Article Text

Abstract
Background: There is uncertainty as to the dose of inhaled corticosteroids (ICS) at which to start concomitant long acting β agonist (LABA) treatment in patients with asthma not adequately controlled by ICS alone.
Methods: A meta-analysis was carried out of randomised, double blind clinical trials that compared the efficacy of adding salmeterol to moderate doses of ICS (fluticasone propionate 200 μg/day or equivalent) with increasing the ICS dose by at least twofold in symptomatic adult patients with asthma. The main outcome measures were the number of subjects withdrawn from the study due to asthma and the number of subjects with at least one moderate or severe exacerbation.
Results: Twelve studies with a total of 4576 subjects met the inclusion criteria for the analyses. The number of subjects withdrawn due to asthma and with at least one moderate or severe exacerbation was higher in the high dose ICS group (odds ratios 1.58, 95% CI 1.12 to 2.24 and 1.35, 95% CI 1.10 to 1.66, respectively). For the secondary outcome variables (forced expiratory volume in 1 second, morning and evening peak expiratory flow, and daytime β agonist use) there was significantly greater benefit in the salmeterol group.
Conclusions: This meta-analysis shows that the addition of salmeterol to moderate doses of ICS (fluticasone 200 μg/day or equivalent) in patients with asthma symptomatic at that dose results in significantly greater clinical benefit than increasing the dose of ICS by twofold or more.
- BDP, beclometasone dipropionate
- FEV1, forced expiratory flow in 1 second
- ICS, inhaled corticosteroid
- LABA, long acting beta agonist
- PEF, peak expiratory flow
- asthma
- inhaled corticosteroid
- long acting β agonist
- combination treatment
Statistics from Altmetric.com
- BDP, beclometasone dipropionate
- FEV1, forced expiratory flow in 1 second
- ICS, inhaled corticosteroid
- LABA, long acting beta agonist
- PEF, peak expiratory flow
The recent British consensus guidelines on asthma management recommend a long acting β agonist (LABA) drug as first line add on therapy at step 3 in patients not controlled on inhaled corticosteroids (ICS) alone.1 However, this recommendation is made over a fourfold ICS dose range (200–800 μg/day beclometasone dipropionate (BDP) or equivalent). The dilemma for clinicians is to know at what dose of ICS within this range to start concomitant LABA treatment in a patient inadequately controlled on ICS alone.
This dilemma is partly due to the heterogeneity of ICS doses used in clinical studies which have compared the efficacy of adding a LABA with increasing the dose of ICS. For example, in the original MIASMA meta-analysis in which the addition of salmeterol was significantly more effective than increasing the dose of ICS, the baseline daily dose of ICS ranged from 400 to 1000 μg BDP or equivalent.2 It was not therefore possible to determine whether there was a differential response across the ICS therapeutic range. In addition, a number of studies were included that used doses of ICS already near the peak of the dose-response curve—that is, 500 μg/day fluticasone or equivalent.3–5 While recognising that there is considerable individual variability in the response to ICS in asthma,6 it would be expected that these inclusion criteria would have favoured the salmeterol group because further increasing the dose of ICS above 500 μg/day fluticasone or equivalent would have produced minimal further benefit. In contrast, most of the studies comparing the effect of the addition of formoterol to increasing the dose of ICS have examined low baseline doses of ICS at which most of the therapeutic response has not been obtained.7,8,9,10 Likewise, this approach is not favoured due to the clinical preference to obtain most of the therapeutic benefit from ICS before adding an additional agent.
In this meta-analysis we have compared the clinical benefit of adding salmeterol in patients not controlled on moderate doses of ICS (200 μg/day fluticasone or equivalent) with increasing the dose of ICS by at least twofold. In this way we have attempted to compare more accurately the relative benefits of both therapeutic options and thereby provide some guidance on what is a common dilemma facing clinicians in daily practice.
