Article Text

Abstract
Background: Interstitial lung disease (ILD) is characterised by exertional dyspnoea, exercise limitation and reduced quality of life. The role of exercise training in this diverse patient group is unclear. The aims of this study were to establish the safety of exercise training in ILD; its effects on exercise capacity, dyspnoea and quality of life; and whether patients with idiopathic pulmonary fibrosis (IPF) had similar responses to those with other types of ILD.
Methods: 57 subjects with ILD (34 IPF) were randomised to receive 8 weeks of supervised exercise training or weekly telephone support. The 6 min walk distance (6MWD), incremental exercise test, modified Medical Research Council (MRC) dyspnoea score and Chronic Respiratory Disease Questionnaire (CRDQ) were performed at baseline, following intervention and at 6 months.
Results: 80% of subjects completed the exercise programme and no adverse events were recorded. The 6MWD increased following training (mean difference to control 35 m, 95% CI 6 to 64 m). A significant reduction in MRC score was observed (0.7 points, 95% CI 0.1 to 1.3) along with improvements in dyspnoea (p = 0.04) and fatigue (p<0.01) on the CRDQ. There was no change in peak oxygen uptake; however, exercise training reduced heart rate at maximum isoworkload (p = 0.01). There were no significant differences in response between those with and without IPF. After 6 months there were no differences between the training and control group for any outcome variable.
Conclusions: Exercise training improves exercise capacity and symptoms in patients with ILD, but these benefits are not sustained 6 months following intervention.
Trial registration number: NCT00168285
Statistics from Altmetric.com
The interstitial lung diseases (ILDs) are a diverse group of chronic lung conditions characterised by dyspnoea on exertion and poor health related quality of life.1–3 Treatment options are often limited and patients suffer increasing exercise limitation as their disease progresses. Although exercise training effectively improves exercise capacity and health related quality of life in patients with chronic obstructive pulmonary disease (COPD),4 its role in patients with ILD is unclear. Small uncontrolled trials suggest positive effects of exercise training on endurance and quality of life,5 ,6 but more robust evidence of benefit in ILD is lacking.
Current guidelines for exercise prescription in chronic lung disease are based on evidence from studies of patients with COPD7 where respiratory mechanics and peripheral muscle dysfunction are major limitations to exercise capacity.8 ,9 The applicability of such guidelines to patients with ILD is unclear as the physiological basis of exercise limitation differs substantially from COPD. Exercise performance in ILD is closely associated with circulatory impairment10 ,11 and is characterised by exercise induced hypoxaemia that may be profound.12–14 Pulmonary arterial hypertension is also common15 and may worsen with exercise.16 In addition, ILD is a heterogeneous group of diseases. Patients with idiopathic pulmonary fibrosis (IPF) generally demonstrate greater abnormalities of exercise induced gas exchange than those with other forms of ILD.17 ,18 Whether it is safe and efficacious to apply standard exercise training principles to all patients with ILD is unknown. Our aims in this study were therefore to evaluate: (1) the safety of a standard exercise training programme in ILD; (2) the effects of exercise training on exercise capacity, dyspnoea and quality of life; and (3) whether there is a difference in response to exercise training in IPF compared with other ILDs.
METHODS
A two site, randomised, single blinded controlled trial was conducted at the Alfred Hospital and Austin Health, Melbourne, Australia. Symptomatic patients aged over 18 years with documented ILD of any aetiology were invited to take part. The diagnosis of ILD was made according to established criteria. For IPF, the diagnostic criteria were consistent with those outlined in the International Consensus Statement.19
Patients were eligible to participate if they were ambulant and reported dyspnoea on exertion on stable medical therapy. Exclusion criteria were a history of syncope on exertion or any comorbidities which precluded exercise training (such as severe orthopaedic or neurological deficits or unstable cardiac disease). Patients were also excluded if they had participated in a pulmonary rehabilitation programme in the past 12 months. All subjects gave written informed consent and the study was approved by the human ethics committees at both trial sites. Random allocation to exercise and control groups was performed at a central location by an individual unrelated to the study who opened a sealed opaque envelope. Randomisation was performed separately for those subjects with IPF to ensure an even distribution across groups.
Baseline measurements of spirometry, diffusing capacity and plethysmographic lung volumes were obtained. A transthoracic echocardiogram was performed to assess whether pulmonary hypertension was present. Spirometry and diffusing capacity measurements were repeated immediately after the intervention period and at 6 months.
