Article Text

Abstract
Objectives In this study we aimed to analyse the structure and content of telephone consultations of final-year medical students in a high-fidelity emergency medicine simulation. The purpose was to identify any areas of deficiency within structure and content in the effective transfer of clinical information via the telephone of final-year medical students.
Design An educational study.
Setting Simulation centre in a medical school.
Participants 113 final-year medical students.
Primary and secondary outcomes The primary outcome was to analyse the structure and content of telephone consultations of final-year medical students in a high-fidelity emergency medicine simulation. The secondary outcome was to identify any areas of deficiency within structure and content in the effective transfer of clinical information via the telephone of final-year medical students.
Results During phone calls to a senior colleague 30% of students did not positively identify themselves, 29% did not identify their role, 32% did not positively identify the recipient of the phone call, 59% failed to positively identify the patient, 49% did not read back the recommendations of their senior colleague and 97% did not write down the recommendations of their senior colleague.
Conclusions We identified a deficiency in our students skills to communicate relevant information via the telephone, particularly failure to repeat back and write down instructions. We suggest that this reflects a paucity of opportunities to practice this skill in context during the undergraduate years. The assumption that this skill will be acquired following qualification constitutes a latent error within the healthcare system. The function of undergraduate medical education is to produce graduates who are fit for purpose at the point of graduation.
- Medical Education & Training
- Communication
- Simulation
- Patient Safety
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Effective and accurate communication is fundamental to high-quality healthcare.
-
Communication of relevant clinical information during telephone calls.
-
An analysis of the content and structure of final-year medical students’ telephone consultations during simulation.
Key messages
-
Of our students, 49% did not read back the recommendations of their senior colleague and 97% did not write down the recommendations of their senior colleague following a telephone consultation.
-
The assumption that this will be acquired following qualification constitutes a latent error within the healthcare system.
Strengths and limitations of this study
-
All 113 final-year medical students took part in a high-fidelity emergency medicine simulation.
-
The videos of the simulations where later analysed using an agreed metric.
-
It was the student's first experience of high-fidelity emergency medicine simulation, under observation by faculty; our metric may have missed out on important aspects of the structure and content of telephone consultations.
Introduction
Accurate, reliable communication of task-relevant information across shift changes is a core component of handover.1 Effective and accurate communication in handover is fundamental to facilitate high-quality healthcare.2 Ineffective handover can lead to wrong treatment, delays in medical diagnosis, life-threatening adverse events, patient complaints, increased healthcare expenditure, increased hospital length of stay and a range of other effects that impact on the health system.3–5 One study identified that errors occurred at a consistent rate of 3.5% during the communication of urgent laboratory results via telephone across three hospital locations, with physicians having the highest error rate of 5% when compared with nurses 3.4% and clerical staff 3.5%.6
Communication between clinical colleagues has become a focus of inquiry and research, given further impetus by the Joint Commission reporting in 2007 that communication was a factor in over 60% of their sample of Sentinel events.7
Leonard et al8 developed the Situation, Background, Assessment, Recommendation (SBAR) approach to interprofessional communication by adapting the USA nuclear submarine fleet communication protocol ‘situation background assessment and resolution’, replacing ‘resolution’ with ‘recommendation’ in their (SBAR) model. The decision to do so was an accommodation to the differing safety cultures of the two organisations. The submarine fleet insists on decisions being affirmed following team discussion, healthcare allows recommendation from a variety of sources, though focusing accountability to a single practitioner.9
Bhabra et al10 in an experimental study of information transfer using surgical registrars compared the clinical information attrition in a succession of handovers. The authors reported ‘After five handover cycles, only 2.5% of patient information was retained using the verbal-only handover method, 85.5% was retained when using the verbal with note taking method and 99% was retained when a printed hand-out containing all patient information was used’. The Joint Commission set ‘Readback’ as a patient safety goal in 2009, albeit with variable implementation.11
Context
