Randomised controlled trial of homoeopathy versus placebo in perennial allergic rhinitis with overview of four trial seriesCommentary: Larger trials are needed
BMJ 2000; 321 doi: https://doi.org/10.1136/bmj.321.7259.471 (Published 19 August 2000) Cite this as: BMJ 2000;321:471
Abstract
Objective: To test the hypothesis that homoeopathy is a placebo by examining its effect in patients with allergic rhinitis and so contest the evidence from three previous trials in this series.
Design: Randomised, double blind, placebo controlled, parallel group, multicentre study.
Setting: Four general practices and a hospital ear, nose, and throat outpatient department.
Participants: 51 patients with perennial allergic rhinitis.
Intervention: Random assignment to an oral 30c homoeopathic preparation of principal inhalant allergen or to placebo.
Main outcome measures: Changes from baseline in nasal inspiratory peak flow and symptom visual analogue scale score over third and fourth weeks after randomisation.
Results: Fifty patients completed the study. The homoeopathy group had a significant objective improvement in nasal airflow compared with the placebo group (mean difference 19.8 l/min, 95% confidence interval 10.4 to 29.1, P=0.0001). Both groups reported improvement in symptoms, with patients taking homoeopathy reporting more improvement in all but one of the centres, which had more patients with aggravations. On average no significant difference between the groups was seen on visual analogue scale scores. Initial aggravations of rhinitis symptoms were more common with homoeopathy than placebo (7 (30%) v 2 (7%), P=0.04). Addition of these results to those of three previous trials (n=253) showed a mean symptom reduction on visual analogue scores of 28% (10.9 mm) for homoeopathy compared with 3% (1.1 mm) for placebo (95% confidence interval 4.2 to 15.4, P=0.0007).
Conclusion: The objective results reinforce earlier evidence that homoeopathic dilutions differ from placebo.
Randomised controlled trial of homoeopathy versus placebo in perennial allergic rhinitis with overview of four trial series
- Morag A Taylora, research associate,
- David Reilly (davidreilly1{at}compuserve.com)a, honorary senior lecturer in medicine,
- Robert H Llewellyn-Jonesb, lecturer,
- Charles McSharryc, principal immunologist,
- Tom C Aitchisond, senior lecturer in statistics
- a University Department of Medicine, Glasgow Royal Infirmary, Glasgow G31 2ER
- b Department of Psychological Medicine, University of Sydney, New South Wales 2006, Australia
- c University Department of Immunology, Western Infirmary, Glasgow G11 6NT
- d Department of Statistics, University of Glasgow, Glasgow G12 8QQ
- a Department of Primary Health Care, Institute of Health Sciences, Oxford OX3 7LF
- b Integrative Medicine Service, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10021, USA
- Correspondence to: D Reilly, Academic Departments, Glasgow Homoeopathic Hospital, Glasgow G12 0XQ
- Accepted 25 April 2000
Abstract
Objective: To test the hypothesis that homoeopathy is a placebo by examining its effect in patients with allergic rhinitis and so contest the evidence from three previous trials in this series.
Design: Randomised, double blind, placebo controlled, parallel group, multicentre study.
Setting: Four general practices and a hospital ear, nose, and throat outpatient department.
Participants: 51 patients with perennial allergic rhinitis.
Intervention: Random assignment to an oral 30c homoeopathic preparation of principal inhalant allergen or to placebo.
Main outcome measures: Changes from baseline in nasal inspiratory peak flow and symptom visual analogue scale score over third and fourth weeks after randomisation.
Results: Fifty patients completed the study. The homoeopathy group had a significant objective improvement in nasal airflow compared with the placebo group (mean difference 19.8 l/min, 95% confidence interval 10.4 to 29.1, P=0.0001). Both groups reported improvement in symptoms, with patients taking homoeopathy reporting more improvement in all but one of the centres, which had more patients with aggravations. On average no significant difference between the groups was seen on visual analogue scale scores. Initial aggravations of rhinitis symptoms were more common with homoeopathy than placebo (7 (30%) v 2 (7%), P=0.04). Addition of these results to those of three previous trials (n=253) showed a mean symptom reduction on visual analogue scores of 28% (10.9 mm) for homoeopathy compared with 3% (1.1 mm) for placebo (95% confidence interval 4.2 to 15.4, P=0.0007).