METHODS
Search strategy
A search was conducted of Medline from January 1966 to August 2003, of EMBASE from 1980 to August 2003, and of the Cochrane Controlled Trials Register. On Medline, a search of studies containing the keyword “salmeterol” using the MeSH subject heading “asthma” and “chemical and pharmacologic phenomena” (MeSH) and “inhaled corticosteroid” was undertaken. When limited to English the total number of studies was 629. GlaxoSmithKline, the manufacturer of salmeterol, was approached for details of all relevant studies; no additional studies were identified. There were no additional relevant studies published in other languages on Medline or EMBASE. Finally, the reference lists of relevant studies were examined but no other studies were found. The search strategy as recommended by the QUOROM statement is shown in fig 1.
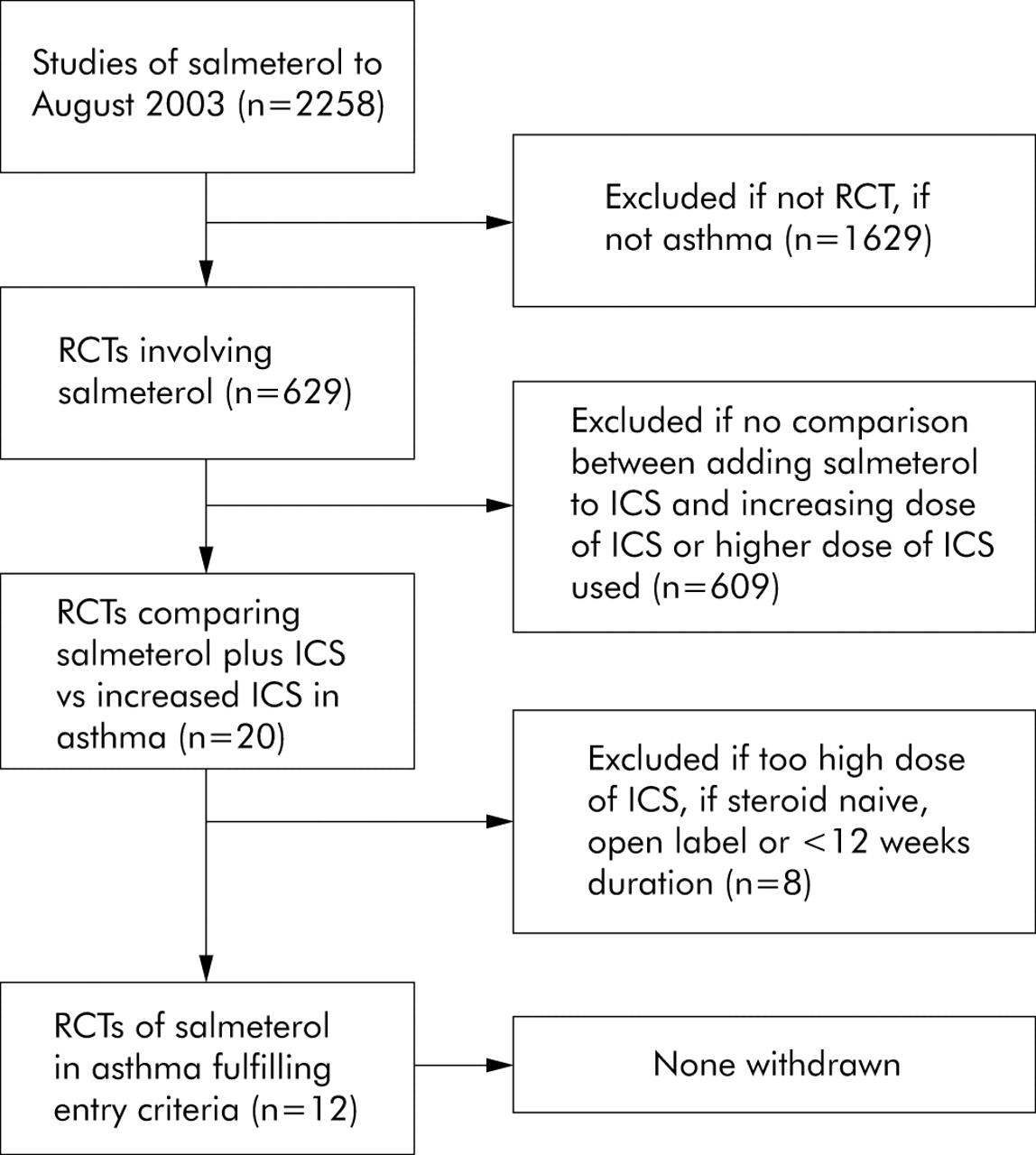
Results of search of Medline, EMBASE and GlaxoSmithKline databases for clinical studies eligible for inclusion in meta-analysis.