The intervention group attended a twice weekly exercise training programme at the institution where they were recruited for a period of 8 weeks. Training was conducted according to the same exercise prescription principles as those used for COPD.7 The exercise prescription consisted of 30 min of endurance exercise at each session, comprising both stationary cycling and walking training. Initial walking intensity corresponded to 80% of the walking speed achieved on the baseline 6 min walk test. Upper limb endurance training and functional strength training for the lower limbs were performed. Exercise was monitored and progressed by an experienced physiotherapist according to a standardised protocol. Supplemental oxygen was provided during training if necessary to achieve oxygen saturation ⩾85%. Once the subject was established on a supervised exercise regimen, an unsupervised home exercise programme was prescribed with the aim of achieving five exercise sessions per week in total. Subjects were considered to have completed the exercise programme if they attended 12 or more out of a possible 16 supervised exercise sessions. The control group did not receive a supervised exercise training programme but were contacted once a week by telephone during the 8 week period to provide support and general health advice.
The primary outcome, functional exercise capacity, was measured before and after the 8 week intervention period using the 6 min walk test.20 Use of oxygen during the test was standardised and the test was stopped if desaturation to less than 80% occurred, in accordance with a previously described protocol for ILD.21 All follow-up walk tests were conducted using the same flow rate of supplemental oxygen that had been used at baseline. The distance walked in 6 min (6MWD), continuous walk velocity and lowest oxygen saturation were recorded.
Secondary outcomes of maximal exercise capacity, quality of life and dyspnoea were also measured at baseline and after completion of the 8 week intervention. An incremental exercise test was performed on a cycle ergometer in all subjects with baseline oxygen saturation greater than 85%.22 Peak oxygen uptake, minute ventilation, heart rate, workload and duration of the test were recorded. Heart rate and minute ventilation at isoworkload were calculated. Both generic and disease specific health related quality of life were assessed using the Medical Outcomes Study Short Form 36 (SF-36) and the Chronic Respiratory Disease Questionnaire (CRDQ). These questionnaires have previously been validated in ILD.3 Dyspnoea was assessed with the modified Medical Research Council (MRC) Scale.23 Following the intervention period, participants from both groups were asked to make a global rating of change in their walking ability as either “worse”, “about the same” or “better”.24 At 6 months, measurements of 6MWD, dyspnoea and quality of life were repeated. All measurements were obtained by an independent data collector who was blinded to treatment allocation.
The pre-specified sample size was 57 patients based on pilot data collected at our centres in 21 patients with ILD who underwent an exercise training programme. The mean observed change in 6MWD in this pilot study was 38 m (SD 43 m). This sample size provided statistical power of 80% to detect changes in 6MWD (n = 44) and all domains of the CRDQ (n = 57). Data analysis was performed according to the intention-to-treat principle and attempts were made to obtain all available data points from all subjects. In the case of subjects being too unwell to perform exercise tests at follow-up, questionnaire data only were obtained. Subjects were considered to have completed the study if data for at least one outcome was available at 6 months. Missing data were replaced by the last-observation-carried-forward (LOCF) method.25 Subgroup analyses were specified a priori for subjects with and without IPF. To test the robustness of the LOCF analysis, a sensitivity analysis was performed using a conservative method where the observed means from the exercise and control groups were substituted for missing data in the opposite arm.26 The sensitivity analysis confirmed the results of the primary endpoint and hence the LOCF analyses have been reported.
Statistical analysis was performed using a two way analysis of variance to account for group and time interaction (SPSS V.14.0; SPSS Inc). Post-hoc contrasts were specified for differences between groups at 9 weeks and 26 weeks. The significance level was set at p<0.05 and differences between groups expressed as means (SD) or 95% confidence intervals (95% CI).
RESULTS
Between February 2005 and November 2006, 62 patients were screened and 57 patients were randomly assigned to treatment (fig 1). Thirty-four subjects (60%) had a diagnosis of IPF. Of these, 12 subjects had a confirmed pattern of usual interstitial pneumonia on open or thorascopic lung biopsy and the remainder had typical findings of usual interstitial pneumonia on high resolution computed tomography. Four subjects had idiopathic interstitial pneumonias other than IPF (non-specific interstitial pneumonia, cryptogenic organising pneumonia). Of the remaining subjects, 14 had diffuse parenchymal lung disease of known cause (collagen vascular disease, drug or dust related), four subjects had granulomatous lung disease (sarcoidosis, Wegener’s granulomatosis) and one subject Langerhans cell histiocytosis.

