Article Text

Abstract
Objectives To ascertain whether the use of oral glucosamine influences symptoms or functional outcomes in patients with chronic low back pain (LBP) thought to be related to spinal osteoarthritis (OA).
Design Systematic review of randomised control trials. Searches were performed up to March 2011 on Medline, AMED, CINHAL, Cochrane and EMBASE with subsequent reference screening of retrieved studies. In addition, the grey literature was searched via opensigle. Included studies were required to incorporate at least one of the Cochrane Back Pain Review Group's outcome measures as part of their design. Trials with participants over 18 years with a minimum of 12 weeks of back pain, in combination with radiographic changes of OA in the spine, were included. Studies were rated for risk-of-bias and graded for quality.
Results 148 studies were identified after screening and meeting eligibility requirements, and three randomised controlled trials (n=309) were included in the quantitative synthesis. The review found that there was low quality but generally no evidence of an effect from glucosamine on function, with no change in the Roland-Morris Disability Questionnaire score in all studies. Conflicting evidence was demonstrated with pain scores with two studies showing no difference and one study with a high risk-of-bias showing both a statistically and clinically significant improvement from taking glucosamine.
Conclusions On the basis of the current research, any clinical benefit of oral glucosamine for patients with chronic LBP and radiographic changes of spinal OA can neither be demonstrated nor excluded based on insufficient data and the low quality of existing studies.
- glucosamine
- facet joint osteoarthritis
- spinal osteoarthritis
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
The current study examines and evaluates the evidence for the use of glucosamine in back pain.
Key messages
-
There is insufficient evidence to either confidently demonstrate or exclude a clinical benefit of glucosamine for spinal osteoarthritis.
-
The use of more objective outcome measures, longer follow-up periods and a clearer understanding of the possible biochemical model for glucosamine's mode of action in back pain may enable more definitive conclusions to be drawn.
Strengths and limitations of this study
-
The review incorporated several databases and utilised systematic and vigorous search strategy. Limitations included the exclusion of articles not published in English and the attempted comparison of studies with participants with different demographics such as age.
Introduction
Rationale
Low back pain (LBP) affects around one-third of UK adults each year.1 ,2 Around 20% will consult their general practitioner (GP), making it one of the commonest presentations seen in primary care.3 Additionally, there are considerable financial consequences associated with back pain, with previous estimates of direct healthcare costs in the UK amounting to over £1.6 billion and indirect costs from informal care and loss of productivity to the economy of £10.7 billion.4
Osteoarthritis (OA) is a highly prevalent degenerative joint condition that the WHO Scientific Group on Rheumatic Diseases estimates is the cause of significant clinical problems in at least 10% of patients who are 60 years or older.5
OA can affect several parts of the body including the spine. Within the spine, OA affects the vertebral facet joints6 and may occur with or without the presence of LBP.7
Borenstein8 suggested that OA may cause LBP; however, this relationship is complex and controversial. Some of the evidence supporting a link between spinal OA and LBP comes from early studies which showed improved back pain following intra-articular or peri-articular joint injections.9––11 However, it is apparent that not all patients with LBP will have symptoms that correlate with severity of radiographic OA changes on imaging.7
A further degenerative process can be found in the spine in the form of intervertebral degenerative disc disease (DDD). A recent twin study demonstrated the presence of lumbar degenerative discs on MRI to be a major determinate feature of patients with LBP.12 Although the prevalence of DDD and facet joint OA correlates,13 it is unclear whether they are independent of one another or whether they are different ends of the spectrum of the same pathological process.
Pharmacological therapies are the most frequently used intervention for LBP;14 however, serious side effects associated with the long-term use of some medications such as non-steroidal anti-inflammatory drugs (NSAIDS) has led patients to seek alternative medicines such as glucosamine.