Conclusion: The objective results reinforce earlier evidence that homoeopathic dilutions differ from placebo.
Introduction
Do homoeopathic serial dilutions, containing no molecules of the original substance from which they were prepared, show intrinsic therapeutic effect? This trial, the fourth in a series, was designed in response to a challenge from an independent clinical team to contest the evidence from the three preceding trials that homoeopathic dilutions seem to differ from placebo.1-3 These were not trials of treatments; they were designed to address the placebo hypothesis, using allergy as a model. In this study, as before, patients with atopic inhalant allergies received, randomly and double blind, either an oral 30c homoeopathic preparation of their principal allergen or a placebo. The previous trials studied effects in atopic patients with hay fever 1 2 and asthma,3 whereas this study focused on perennial allergic rhinitis. We report the results of this fourth trial and an overview of the series.
Participants and methods
Volunteers were recruited in London from four general practices and the ear, nose, and throat outpatient department of Northwick Park Hospital. The prescribers were familiar with homoeopathic principles but were not experienced in homoeopathic immunotherapy. All patients gave written informed consent, and the trial was approved by Hillingdon and Harrow Health Authorities' ethics committees.
Patients meeting the admission criteria (box) were screened for symptoms and compliance during a two week qualification period.6 Although drugs for rhinitis were stopped two weeks before entry, patients could use them during the trial if required, and asthma drugs were not altered. No new allergen avoidance measures were permitted during the trial.
Criteria for eligibility
Inclusion
Age >16 years
Atopic: reactive to inhaled allergens with positive skin test results
More than 1 year history of perennial rhinitis4
Exclusion
Deterioration during grass pollen season
Nasal abnormalities causing obstruction
Previous homoeopathic immunotherapy for perennial rhinitis
Allergen avoidance in past 6 weeks
Away from usual environment for more than 1 week during trial
Respiratory infection
Severe concomitant disease
Pregnancy, breast feeding, or likelihood of pregnancy
Oral or parenteral steroids in past 6 months5
Conventional desensitisation in past 3 months
Washout periods
Long acting antihistamines in past 4 weeks
Topical steroids, cromoglycate, vasoconstrictors, or antihistamines in past 2 weeks
Trial design
The trial was a randomised, double blind, placebo controlled study of two parallel groups (fig 1). Crossover was precluded because of possible carry over effects from homoeopathy. We recruited participants over six weeks from the middle of February so that the prospectively defined stopping time was before the start of the local pollen season.

Recruitment of patients and their progress through the trial
{kind=link}
At the start of the qualification period the doctor assessed each patient's history, allergy status, and nasal obstruction. The principal allergen determining the prescription was then chosen on the basis of the largest skin test weal concordant with the allergy history. In seven cases in which the prescriber had difficulty in determining the principal allergen, telephone advice was given by a doctor experienced in prescribing homoeopathic immunotherapy. The first of three phials of placebo corresponding to the principal allergen was then administered by the doctor on to the patient's tongue. Patients were unaware that the phials contained placebo, although the researchers were not blinded.
The following two weeks served jointly as the qualification and baseline period. At the second visit, qualifying patients were randomised by a restricted technique of permuted blocks of two,7 generated from random number tables and stratified for the indicated allergen. A double blinded prescription was immediately dispensed. The trial ended with a follow up visit four weeks later.
Allergy and respiratory tests
Operators were trained to test sensitivity to house dust mite, cat fur, dog hair, tree pollens, grass pollens, and cladosporium by skin prick testing with preloaded lancets (Phazets, Pharmacia, Milton Keynes) and to aspergillus, feathers, and house dust using a needle and allergen solution (Bencard, Welwyn Garden City). Negative and positive histamine controls were used. A weal reaction of 3 mm or more in its greatest diameter after 15 minutes was taken as positive. To confirm the diagnosis, allergen specific serum IgE was measured by radioimmunoassay according to the manufacturer's instructions (Pharmacia). Samples were tested in batches to avoid interassay variability.