Baseline characteristics of the 57 subjects are shown in table 1. There were no differences between the groups at baseline in demographic variables or in the proportion of subjects with IPF. Exercise capacity did not differ between the groups at baseline either in terms of 6MWD or peak oxygen uptake (Vo2peak). The mean 6MWD at baseline in subjects with IPF was 354 (SD 125) m compared with a mean of 431 (117) m in those without IPF (p = 0.02).
Forty-six subjects completed the study (fig 1). There was a significant reduction in FVC over the 6 month study period (mean reduction 220 ml, 95% CI 60 to 380 ml; p = 0.047). There was no difference between groups in the magnitude of reduction in FVC. There was no change in the diffusing capacity for carbon monoxide (Tlco) over the study period. There were two deaths in each group, with one death in the control group prior to 9 weeks and the remaining three deaths occurring during the follow-up period. All deceased subjects had a diagnosis of IPF.
Twenty-four subjects completed the exercise programme (80%). Reasons for non-completion are shown in fig 1. No adverse events were recorded during exercise training.
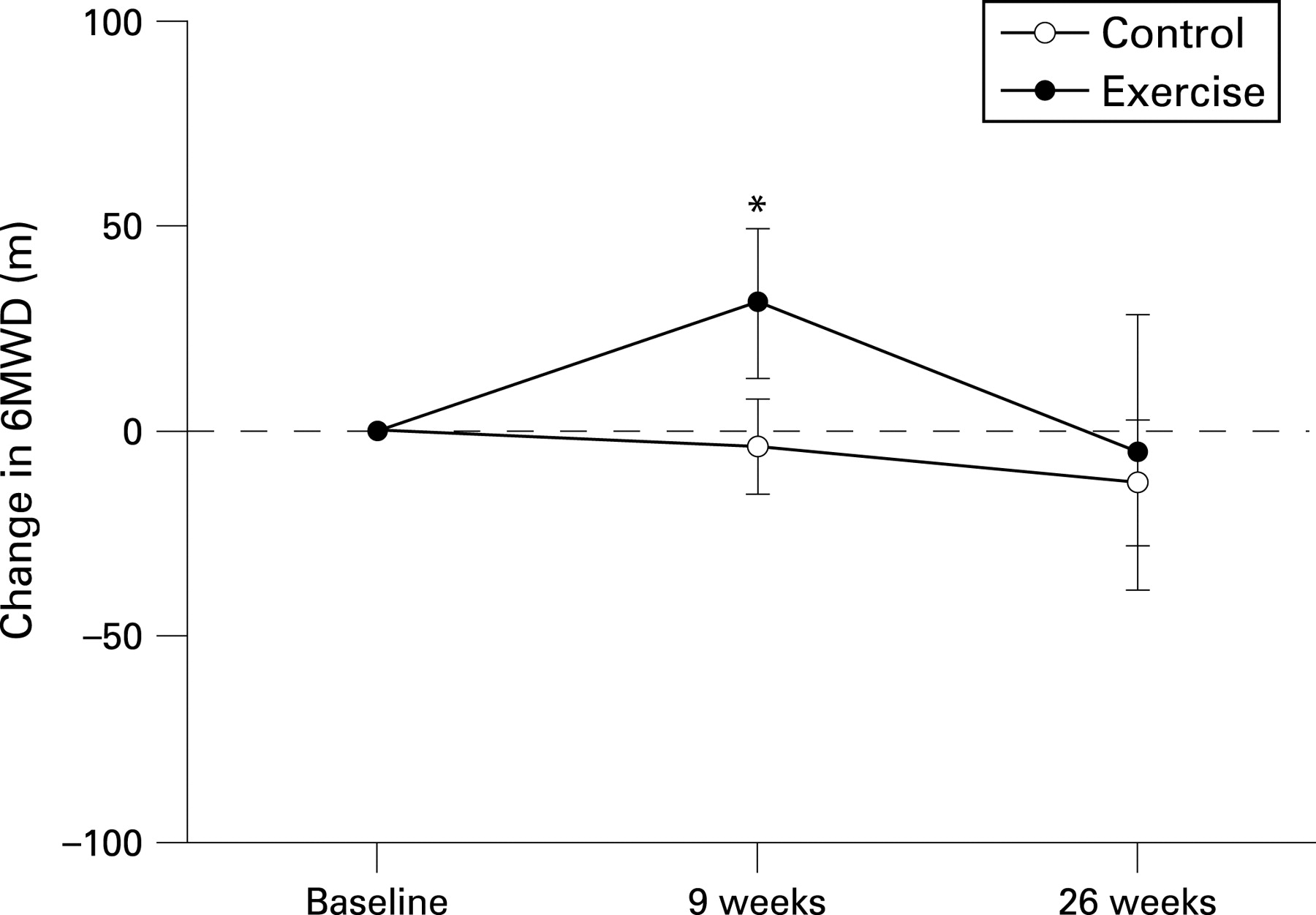
The effects of exercise training on the primary outcome of 6MWD are shown in fig 2. Data were imputed for two patients in each group at 9 weeks; at 6 months, data were imputed for eight subjects in the control group and seven subjects in the exercise group. There was a significant interaction between group and time for walk distance (p = 0.01). The 6MWD improved in the exercise group after the training programme, with a mean increase compared with controls of 35 m (table 2). However, this effect was not sustained at 6 months. A similar interaction was seen between group and time for walk velocity (p = 0.003), with a mean increase of 0.33 km/h in the exercise group following training (table 2) which was not sustained at 6 months. There were no differences between the groups for baseline oxygen saturation or lowest recorded oxygen saturation during the test at any time point.
Cardiopulmonary exercise testing was performed in 52 subjects at baseline, with data imputed at 9 weeks for five subjects in the control group and three subjects in the exercise group. Changes in indices of cardiopulmonary performance are shown in table 2. There were no significant differences between groups in Vo2peak, maximum heart rate or minute ventilation following training. The exercise group showed a reduction in heart rate at maximum isoworkload following training (p = 0.01).
