Article Text

Abstract
Objectives India bears a significant portion of the global tobacco burden with high prevalence of tobacco use. This study examines the socioeconomic patterning of tobacco use and identifies the changing gender and socioeconomic dynamics in light of the Cigarette Epidemic Model.
Design Secondary analyses of second and third National Family Health Survey (NFHS) data.
Setting and participants Data were analysed from 201 219 men and 255 028 women over two survey rounds.
Outcomes and methods Outcomes included smoking (cigarettes, bidis and pipes/cigar), chewed tobacco (paan masala, gutkha and others) and dual use, examined by education, wealth, living environment and caste. Standardised prevalence and percentage change were estimated. Pooled multilevel models estimated the effect of socioeconomic covariates on the log odds of tobacco use by gender, along with fixed and random parameters.
Findings Among men (2005−2006), gradients in smoking by education (illiterates: 44% vs postgraduates: 15%) and chewing (illiterates: 47% vs postgraduates: 19%) were observed. Inverse gradients were also observed by wealth, living environment and caste. Chewed tobacco use by women showed inverse socioeconomic status (SES) gradients comparing the illiterates (7.4%) versus postgraduates (0.33%), and poorest (17%) versus richest (2%) quintiles. However, proportional increases in smoking were higher among more educated (postgraduates (98%) vs high schooling only (17%)) and chewing among richer (richest quintile (49%) vs poorest quintile (35%)). Among women, higher educated showed larger declines for smoking—90% (postgraduates) versus 12% (illiterates). Younger men (15–24 years) showed increasing tobacco use (smoking: 123% and chewing: 112%). Older women (35–49 years) show higher prevalence of smoking (3.2%) compared to younger women (0.3%).
Conclusions Indian tobacco use patterns show significant diversions from the Cigarette Epidemic Model—from gender and socioeconomic perspectives. Separate analysis by type is needed to further understand social determinants of tobacco use in India.
- Public Health
- Preventive Medicine
- Social Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
India bears a significant burden of tobacco consumption, with high prevalence of smoking and chewing among men and women.
-
Previous studies have established a unique social and spatial gradient in tobacco use. However, no studies have yet reported estimates for changing patterns in tobacco use prevalence or relative risk over time.
-
This study estimates socioeconomic patterns and examines the changing gender and socioeconomic dynamics of tobacco use in light of the Cigarette Epidemic Model.
Key messages
-
Among men, higher prevalence of smoking and chewing for less educated, poorer, rural and lower caste. Sharp and rising inequalities by survey year, but percentage change shows increases are greater among higher socioeconomic status (SES) groups—higher education, urban, richer populations, previously unreported.
-
Low and declining risks of smoking and chewing among women. Higher rates of chewing compared to smoking. Increase in smoking with urbanisation for women. Greater declines over time for higher-educated women.
-
Significant changing trend by wealth, education and living environment in smoking among men and in chewing among women. Increases in smoking prevalence among younger men (15–24 years) and chewing among younger women (15–24 years).
Strengths and limitations of this study
-
First systematic examination of socioeconomic patterns in tobacco use in India, highlighting SES gradients in use and risks among vulnerable populations.
-
Large sample, representative and generalisable surveys providing repeated and comparable estimates over time.
-
Limitations: (1) cross-sectional data, limiting scope for causal inference, (2) lack of data by tobacco type or volume of use and (3) data from a reproductive health survey may suffer from social desirability bias.
Introduction
Global estimates indicate that 1 in 10 adult deaths can be attributed to tobacco consumption, leading to approximately five million global deaths per year.1–4 Of these, 2.4 million deaths occur in developing countries. India bears a significant portion of this global tobacco burden.3 ,4 Consumption of both smoked and smoke-less (chewed and inhaled) forms of tobacco is highly prevalent among men (47%) and women (14%).5 However, previous studies have indicated that tobacco use, like other non-communicable disease risk factors, is unequally distributed across different social determinants in India—education, caste and wealth—among both men and women,1 ,5–7 indicating a distinct ‘economic and spatial distribution’ in tobacco use.6 No studies have yet systematically examined patterns and changes in the prevalence of tobacco consumption in India by socioeconomic factors over time.