Inclusion criteria
Two people independently examined the title and abstract of each paper, then the full paper if necessary. To be included in the meta-analysis, studies had to meet all of the following criteria: a double blind, randomised trial of adolescents (⩾12 years of age) or adults with asthma symptomatic on moderate doses of ICS (200 μg/day fluticasone or equivalent); direct comparison between moderate doses of ICS (200 μg/day fluticasone or equivalent) and salmeterol versus at least a twofold higher dose of ICS (⩾400 μg/day fluticasone or equivalent) administered twice daily; studies of at least 12 weeks duration; and data on measures of clinical efficacy. Studies in which participants were dependent on oral steroids or involved in oral steroid reduction regimes were excluded.
Data extraction
Data extraction was based on reported summary statistics (means, SD and SE). The primary outcome measures were the number of subjects withdrawn due to asthma and the number of subjects with at least one moderate or severe exacerbation. Secondary outcome measures included morning and evening peak expiratory flow (PEF), forced expiratory volume in 1 second (FEV1), night awakenings, and daytime and night time β agonist use. Data were primarily obtained from the original publications. If the data were not available in the standardised format in the original publications, they were either obtained from the MIASMA publication or were provided by GlaxoSmithKline (the manufacturer of salmeterol) in the format required. To assess the validity of data, two investigators correlated the data from the different sources. If discrepancies between sources were found, the data were preferentially obtained from the original publication, followed by MIASMA, and then the data provided by GlaxoSmithKline.
In the individual studies, moderate or severe exacerbations were defined as any event requiring treatment with oral/parenteral corticosteroids and/or emergency hospital treatment and/or any asthma medication not allowed as concurrent treatment during the study. Symptom scores could not be analysed because of differences in assessment of symptoms between studies or because the information was not available in the format required. For withdrawals due to asthma, a continuity correction was used in the analysis because the data sets in the papers by Van Noord et al11 and Kalberg et al12 had “zero” cell counts.
Data analysis
For continuous variables a standard method of pooling means based on standardised mean differences using an inverse variance weighting approach13 was used. A weighted mean standard deviation was used to translate the standardised mean difference back into the original units. In the forest plots the area of the box is proportional to the variance of the estimate for the individual trials.
For the categorical variables the log odds ratio was pooled using the inverse variance weighting approach.13 The forest plots are presented as the log of the odds ratio and the area of the box is, where possible, proportional to the variance of the estimate for the individual trials. If the variance of individual trial estimates was too large to fit the scale of the plot, the area of the box is reduced to a quarter of the variance; this was required for the two primary outcome variables. Heterogeneity statistics and inconsistency measurements, the latter according to the method of Higgins and Thompson,14 were calculated for all the comparisons. SAS Version 8.2 was used.