Glucosamine is available to purchase as a food supplement and is gaining popularity among patients in the UK for the relief of knee and hip pain associated with osteoarthritis; however, more than 25% of patients have tried glucosamine for LBP.15
Glucosamine is a naturally occurring amino monosaccharide and is a precursor for glycosaminoglycans, a major component of joint cartilage and synovial fluid,16 and this forms the basis of the rationale for its use in OA. Glucosamine is available in over 50 different preparations most commonly in the form of glucosamine sulfate and hydrochloride.17
Glucosamine hydrochloride (Alateris) is the only preparation licensed for medical use in the UK and the license is restricted to the symptomatic relief of mild to moderate knee OA. Despite its being a licensed drug, there is less evidence for its use compared with glucosamine sulfate and neither are currently recommended by the National Institute for Health and Clinical Excellence (NICE).18
Several trials and systematic reviews have looked into the use of glucosamine in knee and hip arthritis. A Cochrane review identified 16 double-blind randomised controlled trials (RCTs) and concluded that there was good evidence that glucosamine is both effective and safe in treating OA, but this did not assess spinal OA19 This review was updated and failed to show a uniformly positive conclusion, if only high-quality studies were included.20 Analysis restricted to studies with adequate allocation concealment failed to show any benefit of glucosamine for pain, function and stiffness based on Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) used to assess pain, stiffness and function in patients with hip and knee OA. However, the review also assessed pain and function on the Lequesne index, which did reveal an improvement after glucosamine when compared with placebo. The disparity between these findings remains unexplained by the authors; however, a study that compared and tested the validity of WOMAC and the Lequesne index found that although both measures show internal validity when assessing function in hip and knee OA, only WOMAC is consistently reliable when assessing symptoms such as pain.21
Given the lack of conclusive evidence regarding an improvement in LBP from glucosamine and, at present, no recommendations from NICE, the indications for using glucosamine remain controversial for clinicians and patients.
The reviews so far have focused on trials looking at the use of glucosamine in hip and knee OA.22 The current study has been undertaken to provide an up-to-date systematic review of the evidence for the use of glucosamine in LBP.
Objective
To systematically search and assess the quality of the evidence of the efficacy of glucosamine on LBP symptoms in patients diagnosed with spinal facet joint OA or DDD.
Methods
Criteria for considering studies for this review
Types of studies
Only RCTs were considered for this review as randomisation ensures that patients in the treatment and control groups are comparable from the start. In the hierarchy of study designs, RCTs and systematic reviews are considered the highest level of evidence.23 At least 1 day of follow-up was required to ascertain any effect of an intervention. RCTs were included if they: (1) evaluated the efficacy and toxicity of glucosamine in OA, (2) were placebo-based or comparative studies, (3) were open-label, single-blinded or double-blinded, (4) evaluated glucosamine-only or combination preparations, (5) utilised oral administration of glucosamine as this is the route which will be used by the majority of patients.
Types of participants
Participant inclusion criteria for this review included: adult participants (≥18 years), with chronic back pain (≥12 weeks) and signs of spinal OA. As there are no consensus guidelines about what constitutes a diagnosis of OA in the spine, any radiographic changes consistent with OA were included. A variety of radiographic grading systems have been proposed, but there is no single global staging system suitable for the assessment of OA at all sites.24
The exclusion criteria were: trials that included subjects with specific LBP caused by other pathologies such as vertebral canal stenosis, ankylosing spondylitis, scoliosis and coccydinia and trials that looked at OA at multiple sites but did not separate the data from the different sites, making conclusions regarding changes in spinal symptoms difficult.
Types of interventions
Both placebo-controlled trials and comparative studies were eligible. The types of comparison considered appropriate were conventional therapies used for OA such as physical therapy, analgesics and anti-inflammatories.
Types of outcome measures
For inclusion, at least one of the following outcome measures recommended by the Cochrane Back Review Group (CBRG) had to be observed: (1) pain intensity, for example, a visual analogue scale, (2) reliable and valid measure of functional status or disability, for example, the Roland-Morris Disability Questionnaire (RMDQ),25 ,26 (3) perceived recovery, (4) return-to-work status, (5) structural benefits measured by radiography, (6) adverse effects. The primary outcomes for this review were pain and functional status. The timing of the measured outcomes had to be explicitly described.
Search methods for identification of studies
All the three authors are practicing clinicians in the UK and have either completed or are undertaking higher research degrees.