In this study, we aim to provide estimates and inferences on the changing gradient of tobacco consumption in India, analysing prevalence and OR patterns from the National Family Health Surveys (NFHS).8 ,9 We discuss our findings in light of the Cigarette Epidemic Model10 ,11 and examine what populations show higher and lower prevalence of tobacco consumption over time.
Methods
Data were analysed from two rounds of the Indian NFHS (2 and 3) conducted during 1998–1999 and 2005–2006, respectively. NFHS is a national representative cross-sectional survey that is collected and managed by the Indian Institute of Population Sciences (IIPS) in Mumbai, India. These surveys provide vital sources of information on demographic, health and socioeconomic behaviour of Indian households. Data from men and women in the age group of 15–49 years were used from both survey rounds to ensure comparability. Data are representative of all Indian states (except for the small Union Territories), hence covering almost 99% of the country's population. The surveys were collected using multistage cluster random sampling techniques. Rural and urban areas were sampled separately and a uniform sample design was followed in each state; states and PSUs are considered as levels. Individual questionnaires for men and women were used to interview usual residents of the household or visitors who stayed in the house the night before. Further details on sample design, including sampling framework and sample implementation, are provided in the basic survey reports by IIPS.8 ,9
Outcomes of interest included smoking (cigarettes, bidisi and pipes/cigar), chewing tobacco (paan masala,ii gutkhaiii or other chewed forms of tobacco) and dual use (consuming both smoked and chewed forms) of tobacco. NFHS-3 provides details on the different types of smoked and chewed tobacco products, but this information was unavailable in NFHS-2. The main covariates of interest were age, marital status and education at the individual level, and household wealth, area of residence (urban/rural), religion and caste/tribe status at the household level (variable definitions are provided in table 1). Survey-weighted age-standardised prevalence estimates of smoking, chewing and dual use of tobacco along with percentage change were calculated. Pooled multilevel models with state, local area and individual as analytical levels were used to estimate the effect of wealth, education, living environment and caste on the log odds of smoking and chewing among men and women. Regression models were adjusted for age, religion and marital status. Survey year was used in the interaction terms to estimate a time trend in socioeconomic determinants of tobacco. Tests for trend included joint tests for significance of fixed parameters and significance tests for random parameters. Model estimates were maximum likelihood based using the Iterative Generalised Least-Squares (IGLS) algorithm as implemented within the MLwin software programme (V.2.23).
Prevalence (%) of tobacco smoking, chewing and dual use (smoking and chewing) by wealth, education and caste/tribe status among men and women in the National Family Health Surveys (NFHSs) 1998–1999 and 2005–2006
Results
Data used in this analysis covered 131 464 men and 130 886 women residing in 92 486 households in NFHS-2 and 69 755 men and 124 142 women residing in 109 041 households in NFHS-3, with an overall response rate of 96% for NFHS-2 and 98% for NFHS-3. Prevalence (%) of smoking, chewing and dual use of tobacco over two survey rounds are presented by the three primary markers of socioeconomic status (SES)—education, wealth and caste (table 1) along with percentage change estimates. Estimates by living environment, marital status, age and religion are presented in the appendix (see web table 1). Among men, the prevalence of tobacco use (smoking, chewing and dual use) was seen to increase across all socioeconomic groups. For instance, smoking has risen from 35.5% to 40.6% in the fifth (poorest) quintile, 30.6% to 36.5% in the fourth quintile, 25.6% to 31.4% in the middle quintile, 19.3% to 25.8% in the second quintile and 11.9% to 19.9% in the first (richest) quintile (table 1). Chewed tobacco use increased from 34.4% to 47.1% among the illiterate populations, 30.2–41.9% among those with primary schooling only, 23.3–33.1% among those with high-school education, 14.9–23.9% among those with college education and 12.4–18.5% among those with postgraduate degree. Higher prevalence of tobacco use among men in each survey round was seen for socioeconomically disadvantaged groups—with less educated, lower wealth, rural residence or lower caste showing an inverse SES gradient; however, greater proportional increases in prevalence over time were seen among higher SES groups. For instance, higher absolute smoking prevalence in NFHS-3 was seen among men in lower wealth quintiles compared to those in higher wealth quintiles (41% for fifth (poorest) quintile and 37% for fourth quintile, compared to 20% in first (richest) quintile and 26% in second quintile); higher percentage increases in smoking were recorded among first (richest) quintile (63%) and second quintile (37%) compared to fourth quintile (21%) and fifth (poorest) quintile (13%). Similar trend was seen for education with a 98% increase in prevalence among those with postgraduate education and 13% increase in prevalence among those with no education over the two survey rounds. Sharper inequalities with higher inter-group differences were seen for smoking compared to chewing. Prevalence of chewing among men in the richest quintile and with postgraduate education each increased by 49%, while that for the poorest increased by 35% and for those with no education increased by 37%.