RESULTS
Twelve studies with a total of 4576 subjects met the inclusion criteria for the analysis (table 1).11,12,15–23 The mean FEV1 was 64% of predicted normal values (range 40–85%), indicating that subjects had moderate to severe asthma. By virtue of the inclusion criteria used, the methodological quality of included studies was high with all studies achieving a Jadad score of 4 or more.24 In two studies20,21 subjects were only eligible to participate if they had been shown to be unstable on 200 μg/day fluticasone. They were then treated with fluticasone 500 μg/day in the run in phase, before randomisation to fluticasone 200 μg/day and salmeterol or fluticasone 500 μg/day. Comparisons were made between the addition of salmeterol to BDP 400 v 1000 μg/day in one study, BDP 400 v 800 μg/day in three studies, fluticasone 200 v 500 μg/day in six studies, fluticasone 200 v 400 μg/day in one study, and fluticasone 200 μg/day v budesonide 800 μg/day in one study. The study by Baraniuk et al22 was the combined publication of two separate studies (FLTA 4021 and FLTA 4022). The combination salmeterol/fluticasone (Advair/Seretide) inhaler was used in three studies.
Summary of studies included in the meta-analysis
Evidence of heterogeneity was found for several of the outcome variables including morning PEF (where the heterogeneous studies were in the same direction as the others), FEV1 (where one study was more positive and another more negative), daytime β agonist use (two studies showing less difference), and night time β agonist use (with two studies having more effect). For all these the confidence intervals became wider under the random effects models, and for FEV1 and night time β agonist use this led to the lower confidence limit being close to or at zero, consistent with no difference in effectiveness between the two strategies. For the other secondary outcome variables there was no substantive difference to the conclusions.