The search strategy was formulated jointly by the first two named authors. Retrieval of searches, reference screening and subsequent data synthesis was subsequently performed independently. Differences were resolved after discussion with the third author. The search was conducted up to March 2011 and included the grey literature, searched via opensigle. Papers not published in English were excluded. By searching MEDLINE (medical, nursing and biomedical journals), it was anticipated that approximately half of the available RCTs would be identified; therefore, a subsequent search of EMBASE (biochemical and pharmaceutical journals) would ensure a comprehensive search as there is little overlap between these databases and in the field of LBP, EMBASE has been shown to retrieve more clinical trials.27 Searching AMED and CINHAL would cover complementary medicine and allied health journals, while including Cochrane enabled high-quality evidence from RCTs and systematic reviews to be included. References of relevant studies were screened to identify additional studies.
The electronic search strategy outlined in online supplementary appendix 1 was developed in MEDLINE and adapted for the other databases. The search was developed by reviewing relevant articles in the area of back pain and OA and combining search terms used in these studies.
Risk-of-bias assessment and quality
The risk-of-bias was assessed using the criteria advised by CBRG.27 Each criterion was scored as yes, unclear or no, where yes indicated that the criterion had been met. Studies are rated as having a low ‘risk-of-bias’ when at least 6 of the 12 CBRG criteria have been met with no serious flaws.
Data extraction
Data were recorded onto a standardised form and described the main trial characteristics, patient demographics, interventions, comparisons, outcomes, analysis, results and assessment of trial quality (tables 1 and 2).
Characteristics of studies included