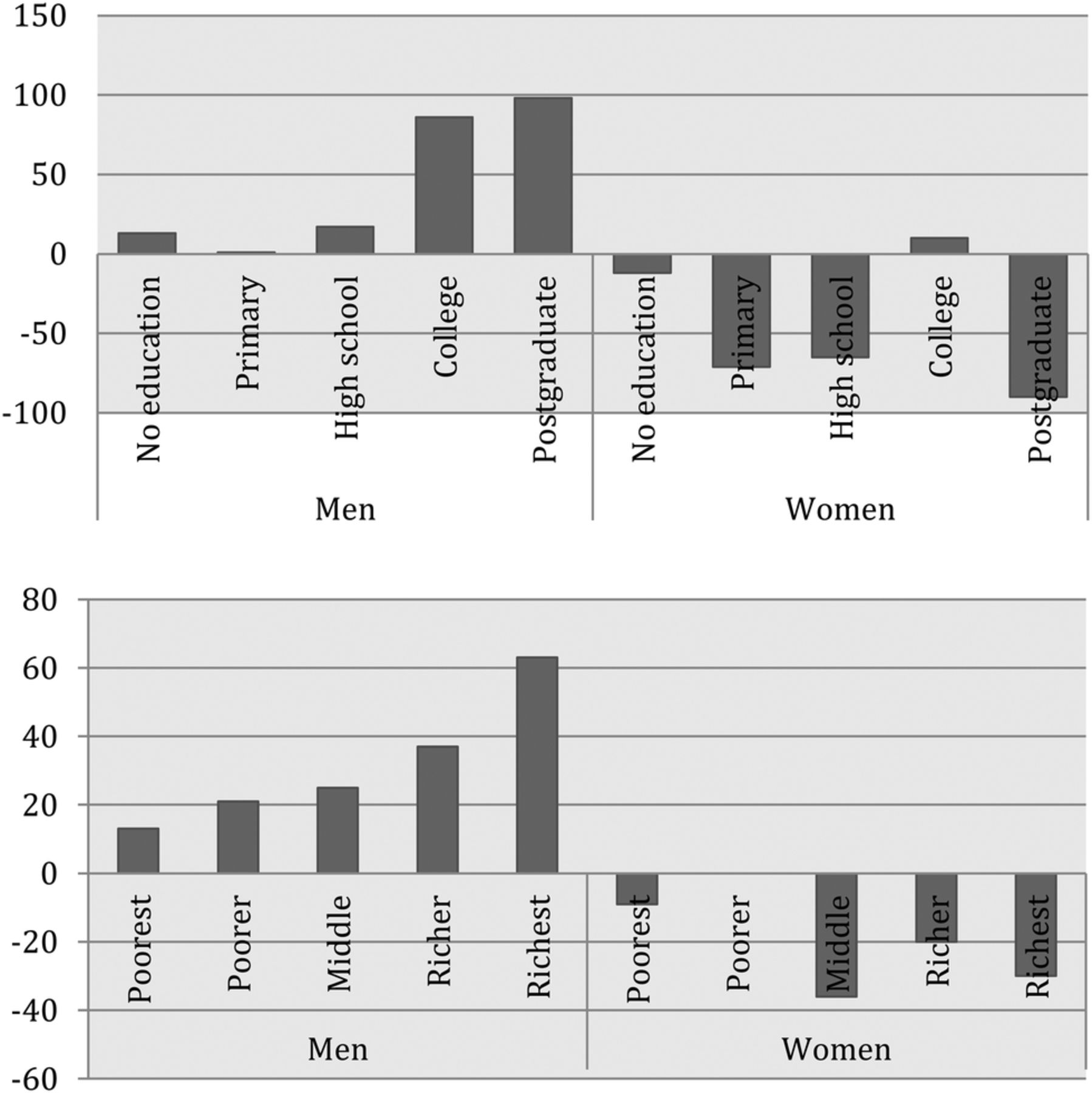
Socioeconomic patterns for tobacco use among women differed distinctly. Overall prevalence rates of tobacco use among women were significantly lower than men. In 2005–2006, prevalence of smoking and chewing among women with no education was 2.3% and 13.3%, respectively, while the same for men was 43.9% and 47.1%, respectively (table 1). Women in most SES categories showed a declining trend for tobacco use, and only scheduled caste women and those with college education showed small increases in smoking and chewing. Higher and more consistent declines in prevalence were seen for education, compared to wealth and caste. For instance, women with postgraduate education noted a 90% decrease in smoking and a 73% decrease in chewing (table 1). Women in the first (richest) quintile showed a decline of 30% for smoking and 8% for chewing (table 1). Results by area of residence (see web table 1) showed an increase in risks for tobacco use with urbanisation among both men and women, except in the prevalence of chewed tobacco among women. Figures 1 and 2 show the percentage change in smoking and chewing by education and wealth for men and women reflecting findings from table 1.

Percentage change in smoking among men and women by education level and wealth quintiles.

Percentage change in chewing among men and women by education level and wealth quintiles.
Tables 2 and 3 present results from pooled multilevel models showing ORs for smoking and chewing by education, wealth, living environment and caste, along with interactions with survey year. Gradients in ORs (95% CI) are seen by all four markers of SES among men and women for smoking and chewing with sharper inequalities seen for education and wealth, compared to other markers. Controlling for wealth, caste