The use of high-fidelity simulation within medical education is gaining an increasing profile as a means by which the clinical practice skills of undergraduates and postgraduates can be acquired and evaluated in a low-risk environment. In their recent report reviewing both undergraduate and postgraduate medical education in the UK the General Medical Council stated: ‘It is increasingly unacceptable for medical students and trainees to practice skills and procedures on patients without prior simulated experience’.12 Likewise, the UK's Department of Health's 2011 document ‘A framework for technology enhanced learning’ in its first recommendation states ‘As part of a managed learning process and where appropriate, healthcare professionals should learn skills in a simulation environment and using other technologies before undertaking them in supervised clinical practice’.13
Simulation has been defined as ‘a technique, not a technology, to replace or amplify real experiences with guided experiences, often immersive in nature, that evoke or replicate substantial aspects of the real world in a fully interactive fashion. 'Immersive’ conveys the sense that participants have of being immersed in a task or setting as they would if it were the real world’.14 Simulation gives the learner the opportunity to experience a learning environment that is immersive and experiential. Continuous practice involving medical simulations is linked with better-quality learner outcomes and this relates to diverse levels of learners from a broad spectrum of clinical specialties. It appears to deliver a dose–response relationship in terms of accomplishing desired learning outcomes.15
Although much medical consultation is conducted over the telephone, relatively little research has been conducted into how best we can prepare our undergraduates for this important skill in their role as a hospital doctor.16 One of the fundamental structures for enhancing safe practice is the successful transfer of clinical information between individuals. Accurate information transfer between individuals is dependent upon them both sharing the same mental model for information transfer.17 In their review of the handover mnemonics literature Riesenberg et al show that SBAR was the most frequently cited mnemonic (69.6%). The review identified among others lack of training as a significant contributor to communication errors.18
In this study we aimed to analyse the structure and content of telephone consultations of final-year medical students in a high-fidelity emergency medicine simulation. The purpose was to identify any areas of deficiency within structure and content in the effective transfer of clinical information via the telephone of final-year medical students.
Method
All 113 final-year medical students took part in a new curricular development of high-fidelity emergency medicine simulation in a purpose built high-fidelity simulator using a METi Human Patient Simulator mannequin in the ASSET Centre located within our medical school. Twelve scenarios based on real-life cases were designed by faculty, and students had access to the types of scenarios electronically beforehand. During a variety of clinical scenarios a senior intensive care nurse, a member of the simulation team, assisted students. Prior to the simulation the students are given a detailed orientation of the simulator. They are also advised that during all scenarios they may use the telephone to seek the advice of a senior colleague (registrar) on patient management. Participants were briefed to adopt the role of a Junior Doctor (intern, F1) and to refer to themselves with this title during any conversations with the patient, other professionals or senior medical staff. Students were advised during orientation that they would receive feedback from faculty on all aspects of their performance including communication during debrief after each scenario. Faculty observed students from within the control room. If students became distressed during the simulation and wished to withdraw they could indicate this by removing their white coat. Throughout the previous 4 years of the regular curriculum all students received instruction in communication skills including communication via the telephone.
The students’ performances including telephone calls were recorded using the installed audio-visual system in the simulation centre for use in debrief. The telephone calls were later analysed using an agreed metric. Only telephone calls to the senior colleague were included in analysis and only those of sufficient duration for the student to be able to disclose and seek all relevant information from a senior colleague (registrar). PH, DP, SDS reviewed the first 20 videos jointly achieving a consensus on each factor before moving on to the next item, the remaining 49 were analysed by PH. Data from the telephone calls were entered jointly by PH and DP into Statistical Package for the Social Sciences and analysed for frequencies of a student completing or omitting an item of the metric. An item of the metric was allocated as a failure if a student omitted to complete that item. All the participating students provided written consent and the Clinical Research Committee of the Cork Teaching Hospitals granted ethical approval for this study.