Methodological quality assessment and risk-of-bias
Quality of the evidence
Grades of Recommendation, Assessment, Development and Evaluation criteria were used to evaluate the overall quality of the evidence. This is recommended by the Cochrane Handbook to rate the quality of evidence for each important patient-centred outcome as it goes beyond the reporting of quantitative analysis. The quality of evidence was based on five domains: limitations of the study design, inconsistency, indirectness (inability to generalise), imprecision (insufficient or imprecise data) of results and publication bias across all studies that measure that particular outcome.28 The overall quality was considered to be high when at least 75% of RCTs with no limitations of study design had consistent findings, direct and precise data and no known or suspected publication biases.27 The grades of quality of evidence are outlined in online supplementary appendix 2.29
Results
Description of studies
Study selection
Studies were identified through the following databases: MEDLINE (11), EMBASE (53), Cochrane library (84) (Cochrane reviews (10), other reviews (7), clinical trials (67)). Three studies were included (table 1). Reasons for exclusion are outlined in figure 1. Owing to differences in the study design of included trials, meta-analysis was not attempted.
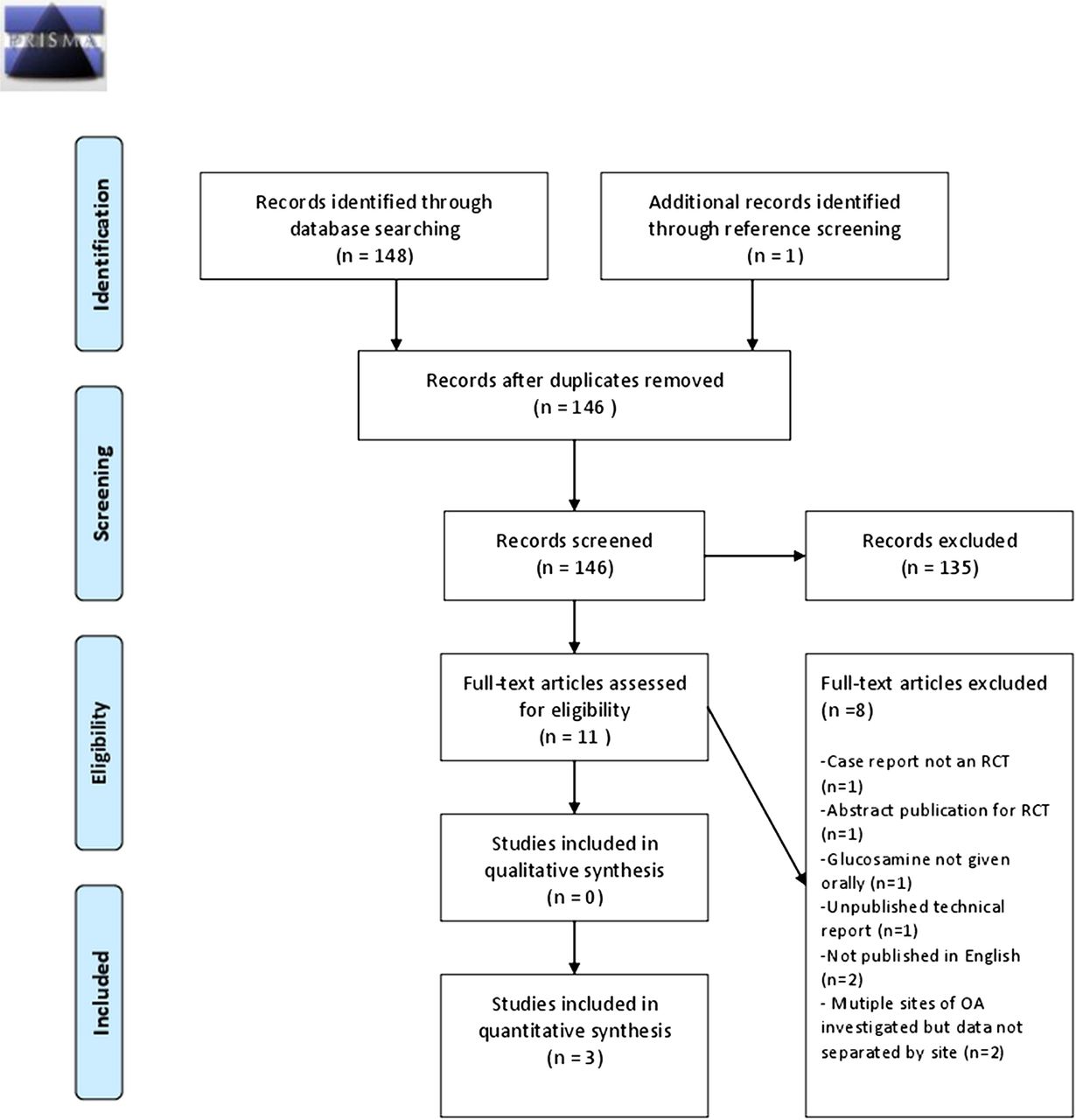
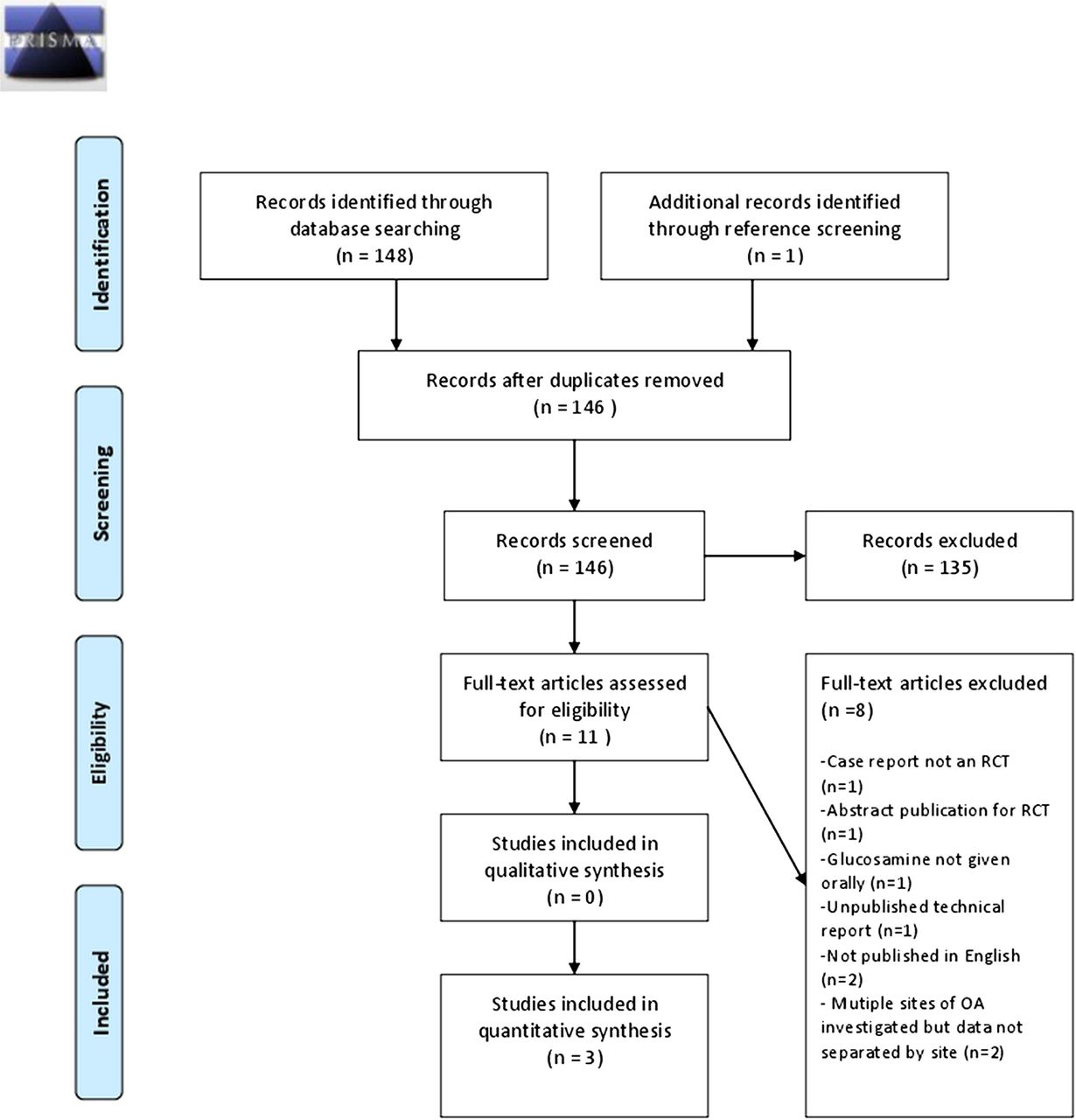{kind=link}
Flow diagram of inclusion and exclusion of articles for glucosamine use in spinal OA (PRISMA 2009 Flow Diagram)40
Risk-of-bias in included studies
The risk-of-bias assessment is shown in table 2. Although all studies were described as randomised, only two described adequate randomisation.30 ,31 One trial was open-label and did not report compliance.31 One trial had a 20% dropout rate.32 All trials had similar groups at baseline, timings of outcome assessments and cointerventions in both groups.