Patients were taught to use a Youlten nasal inspiratory peak flow meter (Clement Clark, Harlow),8 which is an objective, sensitive, valid, and reliable indicator of nasal obstruction.9-12 This measure decreases after nasal challenge in allergic rhinitis. 11 13 In clinical trials increases of 13 l/min after low dose desensitisation14 and 18.5 l/min after topical steroids15 have been correlated with clinical improvements.
Study diaries
At the same time each morning and evening patients recorded three successive nasal inspiratory peak flow measurements. Before making these measurements patients oriented themselves by noting each morning (on a 0 to 4 integer scale) how their symptoms had interfered with their sleep and, each night, rating blocked, runny, or itchy nose symptoms, sneezing, and any eye and chest symptoms. Patients then recorded their daily overall visual analogue scale score. To allow comparison with our previous trials1-3 the identical wording was used: “Overall today I felt …” on a scale of 0–100 mm, where 0 is fine and 100 is terrible. Visual analogue scale scores are a recommended measure of the severity of rhinitis.16 Adverse events, including initial aggravations of symptoms as observed in our previous rhinitis trial,2 were documented by the patients, clarified by the doctor, and recorded on standard adverse experience report forms. Any use of conventional drugs was also noted.
Medication preparation and administration
Using original standard allergen material from the Pasteur Institute in Paris, a homoeopathic laboratory (Boiron, Lyons, France) prepared the drugs according to the French homoeopathic pharmacopoeia through 30 stages of 1 in 99 serial agitated dilutions to produce a 30c dilution, as reported previously.3 Each treatment consisted of three identical phials containing 1 g of lactose-sucrose globules that had been impregnated with either a 30c homoeopathic dilution of the principal allergen or placebo. The three phials constituted a split single dose that was to be taken equally spaced over 24 hours to cover any diurnal variation in the patient's sensitivity to treatment and to ensure compliance. Only one dose was taken. The placebo dilution consisted of the same batch of diluent identically diluted and vibrated but without the starting allergen. The treatments were indistinguishable in packaging, taste, and smell. Random samples of drug phials were checked by independent laboratories for the presence of extraneous house dust mite allergen (der p1) by enzyme linked immunosorbent assay (ELISA)17 (University of Virginia, Charlottesville) and for antiallergy drugs by gas chromatography-mass spectrometry (MD800, Fisons, Manchester). No such contamination was found.
The coded drug packages were sent to the pharmacy department of Glasgow Royal Infirmary where, to augment blinding, each one was recoded with a unique number according to the randomisation schedule and then delivered to the pharmacy department of Northwick Park Hospital for distribution to each centre. The codes were held by both the French laboratory and a hussier de justice (notary) and remained unbroken until the analyses were completed.
Analysis
The prestudy power calculation was based on the results of the hay fever trial,2 from which a mean difference of 15 mm between the groups on visual analogue scale scores and a corresponding standard deviation of 29 were obtained. With a choice of 5% significance and 80% power, we estimated that 60 patients would be required in each group to avoid false negative results. No interim analysis was carried out. The predefined main measures of outcome were the changes from baseline in mean visual analogue scale scores and nasal inspiratory peak flow (use of mean values supported by Wihl and Malm18) over the third and fourth weeks after randomisation, when initial aggravations would be likely to be over and any treatment effects evident. Predefined secondary measures of outcome were differences between the groups in reports of adverse events, including initial aggravations of symptoms and use of drugs for rhinitis. Intention to treat analysis was used. Variables with normal distributions (nasal inspiratory peak flow and visual analogue scale) were analysed by using two tailed, two sample t tests and confidence intervals. χ2 tests were applied to categorical comparisons and proportions, but if any cell in a contingency table was less than 5, Fisher's exact test was used. The independent statistician verified the coded data entry, confirmed all analyses, and then carried out a repeated measures analysis of covariance on the changes from baseline over the four weeks after randomisation for each variable. The possible terms for inclusion in the model were treatment, time into study, and treatment-time interaction; the baseline score was included as a potential covariate.