Results
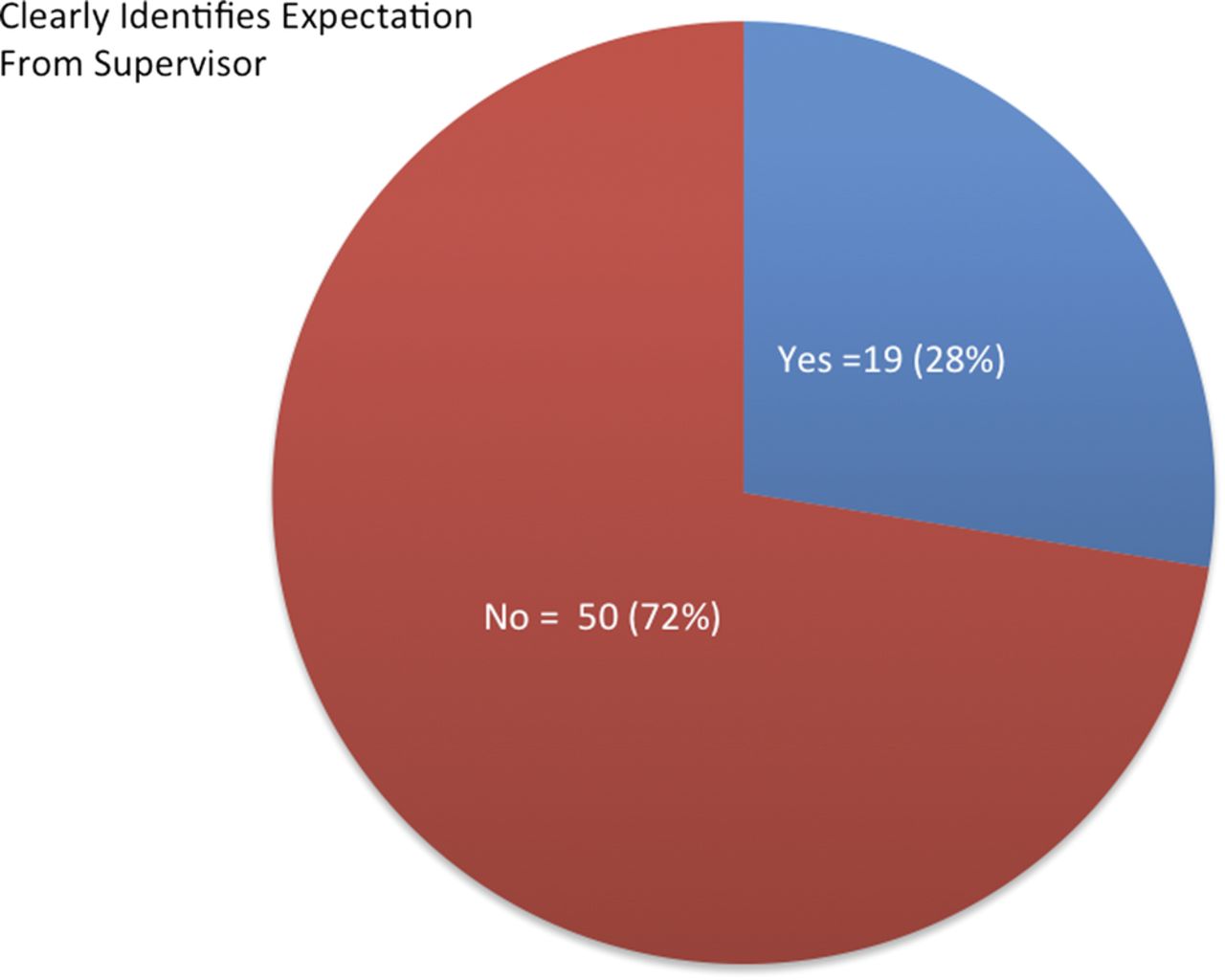
All 114 phone calls were recorded, of these 69 telephone calls were deemed as meeting the criteria for analysis. The results are summarised in table 1. Thirty per cent of students did not positively identify themselves by title and their full name. Thirty-two per cent did not positively identify the recipient of the phone call by confirming their name and title. Twenty-nine per cent of students did not identify their role. Forty-one per cent of students failed to positively identify the patient by name, age and gender (figure 1). Twenty-eight per cent of students did not clearly identify their expectation of their senior colleague (figure 2). Forty-nine per cent of students did not repeat back the recommendations of their senior colleague and 97% of students did not write down and repeat back their supervisors’ recommendations (figure 3).