and living environment and compared to those with postgraduate education, the OR of smoking for men with no education: 3.18 (95% CI 2.96 to 3.43), with primary education: 2.73 (95% CI 2.54 to 2.94), with high school education: 1.81 (95% CI 1.69 to 1.85) and with college education: 1.38 (95% CI 1.28 to 1.49). Controlling for education, caste and living environment and compared to the first (richest) quintile, OR for chewing in the second quintile: 1.43 (95% CI 1.38 to 1.48), middle quintile: 1.75 (95% CI 1.68 to 1.82), fourth quintile: 1.92 (95% CI 1.84 to 2.01) and fifth (poorest) quintile: 2.1 (95% CI 1.99 to 2.2). Interaction terms in the two tables provide effect estimates for change over the two survey rounds. Among men, significant parameters for interaction terms for smoking are seen by wealth, education (except college educated) and living environment (except for small city); and for chewing by wealth, higher education and by residence in towns. The joint test for interaction of fixed terms is significant for smoking by wealth (joint test: 174.31, p<0.001), education (joint test: 13.31, p=0.009) and living environment (joint test: 13.44, p=0.003) and for chewing by wealth (joint test: 15.63, p=0.003), representing robust change over time. χ2 values for random parameters are significant both at state (smoking χ2: 12.82, p=0.0003 and chewing χ2: 12.89, p=0.0003) and local area (smoking χ2: 650.41, p<0.0001 and chewing χ2: 801.4, p<0.0001) level showing variation at both levels.
Pooled regression models showing ORs (95% CIs) for smoking and chewing among men and interactions for wealth, education, residence and caste over time
Pooled regression models showing ORs (95% CIs) for smoking and chewing among women and interactions for wealth, education, residence and caste over time.
