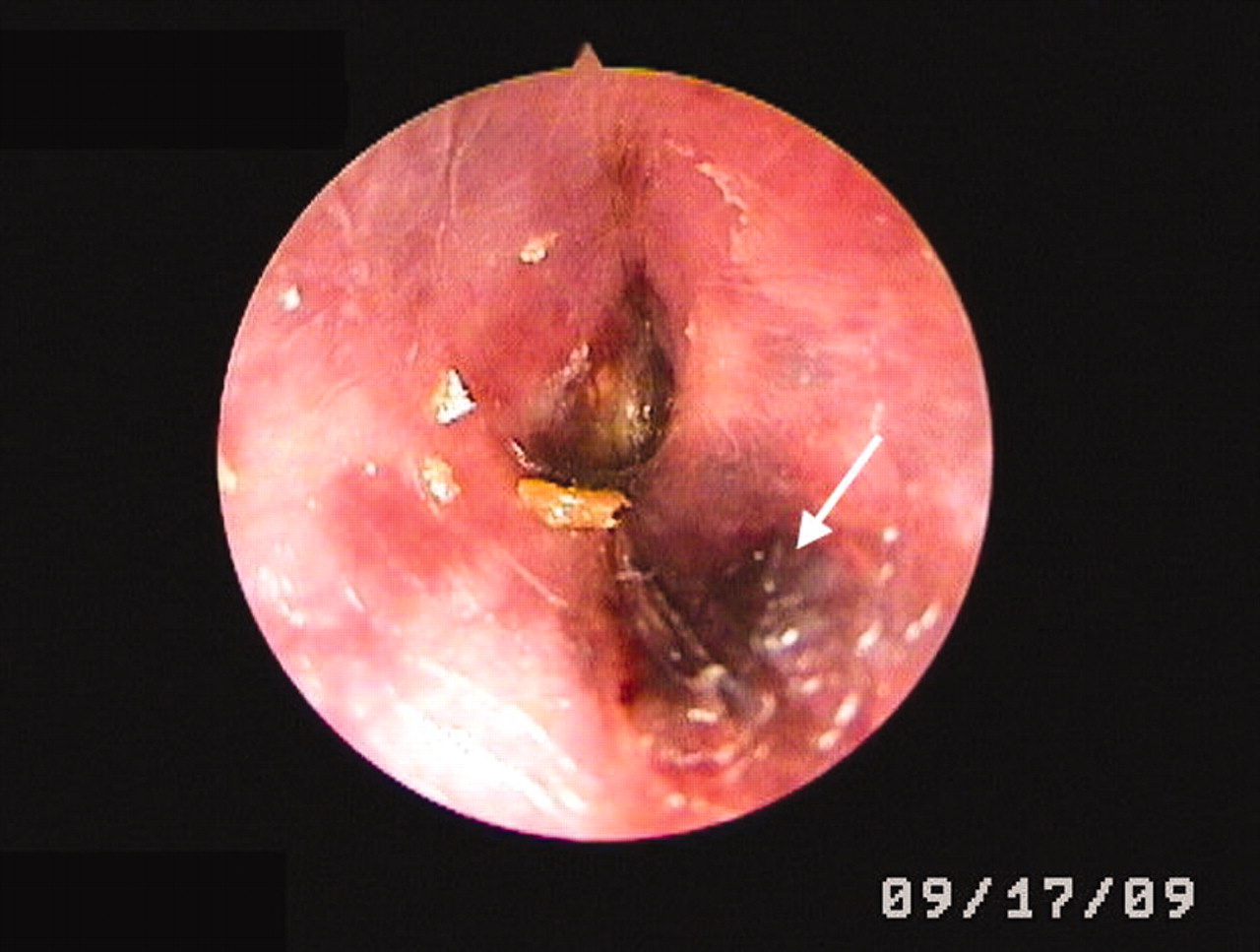
Arrow points to an eschar lesion on the external ear canal.

{kind=link}
{kind=link}
Otoscopic view shows eschar lesion.
Scrub typhus is an endemic disease, caused by Orientia tsutsugamushi. Typical presentations include fever, headache, eschar, rash, and lymphadenopathy.1 The black eschar is the most characteristic symptom and enables a quick diagnosis of this rickettsial disease. However, in a previous epidemiological analysis, only 23% of patients had this eschar lesion.1 Patients without the typical eschar may be misdiagnosed and progress to acute respiratory distress syndrome, disseminated intravascular coagulation, and septic shock.2 Thus, in an endemic area, the physician must check the whole of the patient’s body, including trunk, extremities, axilla, groin and other sites, such as the external ear canal in our patient, to find the mark left by this infectious mite.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.