





Abstract
Aggregate monthly notifications of incident sputum smear-positive tuberculosis (TB) in Mongolia, stratified by sex and age groups, were analysed separately for Ulaanbaatar, Mongolia, and the rest of the country for the 9-yr period from 1998 to 2006. TB notifications were compared with ambient surface temperature.
More than twice as many TB cases were notified in the peak month (April) compared with the trough months (October–December), paralleling the temperature curve. The fluctuations recurred consistently over the entire observation period, were identical in the capital compared with the rest of the country, and were independent of age and sex.
TB notifications parallel the temperature amplitudes and have a magnitude not reported elsewhere. We hypothesise that the influence of temperature on life either indoors or outdoors is consistent with the transmission probability of Mycobacterium tuberculosis and the subsequent delay to disease recognition and notification with the incubation period, possibly co-determined by other factors, rather than accessibility to services.
Mongolia is a vast country and its close to 1.6 million square kilometres are populated by just 2.6 million inhabitants 1. Its geographical location, a landlocked and mountainous territory with an average altitude above sea level of 1,500 m, gives it a pronounced continental climate. Average temperature differences between trough and peak months are close to 40 °C. The average monthly temperature rises above 0 °C during only 7 months, and yet the country has 250 days of sunshine per year.
In 2007, the notification rate of all new tuberculosis (TB) cases from Mongolia was 166 per 100,000 population, of which 44% were sputum smear-positive pulmonary, 15% other pulmonary and 42% extrapulmonary cases 2.
Seasonal fluctuations in TB notifications have been reported from a number of settings 3–6, offering a variety of possible explanations for the findings. Seasons may affect TB transmission and case notifications in a variety of ways. Temperature and precipitations determine the amount of time spent indoors, and thus the transmissibility of Mycobacterium tuberculosis. Seasons shape workload and health-seeking behaviour, as precipitation may hinder access to healthcare facilities when TB causes ill-health, and season-dependent nutrition and metabolism may influence response to infection with M. tuberculosis.
Fluctuations in TB case diagnosis impact on the functionality of the national TB programme. Thus, it appeared to be opportune to study the extent to which seasons are mirrored in TB notifications in Mongolia.
METHODS
The National Communicable Disease Center, Ulaanbaatar, Mongolia, collects TB case information according to international recommendations 7. For the purpose of our study, only cases of pulmonary TB bacteriologically confirmed by sputum smear microscopy were considered. A uniform national reporting system had become functional from 1998 onwards, and the 9-yr period from 1998 through to 2006 was included in our analysis. Aggregate case data, stratified by month and year of report, standard age groups, sex, and whether they were reported from the capital or from the rest of the country were available for this analysis. For the analysis, most calculations were carried out using a spreadsheet (Microsoft Office Excel 2003; Microsoft Corp., Redmond, WA, USA). Where indicated, a graphical statistical package (SigmaPlot 11.0; Systat Software, Inc., Chicago, IL, USA) was utilised for graphing and regression analysis.
Information on surface temperature was obtained from the National Center for Meteorology, Ulaanbaatar. Data were obtained in a spreadsheet as monthly average surface temperatures in the 21 provinces and the capital Ulaanbaatar for the 21-yr period from 1983–2003. The temperatures were summarised as monthly averages over the 22 areas and the 21 yrs of observation. Data on TB were available as aggregate data in a spreadsheet, with each cell containing a stratum of the number of cases by age, sex, month and year for Ulaanbaatar and the rest of the country. Due to the aggregate nature of the data, stratification beyond what was available was not possible, data could only be further collapsed into relevant groupings and regression analysis only performed where deemed appropriate. All data on TB were restricted to sputum smear-positive pulmonary TB, largely because the diagnosis of other forms is uncertain in a country where culture facilities are poorly developed and the proportion of cases other than sputum smear-positive ones was very small.