Among women, controlling for education, caste and living environment and compared to those in the first (richest) quintile, the OR of smoking in second quintile: 1.48 (95% CI 1.28 to 1.71), middle quintile: 1.9 (95% CI 1.64 to 2.2), fourth quintile: 2.75 (95% CI 2.37 to 3.19) and fifth (poorest) quintile: 3.95 (95% CI 3.39 to 4.6). Controlling for wealth, caste and living environment and compared to those with postgraduate education, OR of chewing among women with college education: 1.84 (95% CI 1.55 to 2.19), high-school education: 2.19 (95% CI 1.86 to 2.57), primary schooling: 2.87 (95% CI 2.44 to 3.4) and no education: 3.85 (95% CI 3.27 to 4.53). Significant ORs for interaction terms are seen for smoking by wealth (joint test: 19.128, p<0.0001) and for chewing by wealth (joint test: 31.96, p<0.0001), education (joint test: 17.42, p<0.0001) and living environment (joint test: 157.008, p<0.0001). χ2 values for random parameters are significant for both state (smoking χ2: 12.91, p=0.0004 and chewing χ2: 12.94, p=0.011) and local area (smoking χ2: 264, p<0.0001 and chewing χ2: 839, p<0.0001), showing variation at both levels. Figure 3 presents adjusted probability estimates for smoking and chewing among men and women by wealth and education from multilevel models, which show findings similar to prevalence estimates.

{kind=link}
{kind=link}
{kind=link}
Probability of smoking and chewing among men and women by education and wealth. NFHS, National Family Health Survey.
Discussion
In 1994, Lopez et al10 proposed the four-stage Cigarette Epidemic Model discussing transitions in smoking prevalence, consumption amount and mortality in developed countries. As per the model in stage I, male smoking prevalence is comparatively low and rising (< 20%) and female smoking prevalence does not exceed 5% due to sociocultural factors. In stage II, tobacco prevalence among men starts to rise rapidly and peaks around 50–80% with female smoking increasing at a lagged pace behind men. In stage III, prevalence rates for smoking among men start to fall, with both male and female smoking converging. Increases are seen for smoking rates among younger compared to older populations. In stage IV, prevalence of smoking begins to decline for both men and women. Mortality attributable to smoking rises to about one-third for all men, with much lower mortality rates seen among women. This model was developed based on empirical data from developed countries and has not been tested in developing countries. However, in 2011, Thun et al11 proposed modifications to the model potentially relevant for developing countries and were the first to note that smoking patterns by gender in developing countries distinctly differ from patterns noted in developed countries. India shows a high and complex burden of tobacco consumption, as also reported in tobacco surveillance studies.2 ,12 ,13 This paper uses empirical evidence to show that India is currently between stages II and III of the Cigarette Epidemic model on the basis of estimates of smoking for men, but distinctly differs from the model on the patterns seen for women.
Overall, several dissimilarities are noted in the Indian experience from this model. First, India's unique tobacco experience comprises a ‘double burden’ of smoked and chewed tobacco consumption. Patterns for smoking and chewing seem to follow trajectories that differ by education, living environment and wealth. Further, within smoking, differences potentially exist by SES in the consumption of cigarettes from bidis, which most data are unable to distinguish. The quantity and quality of these products may differentially determine the mortality burden attributable to tobacco use in India.14–16 Assessment of the disease, mortality and cost burden of the tobacco epidemic needs to account for this complexity.14 ,15
Second, socioeconomic and sociocultural dynamics play profound roles in impacting tobacco use in India. Differences in tobacco consumption are seen by major SES markers such as wealth, education, living environment and caste. Findings from this analysis indicate a dichotomy between higher absolute prevalence by lower caste, wealth and education levels; but higher relative change in prevalence over time by higher caste, wealth and education levels. No previous study has reported this finding for India. Urbanisation seems to be playing an increasing role in impacting tobacco use for men and women. Further analyses by type and amount of tobacco consumed are needed to systematically understand these patterns.
Third, social gradients in tobacco use (overall and by type of tobacco) in India distinctly differ by gender. Despite women's empowerment, large-scale increases in women's smoking as predicted by the Cigarette Epidemic Model are yet to be seen in India.,10 ,11 ,17 ,18 Aggregate estimates show that women are far behind men in prevalence rates for smoking; and smoking and chewing rates among women, barring a few groups, seem to be declining. The reasons for this could be several. First, that Indian sociocultural realities and lower acceptability of smoking among women lead to delays in age of initiation of smoking and higher rates among older compared to younger women (see web table 1). Women's smoking has been linked to their empowerment, but this may be confined to urban areas and it is possible that on average, smoking continues to remain a social taboo among women. Representation of smoking in the media may also explain the gender patterns in the use of tobacco; smoking has been projected as an expression of masculinity among men and has moralistic connotations for women.19–21 Second, an economic perspective explaining the lower smoking rates among women in India may attribute this statistic to women's unequal participation in the labour market and limited access to personal disposable income. Higher smoking among women in cities may partly indicate greater uptake of smoking by employed women. Third, given that data for this analysis come from a reproductive health survey, it is possible that results for women are an underestimate. Web table 1 indicates that older (above 35 years of age) women are more likely to use tobacco. However, patterns in this analysis match findings from other tobacco studies such as the GATS (global adult tobacco survey) in India (IIPS),5 ,6 providing a counter to this argument.