Overview
To summarise our results, the original data19 from all four trials were pooled and analysed by an independent worker using Cochrane Collaboration meta-analysis software (Revman 3.0). All available visual analogue scale scores from every randomised patient in the four trials were used on an intention to treat basis, with each patient acting as his or her own control. The four trials had been designed as a series to address the hypothesis that homoeopathy is a placebo response. Each trial studied atopic inhalant allergies and assessed subjective effects in the same way over the third and fourth weeks after randomisation. They had also all used homoeopathic immunotherapy at 30c potency. The studies should therefore have a good degree of clinical homogeneity. Statistical heterogeneity was assumed to be present when the P value for heterogeneity was less than 0.10, and therefore the random effects model was used.20 The weighted mean difference was used as an estimate of the treatment effect (average change on homoeopathy minus average change on placebo).21 To aid presentation the overall daily graph was plotted with smoothed values by using simple robust non-linear procedures.22 As the main objective measure varied across the studies we compared them in a simple overview.
Results
Participants
Fifty one patients successfully completed qualification screening and were randomised (fig 1). Because of the exacting screening, strict qualification criteria, and the prospectively defined requirement to stop enrolment before the pollen season, we did not recruit the number of patients that the power calculation had estimated we required.
At baseline, clinical characteristics (table 1) and main measures of outcome (table 2) were similar in both groups. One patient (homoeopathy group) was subsequently lost to follow up despite repeated postal reminders.
Baseline clinical characteristics of study participants. Values are numbers (percentages) of participants unless stated otherwise

Mean (SE) weekly change from baseline in nasal inspiratory peak flow
{kind=link}
Baseline scores and mean change from baseline over third and fourth week after randomisation for subjective and objective measures of severity of rhinitis
Nasal inspiratory peak flow
We found a clear objective difference between the effects of placebo and homoeopathy on nasal airflow (table 2, fig 2). Patients in the homoeopathy group had an overall improvement from baseline averaging 21% compared with 2% in the placebo group over the third and fourth weeks after randomisation. This difference was significant (P=0.0001) and was confirmed by repeated measures analysis of covariance. The improvement was consistent across all recruitment centres.
Visual analogue scale