From this assessment, two studies have been rated as having a low risk-of-bias. The one study rated as a high risk-of-bias scored 6, but its open-label design was considered to be a significant methodological flaw.
Effects of intervention
Tables 3⇓⇓–6 summarise the findings with respect to the main outcomes measured. For pain, the two studies with a low risk-of-bias failed to show any significant improvement with glucosamine compared with placebo, while the one study with a high risk-of-bias did show a significant difference with glucosamine compared with no glucosamine.
Key findings: effect of glucosamine on back pain outcomes
Key findings: effect of glucosamine on function outcomes
Key findings: adverse effects
GRADE evidence profile
Back function/disability was measured by the Owestry Disability Index (ODI) and RMDQ, both validated tools26 ,33; there was no significant difference in the RMDQ scores with glucosamine as an intervention. The study with a high risk-of-bias demonstrated a statistically significant difference in the ODI score reduction for the glucosamine group, although this difference was small.31
With respect to adverse effects, one trial revealed ∼30% of participants experienced adverse effects irrespective of whether they were in the placebo or glucosamine group.30
Other outcomes that were considered but not across all trials included an assessment of quality-of-life measured by the Euro-Qol-5 Dimensions index and overall health status measured by EQ-VAS.30 There was no significant difference found between glucosamine and placebo with these outcomes.
One study used several assessments that were totalled to provide an overall summary score.32 In addition to measuring pain and function, physical examination scores and running times were assessed. There were no statistically significant changes in the LBP group when considering the overall summary score or individual outcome measures.
None of the studies looked at radiographic changes in association with glucosamine use.