Data for dyspnoea and quality of life outcomes were imputed for two subjects in each group at 9 weeks and five subjects in each group at 6 months. There was a significant interaction between group and time for modified MRC dyspnoea score (p = 0.04) (fig 3). There was a reduction in modified MRC score following exercise training with a mean difference between groups of 0.7 points (table 2). However, this reduction did not persist at 6 months. The CRDQ also demonstrated improvements following exercise training in dyspnoea (p = 0.04) and fatigue (p = 0.009) (table 2). These effects were no longer statistically significant at 6 months (fig 4). There were no statistically significant changes in emotional function or mastery over time. Of the eight domains of the SF-36, only vitality showed gains immediately following exercise training (3.58 points, 0.44 to 5.72; p = 0.005) but this difference was not evident at 6 months.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Global rating of change scores indicated that 68% of participants in the exercise group perceived that their walking ability had improved during the intervention period compared with 20% of participants in the control group. The proportions of improved participants were similar in the subgroup of patients with IPF (73% in the exercise group, 20% in the control group).
Subgroup analyses showed that the mean improvement in 6MWD for subjects with IPF was 25.1 (54.2) m compared with 43.5 (34.2) m in those without IPF; however, there was wide variation in response and this did not reach statistical significance (p = 0.34). The decline in 6MWD from 9 weeks to 26 weeks in those with IPF was −44.2 (75.4) m compared with −20.8 (35.6) m in those without IPF. This difference was not statistically significant (p = 0.65). No significant differences between the response of those with and without IPF were evident for any outcome measure.
DISCUSSION
This study is the first randomised controlled trial of exercise training in ILD. We have shown that exercise training is safe and feasible in this patient group, with programme completion rates similar to those reported in COPD.7 Short term gains in functional exercise capacity and improved symptoms were demonstrated following exercise training using a standard pulmonary rehabilitation training protocol. However, the 6 month follow-up indicates that these benefits were not sustained over time.
Our data showed a mean improvement in 6MWD following exercise training of 35 m. This is a smaller gain than that reported in previous trials of pulmonary rehabilitation performed in patients with COPD, where increases of approximately 50 m were common.4 We used the same exercise training principles that are applied in COPD7 and we have previously shown that our programme achieves gains in 6MWD which exceed the minimal clinically important difference in patients with COPD.27 It therefore seems likely that the magnitude of response to pulmonary rehabilitation is smaller in patients with ILD. Given the progressive nature of many ILDs and the evidence of disease progression in our subjects, a smaller degree of change following exercise training is not unexpected.