Subjectively, both treatments resulted in improvement, with no significant difference between them (table 2). This change began during the single blind placebo run-in period, decreasing the baseline value by the time of randomisation. Subsequently both groups showed further improvement. The individual symptom scores echoed these trends. Centre by centre analysis showed that in all but one of the centres the homoeopathy group improved more than the placebo group. This anomalous result seemed to be related to the increased frequency of aggravations and later entry in that centre.
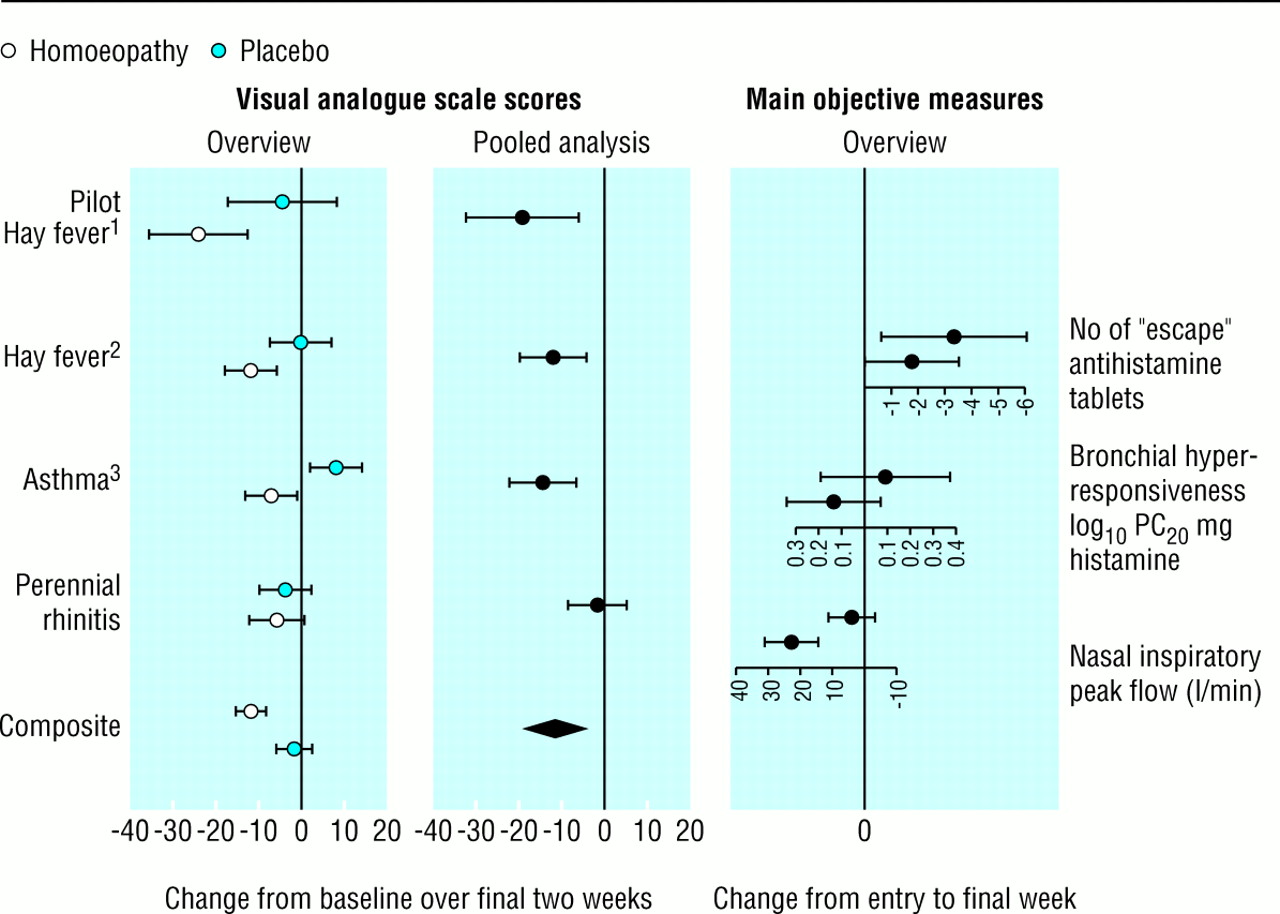
Overview and pooled analysis of four trials of homoeopathic immunotherapy
{kind=link}
Other measures
Non-respiratory adverse events were minor, and no difference was found between the groups. Initial aggravations of rhinitis symptoms were provoked more by homoeopathy than by placebo. By 48 hours after randomisation seven (29%) patients in the homoeopathy group reported a worsening of rhinitis, two with wheeze, compared with two (7%) patients in the placebo group, neither of whom had wheezing (P=0.04, Fisher's exact test). By 14 days, 11 (46%) patients in the homoeopathy group had reported adverse events, 10 of whom had rhinitis related aggravations, compared with seven (26%) in the placebo group, five of whom had rhinitis related aggravations (χ2=3.28, P=0.07). In general, most aggravations were short lived, averaging four days, and all had resolved by day 16. Aggravations of rhinitis in patients who received homoeopathy seemed to point to a good outcome. Initial deterioration was followed by subjective improvement and a corresponding improvement in nasal inspiratory peak flow. Only one patient in each group resorted to conventional rhinitis drugs, and both took them for less than four days.
Overview
Figure 3 compares the underlying patterns from the four trials based on daily visual analogue scale data from all 253 randomised patients and the main objective measures. The subjective changes measured by the visual analogue scale show a therapeutic response from homoeopathy across the four trials. There was a lesser and more variable response in the placebo groups, which probably accounts for the evidence of some statistical heterogeneity (χ2=9.04, df=3, P=0.03). The pooled estimate of the treatment effect (middle column, fig 3) showed an average improvement in visual analogue scores in the homoeopathy group compared with the placebo group (improvement 11.1 mm, 95% confidence interval 3.3 to 18.8; P<0.01). Thus, overall, the trend of the individual trial results and pooled data point towards homoeopathy differing from placebo. The trends in the objective measures all follow the same direction as the subjective measures (fig 3), again indicating a difference between a homoeopathic dilution and placebo.