Discussion
In this review, three RCTs were included that evaluated the effectiveness of glucosamine as an intervention for chronic LBP associated with spinal OA.30–32
Overall, the review found that the limited number of studies had methodological deficiencies. The studies did not demonstrate a clear beneficial effect of using glucosamine for LBP due to OA.30 ,32 One study, however, showed a statistically significant difference in the ODI score reduction for the glucosamine group,31 although this difference was small and does not appear to reach the minimally clinical important difference (MCID) alluded to in previous research.34
There was conflicting evidence regarding the effect of glucosamine on pain scores. Two studies showed no statistically significant difference on pain scores between the intervention and placebo groups.30 ,32 One study did show a statistical and clinically significant reduction in pain scores for those taking glucosamine.31 While this study had significant methodological shortcomings that are discussed in the next section, this alone may not completely explain differences when compared with the two other studies. A possible reason was that the study recruited older patients with a mean age of 64 compared with a much younger demographic in the remaining two studies. Facet-joint OA is known to become more prevalent with age,13 and therefore the proportion of patients with pain related to facet joints as opposed to discogenic pain may have been higher. This, combined with a theoretical possibility that glucosamine may predominantly affect articular cartilage, as opposed to intervertebral discs, may lead to an under-representation of the effect of glucosamine in studies with a younger cohort.
Methodological considerations
There were several factors that contributed to the very low-quality or low-quality assessment for the main outcomes measured in the trials. The results of one study31 in particular, which found positive effects of glucosamine on both pain and function, appear to contradict the findings of the other two; however, this may be partly explained by its limitations. A key limitation was its open-label design. Since the participants and clinicians were aware of the group allocation, bias was introduced.
Another study had unclear details about its randomisation.32 Blinding and randomisation decrease the likelihood of selection and performance bias, which would affect the internal validity of the study.35 This same RCT employed a crossover design, which may intrinsically have introduced bias if the 5-week washout period employed was too short.
To minimise the attrition bias, the dropout rate should be described and be acceptable with all the randomised patients analysed in the group to which they were allocated, by an intention-to-treat analysis (ITT).35 One trial did not employ an ITT analysis and compliance was unclear.31
There are difficulties in how the trials can be directly applied to the general population and this adversely affects their relevance to practice and external validity. One trial used patients from the US Navy diving and special warfare community who have a history of high-activity levels and unique occupational exposures. They were also all men; hence, the results may not be generalisable.32 This study used a mixed population of both knee and back-pain patients, with some participants having both knee and back pain. The proportion of patients in each group was described and the data were separated.
Despite the fact that the risk-of-bias was low in two studies, the studies collectively showed flaws regarding the concealment of treatment allocation, adequate randomisation, compliance and dropout rates. The review findings were significantly influenced by these shortcomings despite the fact that the study by Wilkens et al was of a high quality and well designed. The quality of future RCTs needs to be improved to reduce bias in future reviews.
Review strengths and limitations
The selection procedure and literature search utilised in this review may have introduced bias.
The selection criteria did not place limits on the ages of participants and as the pathology of LBP may change with age, direct comparisons between studies of patients with different patient demographics need to be taken with caution.
Relevant, unpublished trials may have been omitted and as these are likely to be small studies without positive results, this may lead to publication bias. Studies not published in English were excluded and may also have introduced bias. Utilising references of the included trials to identify other studies may have also led to an over-representation of positive studies.
The search strategy, however, was vigorous with several databases utilised, in addition to reference screening of included studies, which ensured that the omission of relevant studies was minimised.
Implications for health practice
LBP is extremely prevalent with considerable financial consequences.4 OA accounts for a significant proportion of LBP seen by GPs and secondary care clinicians. Current treatment options such as NSAIDs and surgery have some potentially serious adverse effects .Therefore, alternative treatments such as glucosamine, which may provide a possible solution to this problem, seem attractive.
Global sales of glucosamine reached almost £1.3billion in 2008.36 Currently in the UK, glucosamine is available as a food supplement and can be prescribed for knee OA. The evidence for its use in back pain is conflicting; it is therefore imperative that a consensus based on sound clinical evidence is reached to justify this immense cost to the public.