RESULTS
During the 9-yr period, a total of 14,905 sputum smear-positive TB cases were reported, with an annual average of 1,656 cases and a monthly range from -36% (in December) to +51% (in April) of the monthly average of 138 cases (table 1⇓). The seasonal fluctuations were large, with two- to three-fold differences between trough and peak levels (fig. 1⇓). There was an average annual increase in notified cases of ∼6% over the observation period.

Seasonal variations in notification of sputum smear-positive tuberculosis in Mongolia, 1998–2006. ––––: reported sputum smear-positive tuberculosis cases by month and year; ○: average monthly cases in each year; ----: regression through average monthly cases in each year.
Reported sputum smear-positive cases by sex, month and year in Mongolia, 1996–2006
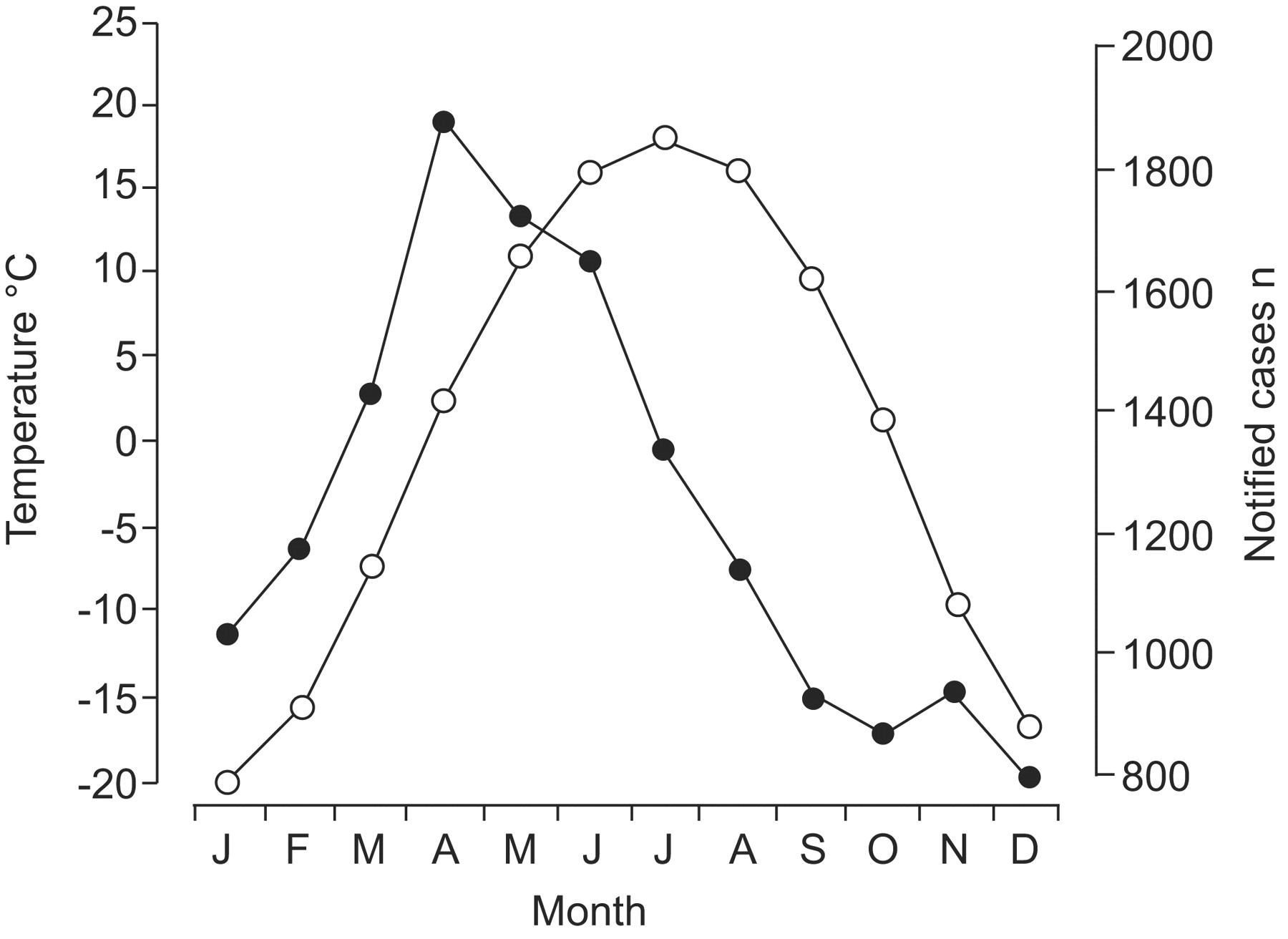
Within the calendar year, the largest monthly number of cases was reported in April and the smallest from September through December. Case notifications at the peak and subsequent to the peak preceded the temperature course by ∼3 months (fig. 2⇓). Almost throughout the year, the shape of the case curve was∼3 months ahead of the temperature curve. Reported cases declined after the April peak through to September, but then remained relatively level through the end of the calendar year while temperatures continued to drop throughout January of the subsequent year.

Relative changes in monthly tuberculosis case notifications (•) and ambient temperature (○), forced to scale to allow comparison in Mongolia, in combined cases from 1998–2006.
More cases were reported among males than among females (female-to-male ratio 0.85). If grouped into three similarly sized tiers, female cases predominated among those aged up to 24 yrs (female-to-male ratio 1.12), males in the 25- to -34-yr-old age group (female-to-male ratio 0.92), and the number among males far exceeded that among females in those aged ≥35 yrs (female-to-male ratio 0.63). While among the youngest of these groups, there appeared to be an increase in the preponderance of females from December–August, no such pattern was discernible among the other two age groups (fig. 3⇓).

Female-to-male tuberculosis case ratio by age group and month in Mongolia, in combined cases from 1998–2006. ······: 0–24 yrs, 4,795 cases; – – –: 25–34 yrs, 4,612 cases; –––––: ≥35 yrs, 5,498 cases.