Figure 4 shows the average response to homoeopathic immunotherapy over time in the four trials. A distinct separation emerges between the action of homoeopathy and placebo. On average, over the last two weeks after randomisation, patients who received homoeopathy had a 28% improvement compared with 3% among those in the placebo group. There was a mean reduction of the visual analogue scale score of 10.9 mm in the homoeopathy group compared with 1.1 mm in the placebo group (95% confidence interval for difference 4.2 to 15.4, P=0.0007; two sided, two sample t test).
Discussion
We found that homoeopathy and placebo had different effects. Compared with placebo, homoeopathy provoked a clear, significant, and clinically relevant improvement in nasal inspiratory peak flow, similar to that found with topical steroids.15 However, the subjective improvement was less clear. Although the objective measure consistently improved in all five centres, the subjective results were better than placebo in only four of the five centres and overall there was no difference between the groups. If the objective results are valid the discrepancy in the subjective measurements may be partly due to under recruitment compounded by aggravations and possible initial placebo responses during the run-in period in both groups, perhaps reflecting the positive expectations of the participants.23 Patients with rhinitis are keen to enter studies in their quest for better symptom control.24 Subjective improvement began before the end of the placebo run-in phase in both groups, and this lessened the chance of distinguishing between the groups. 25 26 A larger sample size may have shown a subjective difference between the groups.

Effect of homoeopathic immunotherapy and placebo on visual analogue scale scores averaged over four trials
{kind=link}
More initial aggravations occurred in patients who received homoeopathy, and this may have further complicated the subjective results. The pattern of temporary worsening followed by improvement, seen in this trial and observed in clinical homoeopathy for over 200 years, 27 28 is not typical of placebo.
Validity of results
Like any other therapy, homoeopathy requires rigorous scientific testing, and one study is insufficient evidence. Some perspective may be gleaned by viewing the results of this trial in the context of the series of which it is part. Except for the subjective measure in this fourth trial, the subjective and objective results show a trend across these four trials clearly pointing to homoeopathy being different from placebo. If the results were due to chance then some trends in favour of placebo would be expected. So does homoeopathy work or are our results due to some other factor?
Recent attempts to resolve the controversy surrounding homoeopathy have centred on the 180 or so controlled trials to date. A criteria based review in 1991 found that the evidence was positive but not conclusive.29 In a 1997 update, other workers concluded that 73% of the existing trial data supported homoeopathy being more effective than placebo, with the pooled odds ratio from a criteria based meta-analysis of 89 trials suggesting homoeopathy showed around twice the overall mean effect of placebo. The difference was significant and proved robust in sensitivity analyses that included correction for publication bias.30 A third working group, independently set up by the European Commission, selected 17 comparisons in 2001 patients for a meta-analysis. The pooled P value was highly significant, and the group commented that “it is likely that among the tested homeopathic approaches some had an added effect over nothing or placebo.”31 Are these findings “meta-errors” or, however implausible, does something tangible lie at the core of homoeopathy?
To interpret these findings as arguing for homoeopathy having an effect may now be more plausible than our previous hypothesis of serial false positive results. 3 32 For now, we conclude that this study has failed to confirm our original hypothesis that homoeopathy is a placebo.
What is already known on this topic
Much scepticism exists about the effectiveness of extreme homoeopathic dilutions
Several trials have suggested that homoeopathic dilutions have more effect than placebo
What this study adds
Patients with allergic rhinitis who received homoeopathy had significantly better nasal air flow than those in the placebo group
More patients in the homoeopathic group had initial symptom aggravations
Overall, no difference was seen in subjective measurements on a visual analogue scale, with both groups showing improvement
When the results are combined with those of three similar studies, homeopathy is different from placebo on both subjective and objective measures
Acknowledgments
We thank the patients who took part in the study, their doctors (Janet Gray, Ian Isaac, John Porterfield) and R Auerbach of Northwick Park Hospital, London, for ear, nose, and throat assessment. We thank Laboratoires Boiron for preparing the drugs, Angela Mahoney for help with randomisation, Neil Beattie for prescription advice, Peter Langhorne for independent pooled analysis, Andrew Jenkins for computer programming and graphics, and J H McKillop for his support. We also thank S McIntosh of the Institute of Biochemistry, Glasgow Royal Infirmary, for screening for anti-asthma drugs and T G Merrett of the Allergy Analysis Centre, Gwynedd, Wales, for screening for house dust mite antigen.