This review helps to clarify the existing evidence for the use of glucosamine in back pain, which will be of particular relevance to patients and clinicians considering using glucosamine.
The current review has demonstrated that if only the studies with a low risk-of-bias are considered, there is no evidence of a significant difference between glucosamine and placebo for pain or pain-related disability associated with OA in the lower back.
The mechanism by which glucosamine may exert its effect is poorly understood. Wilkens et al, previously proposed that glucosamine may reduce LBP by inhibiting interleukin (IL)-1β, which is present in lumbar discs and facet joints. This mechanism is purely theoretical with no conclusive evidence demonstrating a direct pharmacological effect on the spine. The lack of a sound scientific rationale for the use of glucosamine in LBP makes it difficult to successfully design a study to prove any clinical benefit that it may have. In addition, there is much debate as to the relationship between LBP and spinal OA findings. Not all patients with LBP have spinal OA and vice versa; however, most studies assume they are correlated.
All the studies included in the review had limitations. All were single centre trials and two had small sample sizes. There were methodological differences in randomisation, blinding, allocation concealment and varying outcome measures. Inclusion criteria varied between trials; some looked at both facet joint OA and DDD. These two conditions do not necessarily represent the same pathological process. In addition, the method for diagnosing OA differed as there is no existing consensus or criteria for diagnosis. Back pain is complex and while spinal OA may cause LBP, several other structures may be responsible and pathologies may coexist.
It is possible that glucosamine may work better in more severe disease, as has been suggested with knee OA.37 All the studies reviewed had varying severities of OA symptoms required for inclusion. This limits the conclusions that can be made as the studies did not separate the data for different levels of severity in the analysis.
OA is a chronic disease and patients taking supplements such as glucosamine may do so for several years. Follow-up periods for the trials varied from 8 weeks to 1 year. Glucosamine may take longer than this to have an apparent affect. A case report revealed an improvement in the structural quality of disc cartilage on MRI in a patient taking glucosamine over a 2-year period.38 The patient's symptoms only began to improve at 6 months and continued until the end of the study period. None of the studies in this review looked at objective radiographic changes as an outcome and while there are obvious limitations to drawing any broad conclusions from a single case report, this provides an argument for a longer follow-up RCT and more objective outcome measures.
A strength of this review is that it contained several placebo-controlled RCTs. One especially well-designed study clearly showed that patients treated with glucosamine for 1 year, who had a combination of chronic LBP and either or both facet-joint OA and DDD, had no difference in pain or disability when compared with placebo.
An important factor to consider when assessing the relevance of trial data to everyday practice is the generalisability or external validity of the studies. The current review included one study which used a relatively young cohort of male patients who were from a US Navy diving and special warfare community with a history of high-activity levels and unique occupational exposures. This is not the profile of a typical OA patient a doctor would see in general practice.
An important distinction is between statistical significance and clinical relevance of findings. One study showed a statistically significant difference in pain-related disability on ODI; however, the difference was very small and may not have represented a clinically relevant change.31 Currently, there is consensus regarding minimal clinically important changes for pain and function (measured by RMDQ, not ODI) in back pain.27 For LBP, 30% on VAS/NRS for pain is considered to be clinically significant and 2–3 points (8–12%) on the RMDQ for function is also considered as clinically significant.39
Glucosamine may be viewed as a relatively safe medication; however, the current review nonetheless highlights a high incidence of adverse effects and although these were mild, it is an important consideration when recommending it.
On based on the current evidence explored in this review, there is insufficient evidence to either demonstrate or exclude a clinical benefit of glucosamine for spinal OA. Using more objective measures such as radiography to look at any change in OA progression, refining the study inclusion criteria, providing longer follow-up periods and trying to establish a clear biochemical model for glucosamine may enable more definitive conclusions to be drawn so that clinicians can confidently advise their patients based on the best available evidence.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendices
Footnotes
-
Contributors All the listed authors fulfil the ICMJE guidelines for authorship. The first author (RS) conceptually designed the study, performed the searches and data synthesis and provided the initial draft for publication. NS performed the database searches and also aided the data synthesis and prepared the manuscript for publication. MA contributed to the data analysis and revised the manuscript prior to submission. All authors have read and approved the final manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.