Main outcome measures
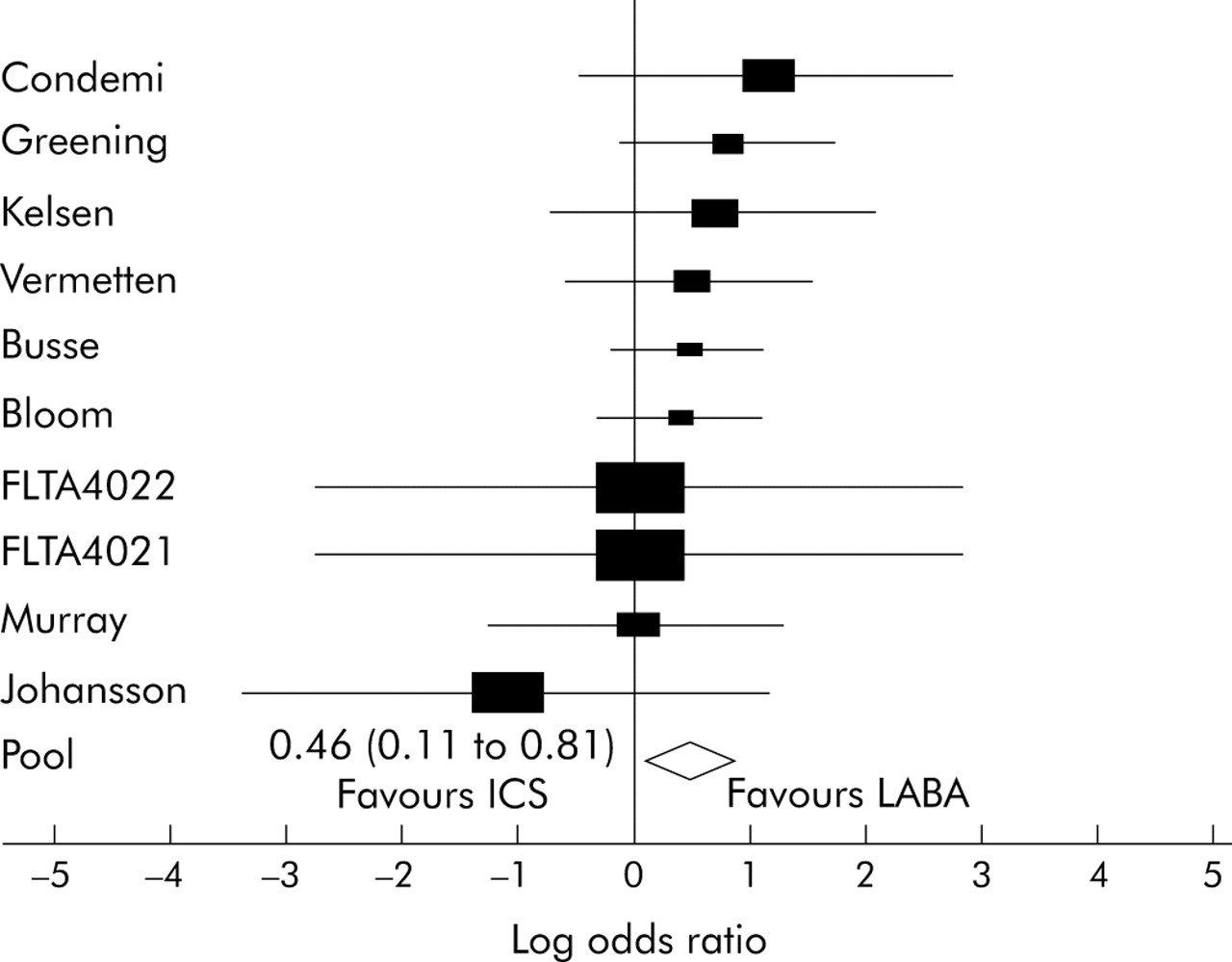
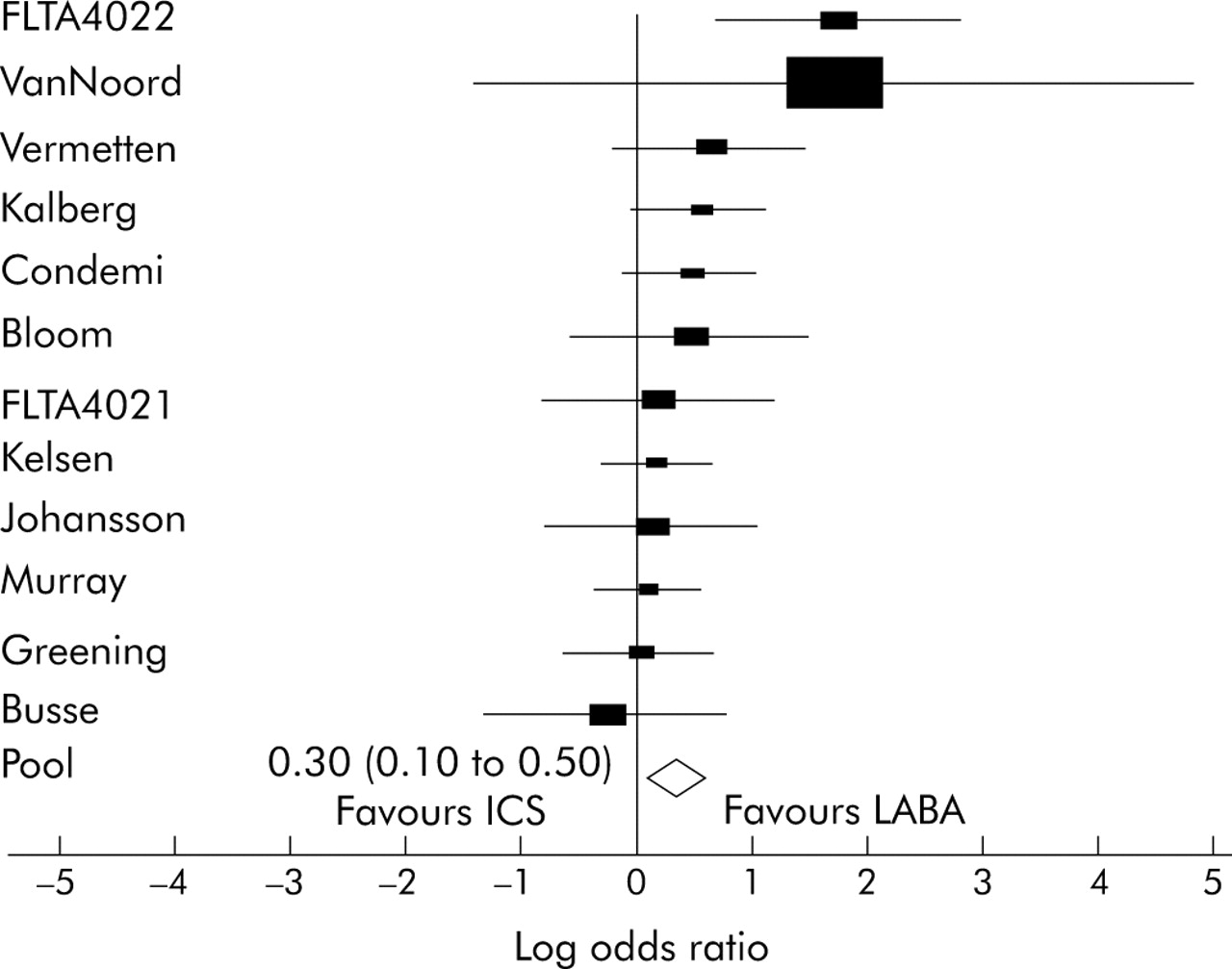
There was a significant reduction in the number of subjects withdrawn due to asthma in the low dose ICS/salmeterol group (59/2036) compared with high dose ICS treatment (86/1992) with an odds ratio of 1.58 (95% CI 1.12 to 2.24) (table 2, fig 2). There was a significant reduction in the number of subjects with one or more moderate or severe exacerbation in the low dose ICS/salmeterol group (184/2312) compared with high dose ICS treatment (243/2264) with an odds ratio of 1.35 (95% CI 1.10 to 1.66) (table 2, fig 3).
Numbers of subjects withdrawn due to asthma and number of subjects with at least one moderate or severe exacerbation, and associated odds ratios (95% CI) between treatment with salmeterol and increased dose of inhaled corticosteroid

Odds ratio for proportion of withdrawals due to asthma. Forest plot of fixed effects. ICS, inhaled corticosteroids; LABA, long acting β agonist.

{kind=link}
{kind=link}
{kind=link}
Odds ratio for number of subjects with one or more moderate or severe exacerbation. Forest plot of fixed effects. ICS, inhaled corticosteroids; LABA, long acting β agonist.
Secondary outcome measures
Mean morning PEF and evening PEF were significantly greater and daytime β agonist use was reduced in those who received low dose ICS/salmeterol compared with high dose ICS, with differences of 23 l/min, 19 l/min, and −0.6 puffs per day, respectively (table 3). Significantly greater improvements were also observed for FEV1, although the lower confidence limit was closer to no difference. For night awakenings and night time β agonist use, the lower confidence limits included no difference in effect although the point estimates favoured the ICS/salmeterol group.