The seasonal variation was similar in all age groups. The approximated mean age stratified by sex did not show any apparent monthly variation (data not shown).
Of the 14,905 notified sputum smear-positive cases, 52.0% (7,758) were notified from Ulaanbaatar, and the remaining from the mostly rural areas of the country. The seasonal fluctuations in Ulaanbaatar were similar to those in the rest of the country, with very few exceptions, for example, in the first observation year (fig. 4⇓). Sometimes the amplitude of fluctuation was even larger, as in the last observation year. A stratification by sex did not show any difference between Ulaanbaatar and the rest of the country.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reported sputum smear-positive tuberculosis cases by month for Ulaanbaatar (––––) versus the rest of the country (-----), in Mongolia during 1998–2006.
DISCUSSION
TB increased annually by ∼6% over the observation period. The reasons for this observation remain elusive and may be attributable to improved surveillance, demographic changes, an actual deterioration of the epidemiological situation, or a combination of all factors. While case notifications increased in all of the country over the observation period, they were particularly large in Ulaanbaatar, probably reflecting the increasing urbanisation and migration from rural areas to the capital. Calculations by the World Health Organization using United Nations population data suggest that the notification rate in Mongolia has remained unchanged between 1990 and 2007 2, which would suggest that a major contributor to the increase in case notifiactions in Ulaanbaatar is related to the increase in the population.
While seasonal patterns have been reported from other areas 3–6, the data on reported TB cases from Mongolia present, to our knowledge, one of the most pronounced seasonal variations on a national scale reported in the English literature. The finding is consistent for every year during the observation period from 1998–2006.
The principal explanatory hypothesis we offer for this observation is that transmission probability is highest in the coldest months due to long periods of containment indoors. The often insidious initial symptoms subsequent to the incubation period may not immediately result in seeking medical assistance, as the warming period also coincides with the busiest period during the year, at least for the rural population.