The minimal clinically important difference for the 6MWD in ILD has not been defined and the clinical significance of our finding is therefore unclear. Our results could be compared with a recent uncontrolled report of a mean improvement in 6MWD of 49 m following sildenafil therapy in IPF.28 The observed gains in exercise capacity in our trial were associated with improvements in dyspnoea and fatigue on the CRDQ as well as improved global rating of change scores in the majority of participants. This suggests that clinically relevant improvement in symptoms did occur in most participants following exercise training.
The improvements in symptoms and walking distance reported here did not occur as a result of improved maximum exercise capacity. No differences in Vo2peak or any other maximum exercise variables were observed following training. However, the significant reduction in heart rate at maximum isoworkload indicates that a cardiovascular adaptation to training was achieved. This suggests that while maximum exercise capacity may be constrained by the pathophysiology of ILD, submaximal exercise capacity is amenable to training. It is also likely that peripheral muscle adaptation contributed significantly to improved functional capacity. Peripheral muscle weakness is predictive of exercise intolerance in ILD29 ,30 and previous studies in COPD have indicated that much of the improvement in exercise capacity following pulmonary rehabilitation is due to peripheral muscle adaptation.31 ,32 A limitation of this study is that peripheral muscle strength was not measured and future studies of exercise training in ILD should include this variable.
The lack of a benefit of exercise training after 6 months indicates that the observed improvements in exercise capacity and symptoms may only be of short duration. Previous studies have shown that the benefits of pulmonary rehabilitation decline over 6–12 months but differences to the control group are still evident after 1 year.33 Our study was performed in subjects with progressive lung disease, which may explain the faster decline in benefit. The pulmonary rehabilitation literature suggests that health related quality of life is better preserved than is exercise capacity.34 ,35 Our data reflect this pattern; but differences at 6 months were not statistically significant. The number of dropouts at 6 months may have affected these results and is a common difficulty in trials which include participants with IPF.36 Participants in our trial were encouraged to continue with home exercise but did not undertake a formal maintenance exercise programme. It is possible that the benefits of exercise training in ILD may have been longer lasting if a maintenance intervention had been employed; however, at present, the role of maintenance programmes following initial structured programmes remains unclear.37
It is a limitation of this study that the effects of disease aetiology and severity on response to exercise training could not be fully characterised. Interstitial lung disease is a heterogeneous group of conditions with variable disease progression. Although our subjects with IPF appeared to have smaller gains in exercise capacity and health related quality of life than those with other forms of ILD, our study was not powered to adequately assess this outcome. Our sample included subjects with a wide range of disease severity, with diffusing capacity for carbon monoxide ranging from 19% to 75% predicted and right ventricular systolic pressure ranging from 16 to 80 mm Hg. The small sample size did not permit analysis of the effects of disease severity on outcomes of exercise training. Further research with larger samples is needed to address the effects of aetiology on response to training and to establish whether there is an optimal time in the disease course at which exercise training should be offered. This is particularly important for patients with IPF, where the prognosis is poor and the burden of care must be carefully considered.
Treatment options for ILD are limited. Available drug therapy has significant toxic side effects and may not be suitable for many patients. There is no evidence that current drug therapies for IPF can improve quality of life and symptoms.38 In this setting, the modest improvements and absence of side effects associated with exercise training may be of importance to some patients. The short term beneficial effects of exercise training on dyspnoea and 6MWD, variables which are important to prognosis,1 ,2 suggest that further investigation of exercise training is warranted in larger trials.
In conclusion, exercise training in interstitial lung disease is safe and results in short term improvement in functional exercise capacity, dyspnoea and quality of life. These benefits are no longer evident at 6 months. Exercise training may be considered in patients with interstitial lung disease of any aetiology if dyspnoea is associated with diminished functional capacity.
REFERENCES
Footnotes
Funding: This study was funded by the Victorian Tuberculosis and Lung Association.
Competing interests: None.
Ethics approval: The study was approved by the human ethics committees at the Alfred Hospital and Austin Health, Melbourne, Australia.
Linked Articles
- Airwaves