Summary of results
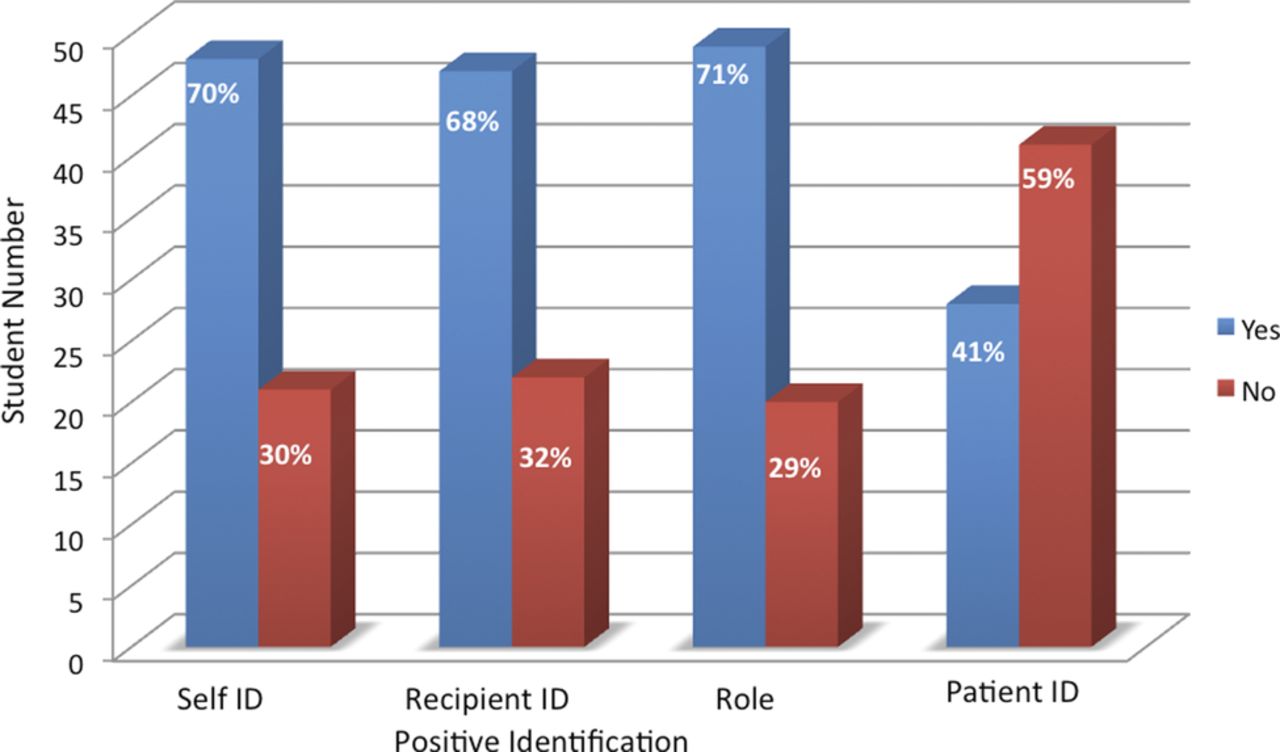
Students' positive identification of self, recipient, role and patient.

Students cleary identify their expectation of their senior colleague.

{kind=link}
{kind=link}
{kind=link}
Students reading back and writing down senior colleagues recommendations.