Mean difference (95% CI) for all secondary outcome measures between the group receiving added salmeterol and the group receiving increased dose of ICS
DISCUSSION
In this meta-analysis we have shown that, in patients symptomatic on ICS at a dose of 200 μg fluticasone or equivalent, the addition of salmeterol is superior to increasing the dose of ICS by at least twofold for all major clinical outcome measures. For the main outcome variables of withdrawals due to asthma and at least one moderate or severe exacerbation, subjects receiving salmeterol had a 35–50% reduced risk compared with higher dose ICS treatment. The secondary outcome variables of lung function and β agonist use were also significantly improved compared with the higher ICS dose.
There are issues relating to the design of the study that are relevant to the interpretation of the results. The most important was the decision to restrict the analysis to studies that used a baseline dose of ICS of 200 μg/day fluticasone or equivalent. While recognising the marked individual variability in response to ICS5 and the requirement for higher doses in certain circumstances,25,26 this ICS dose was chosen as its use results in 80–90% of the maximum obtainable benefit for all clinical outcome measures including exacerbations.3–5
Consideration was given to broadening the inclusion criteria to include similar studies of the LABA formoterol. This was not undertaken due to the paucity of such studies which used an equivalent baseline daily dose of ICS and the lack of data presented in the same standardised format.7,8,9,10 However, the findings are complemented by the FACET study in which budesonide at 800 μg/day resulted in significantly fewer severe exacerbations than low dose budesonide (200 μg/day) plus formoterol.7 This study illustrates the importance of obtaining most of the therapeutic benefit from ICS therapy before considering add-on therapy in patients with symptomatic asthma.