Contributors: MAT was project manager, participated in the design, and conducted most of the analysis. DR conceptualised and developed this series of trials and was involved in the design and analysis of this trial. RHL-J instigated this trial, acted as clinical coordinator while working in London, and contributed to design and analysis. CMcS participated in the design and carried out immunological analysis. TCA advised on the design of the project and implemented further independent analysis. The paper was written mainly by MAT and DR with important contributions from the other authors. MAT and DR are guarantors.
Footnotes
Funding Fondation Française pour la Recherche en Homeopathie, Blackie Foundation Trust, British Homoeopathic Association, and Scottish Homoeopathic Research and Education Trust. The project was initially part of a research fellowship created by the Research Council for Complementary Medicine in partnership with the Medical Research Council and the King's Fund.
Competing interests MAT's salary was partly paid by the Blackie Foundation Trust, British Homoeopathic Association, and Scottish Homoeopathic Research and Education Trust administered by Glasgow University. She was reimbursed for attending a symposium organised by the Blackie Foundation Trust. DR began this research programme before using homoeopathy or developing education. He uses homoeopathy in clinical care. He accepts occasional lecture and teaching fees but has no consultancy work. He has declined all direct industry grants for research and has used intermediary regulatory organisations to ensure independence.
References
Commentary: Larger trials are needed
- Tim Lancaster, clinical reader in general practice (tim.Lancaster{at}public-health.oxford.ac.uk)a,
- Andrew Vickers, assistant attending research methodologistb
- a University Department of Medicine, Glasgow Royal Infirmary, Glasgow G31 2ER
- b Department of Psychological Medicine, University of Sydney, New South Wales 2006, Australia
- c University Department of Immunology, Western Infirmary, Glasgow G11 6NT
- d Department of Statistics, University of Glasgow, Glasgow G12 8QQ
- a Department of Primary Health Care, Institute of Health Sciences, Oxford OX3 7LF
- b Integrative Medicine Service, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10021, USA
- Correspondence to: T Lancaster
High quality randomised trials are welcome in the evaluation of homoeopathy, as in other branches of health care. The methods used by Reilly and colleagues in their study of homoeopathy for perennial allergic rhinitis were rigorous, and it is unlikely that their results arose from methodological bias.
Are they correct to argue that they have reinforced the evidence that homoeopathy is more than a placebo? The current trial is the fourth in which this group evaluated a similar treatment, comparator, patient group, and outcome measure. As with the previous studies, the primary outcome used to calculate the sample size was a visual analogue score measuring patients' perceived improvement in symptoms. In contrast to the earlier studies, they detected no effect of homoeopathic treatment on the visual analogue score. These data do not strengthen the conclusion that homoeopathy differs from placebo. In fact, the effect of including the current study in their meta-analysis with data from the three earlier trials is to weaken (though not overturn) this conclusion.
The authors report a significant effect of homoeopathy on a second outcome measure, the nasal peak inspiratory flow. This result, like that of the meta-analysis, is challenging to those who believe that homoeopathy is always equivalent to placebo. However, it is difficult to place this finding in the context of the previous studies as they did not measure this outcome.
Clinical trials are particularly important in homoeopathy as they are nearly the only evidence that treatment can have effects different from placebo. Unlike many medical interventions, there are no established animal models, mechanisms of action, or examples of similar treatments of proved benefit. Moreover, homoeopathy is biologically implausible because of the use of medicines diluted beyond the Avogadro limit. It is therefore reasonable to ask for a high level of randomised evidence before concluding that homoeopathy exerts specific effects. A meta-analysis based on all the controlled trials identified by a systematic search showed a modest effect of homoeopathy over placebo.1 Because of the relatively small number of patients studied, neither the positive nor the negative result of the current study would shift this estimate significantly. To move the scientific debate forward, homoeopathic research needs trials with the power to detect or effectively refute the moderate effects suggested by the meta-analysis. Others have shown that such trials are feasible in homoeopathy. 2 3 The new challenge for Reilly and colleagues is to do the large trials that really could change thinking.
Footnotes
Competing interests None declared.