We present our data from this study with the following caveats that limit the conclusions that can be drawn. For our students it was their first experience of high-fidelity emergency medicine simulation, under observation by faculty, which may have increased or impeded performance. It is possible that our metric may have missed out on important aspects of the structure and content of telephone consultations. The performance of some students may have improved because of hearing feedback on previous scenarios thereby possibly improving communication performance; however, this would not have seemed to have had a significant impact on performance of ‘readback’ and writing down of recommendations from a senior colleague.
Discussion
Our study suggests a significant deficit in 30%, 32% and 29%, respectively, of our sample of final-year medical undergraduates, who did not demonstrate the ability to positively identify themselves, the patient or the recipient during communication via the telephone with a senior colleague. Likewise, 28% were unable to clearly identify the expectation they had of a senior colleague during a telephone consultation. That is whether they were simply informing, requesting advice or requesting that the senior colleague come to attend the patient in the simulation. Of particular concern is the high failure rate of 49% to repeat back instructions and the even higher failure rate of 97% to write down instructions given over the telephone despite receiving instruction with respect to both of these aspects during communications training previously in the curriculum. During debrief after each scenario a specific focus of the feedback process was on performance of communication skills by the students. Students readily identified lapses in appropriate communication in their comments on there performance. Many identified that being nervous and this being their first experience of simulation in this format impacted on their performance. Many also highlighted that this experience highlighted the importance of communication in practice and that would be a ‘take home’ learning point for them. We suggest the deficits highlighted above in the telephone communications reflect the absence of a structured and systematic approach by the medical students. It is our contention that the results reflect their lack of regular practice of these skills and limited assessment of these skills.
Should these skills be learnt ‘on the job’ in postgraduate training? The assumption that the ability will be acquired following qualification constitutes a latent error within the healthcare system.18 We believe that the function of undergraduate medical education is to produce graduates who are fit for purpose (as junior doctors) at the point of graduation.
We suggest that the way forward is to first of all focus on aspects of adult learning that can be applied to the teaching and learning of knowledge skills and attitudes in medical education. These areas focus on the learner, the learning process and the context of the learning process, respectively. To begin with the students must have a readiness to acquire the appropriate knowledge, and it is important that this knowledge is applicable to their perception of existing relevant problems. Factors in the non-cognitive domain such as the pacing of learning, the meaningfulness of the learning and the motivation for learning must be incorporated within the learning process. Finally the context of the learning must be skills specific for a given situation and these skills must pertain to solving relevant and authentic problems.
Second, we suggest that simulation is a way of skill development, transfer and maintenance that can support the learner on the path from novice to expert, from the classroom to the workplace in a safe and controlled manner. It is not a mere focus on procedural skills or performance rather it has a much more expansive perspective incorporating the affective and cognitive domains.
Third, we suggest that it is important to incorporate these skills sets into the clinical assessment process in undergraduate medical education. However, we join with Gordon and Findlay19 in recognising that there is a need for robust evidence on the ability of educational interventions to effect the transfer of such communication skills to the workplace.
Acknowledgments
We would like to acknowledge and thank Mr. Uwe Schiller for his support with the audiovisual recordings.
References
Footnotes
-
Contributors PH contributed to conception and the design of the study, the analysis and interpretation of data, to writing the paper and approval of the final version to be published. DP to the design of the study, the analysis and interpretation of data, to writing the paper and approval of the final version to be published. SDS contributed to conception and the design of the study, the analysis and interpretation of data, to writing the paper and approval of the final version to be published. TP contributed to the design of the study, revising the paper for important intellectual content and approval of the final version to be published. HH contributed to the design of the study, to revising the paper for important intellectual content and approval of the final version to be published. RG contributed to the design of the study, to revising the paper for important intellectual content and approval of the final version to be published. JM contributed to the design of the study, to revising the paper for important intellectual content and approval of the final version to be published
-
Funding The ASSET Centre is funded by University College Cork and is available for the training of undergraduate medical students from the School of Medicine University College Cork.
-
Competing interests None.
-
Ethics approval All of the participating students provided written consent and the Clinical Research Committee of the Cork Teaching Hospitals granted ethical approval for this study.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No further data are available.