By limiting the analysis to studies of salmeterol, we were able to include 12 studies involving over 4500 patients with asthma including five studies of 1935 subjects not included in the original MIASMA publication.2 We are confident that we obtained all eligible studies as a result of the comprehensive search strategy undertaken. However, even with the strict inclusion criteria employed, our meta-analysis did include studies in which salmeterol was added to different ICS (BDP and fluticasone), different inhaler devices (Diskus and MDI), and both combination and separate inhalers. We were provided with data in a standardised format from GlaxoSmithKline which, in addition to the data published in the original manuscripts and MIASMA, allowed data to be used in a standardised format across the studies included in the meta-analysis.
Another issue was the choice of the main outcome variables—withdrawals due to asthma and one or more moderate or severe exacerbations. This analysis differed from the original MIASMA study2 in that we did not include mild exacerbations which incorporated an increase in β agonist use as this would be expected to be reduced with concomitant LABA treatment. However, even with the use of withdrawals due to asthma, the results must be interpreted with some caution as the number of withdrawals due to asthma was relatively few in comparison with total withdrawals. With regard to moderate to severe exacerbations, this may have included some episodes that reflected “loss of asthma control” rather than clinically severe exacerbations, and the paucity of hospital admissions prevented this specific outcome measure being used. Furthermore, it is likely that there was a close correlation between withdrawals due to asthma and moderate or severe exacerbations. However, despite these limitations we consider that withdrawals and moderate or severe exacerbations are of greater clinical relevance than lung function measures, particularly with comparisons between ICS and LABA treatment. Consistent with the findings for these main outcome measures, the secondary outcome measures including lung function measures such as clinic FEV1, morning and evening PEF, and β agonist use also favoured the salmeterol group.
Finally, it is worthy of comment that, although the studies in this meta-analysis were restricted to salmeterol as the LABA, the evidence that salmeterol and formoterol have similar efficacy in the long term treatment of asthma27,28 would suggest that the results are probably applicable to the class of LABAs.
In conclusion, recent meta-analyses of the dose-response of ICS demonstrate a relatively flat dose-response relationship with 80–90% of the maximum therapeutic benefit achieved with a daily dose of around 200 μg fluticasone or 400 μg budesonide.3–5 Notwithstanding the marked individual variability in response to ICS treatment,6 these studies would suggest that the 200 μg/day dose of fluticasone or equivalent is likely to represent the preferable level at which to consider the addition of salmeterol in an asthmatic patient not well controlled on ICS. The results of this meta-analysis support this view by showing that the addition of salmeterol to moderate doses of ICS (200 μg/day fluticasone or equivalent) is more effective than increasing the dose of ICS by twofold or more for clinical outcome measures including exacerbations and withdrawals due to asthma. These findings should provide clinicians with greater confidence when deciding the dose of ICS at which to consider adding salmeterol at step 3 in the asthma guidelines.
REFERENCES
Footnotes
-
Competing interests: The Medical Research Institute of New Zealand, the Wellington School of Medicine & Health Sciences, and P3 Research have all received research grants from Astra Draco, GlaxoSmithKline, and Novartis. R Beasley has received fees for consulting and speaking and reimbursement for attending symposia from Astra Draco, and GlaxoSmithKline and Novartis. M Masoli and S Holt have received reimbursement for attending symposia from Astra Draco and Novartis, and S Holt also from GlaxoSmithKline.
-
MM developed the protocol, organised the search, undertook data extraction and wrote the paper. MW was responsible for the data analysis, statistical methodology and manuscript preparation. SH contributed to the study concept and manuscript preparation. RB provided senior oversight for the study and was responsible for the manuscript preparation. MM will act as guarantor for this paper.
Linked Articles
- Airwaves