Finally, evidence on the socioeconomic gradient in tobacco use in India needs to be linked to its implications for tobacco-related mortality and morbidity.14 ,15 Dikshit et al15 provide the first estimates of cancer mortality in India, attributing a major component of age-standardised cancer mortality from lung and oral cancers to high rates of tobacco use in India. Analyses stratifying cancer morbidity and mortality in India by SES have not yet been attempted, and the lack of reliable surveillance data for chronic diseases prevent exhaustive assessments of the impact of tobacco use on Indian current and future chronic disease burden.22
This study provides a systematic examination of the socioeconomic patterns in tobacco use in India over time. Data in this analysis come from the NFHS, which is a large, representative and generalisable survey, providing a comparative picture of tobacco patterns over time. The limitations of this analysis are the following. First, the surveys are cross-sectional, hence limiting scope for causal inference. NFHS does not provide detailed data by type or volume of tobacco. Finally, NFHS is a reproductive health survey where women in the ages of 15–49 years are sampled. Men are sampled in the households of the female sample. This introduces the potential for two downward biases. The first pertains to social desirability bias particularly related to underestimation of smoking patterns in women's childbearing years. Second, since the sample of men is conditional on the households from which women were sampled, the pool of men sampled may not be representative. Despite these caveats, NFHS (and in general the demographic and health surveys (DHSs)) has proven to be representative and generalisable, and continues to be used in a number of studies related to tobacco.5 ,6 In addition, our findings are consistent with estimates from studies using other surveys assessing the burden of tobacco and its drivers in India.2 ,23 Tobacco burden in the ‘productive’ populations (14–50 years) not only represents the current burden of tobacco but may predict future morbidity.
We present empirical evidence that India is experiencing a unique economic and social transition in tobacco consumption, quite distinct from the experience of developed countries that is likely to manifest in a number of morbidities.2 ,14 ,15 In order to ensure policy effectiveness to prevent and reduce the exposure to tobacco, there is a need to systematically monitor and examine the social inequities in tobacco use over time and channel interventions to the social groups that are most vulnerable to these inequalities.
Acknowledgments
We acknowledge the support of Macro International Inc (Washington, DC) for providing access to the surveys.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
Footnotes
-
Contributors SVS and NB conceptualised and planned the study. NB led the data analysis, interpretation and writing of the manuscript. SS, MAS and SA contributed to data analysis and writing of the manuscript. CJM and SS contributed to the interpretation and writing of the manuscript. SVS contributed to the interpretation and writing of the manuscript, and provided the overall supervision.
-
Funding NB is supported by the Presidential Scholarship at Harvard University. SA is supported by a Wellcome Trust Strategic Award Grant No. Z/041825. CM conducted this work during a Study Abroad Fellowship funded by the Leverhulme Trust. CM is also funded by the Higher Education Funding Council for England and the National Institute for Health Research.
-
Competing interests None.
-
Ethics approval Secondary analysis of open-source datasets.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Data for the analysis comes from the India chapter of the Demographic and Health Surveys (DHS) and is freely available online at the Measure DHS website. It is also available from the International Institute for Population Sciences (IIPS), Mumbai, India.
-
↵i Bidis are local inexpensive cigarettes, which are thinner and contain tobacco flakes rolled inside tendu leaves. Bidis are often smoked by poorer populations.
-
↵ii Paan masala is a powdered preparation of betel leaves combined with cured tobacco and/or areca nut, which has stimulating properties.
-
↵iii Gutkha is a savoury or sweet preparation containing areca nut, tobacco, catechu, paraffin and slaked lime.