The present analysis was restricted to sputum smear-positive cases of TB. While the most appealing indicator for TB resulting from recent transmission is TB in children, such cases are difficult to determine because diagnostic certainty is unavailable in the majority of them. Furthermore, pulmonary TB that is not sputum smear-positive is still rarely diagnosed in Mongolia, making up just 15% of all new notified cases 2, suggesting an important extent of undiagnosed cases.
Mongolian life is shaped by the large variations in ambient temperature. While close to 40% of the Mongolian population now lives in the capital, Ulaanbaatar, a similar percentage of the country's population is rural 1 and to a large extent nomadic. During the warmer months, much time in rural areas is spent outdoors, where the probability of transmission of M. tuberculosis is small 8, as dissipation of tubercle bacilli is immediate and rapid killing of bacilli assured by 250 days of sunshine per year 9. Transmission opportunity indoors is an altogether different matter, particularly where, traditionally, the single, tightly sealable one-room ‘ger’ assembles the entire family and is shared day and night by the inhabitants. Should a case arise in the cold months, transmission to family members is greatly facilitated, resulting in new and re-infections, both of which have been shown to be important contributors to morbidity in both low- 10 and high-incidence 11 settings.
The median interval between infection with and specific readily observable immunological response to M. tuberculosis is ∼7 weeks 12. Thus, the earliest manifestation of clinically manifested TB would be expected to commonly follow with a delay of ≥2 months following infection. The end of February through to April is the birthing season for the five types of livestock animals (camels, horses, cattle, goats and sheep) most commonly reared in Mongolia. These account for a staggering 35 million animals 1, and this time of the year is thus the busiest period for the rural population. It is conducive to assume that the initially often mild symptoms attributable to the onset of clinically active TB are neglected during this time and a visit to a healthcare facility may be postponed.
While the harsh climate and precipitation in winter months may impede travel and thus reduce timely accessibility to healthcare, it is noteworthy that the pattern of seasonality was precisely the same in Ulaanbaatar as compared with the rest of the country. As healthcare services tend to be generally more accessible in urban than rural areas, this finding would argue against a major influence of the season on accessibility to services. That acute onset illnesses result in prompt seeking of medical attention during the coldest months has been amply documented in the surveillance network of influenza in Mongolia 13.
Protection against progression from latent infection to overt clinical TB might also be affected by the season through factors affecting immunological response. Among these, the role of vitamin D has long received considerable attention. While there is no evidence that rickets, the most serious manifestation of vitamin D deficiency, increases the risk of TB, administration of cod-liver oil to treat TB was nevertheless suggested as early as 1849 14. In 1903, Niels Ryberg Finsen was awarded the Nobel Prize for his work on treatment of lupus vulgaris with high-intensity light, inducing moderate sunburns 15. Vitamin D is marginally present in most diets. Skin conversion to the hormonally active form through solar irradiation is dependent on atmospheric ultraviolet B absorption. Although sunshine is abundant in Mongolia, the required clothing, especially in the cold season leaves virtually no exposed skin. Unsurprisingly, vitamin D deficiency and rickets are rampant in Mongolia 16. The hormonally active form has, in addition to its calciotropic effect, a critical regulatory role in immune functions. Seasonality of TB with winter troughs and summer peaks has been reported from the UK and Hong Kong, which is reversely associated with vitamin D seasonal variation 3, 4, 17. To explain “summer TB”, a possible delayed effect of vitamin D deficiency on progression to TB must be postulated. The lower vitamin D levels found in TB patients may be less related to diet or skin pigmentation, but rather to an abnormal handling of the vitamin 18. Thus, the actual role of vitamin D in protection against TB remains elusive despite many speculations to the contrary 17, 19. Nutrition is influenced by season and may assert its effect on immune response in more complex ways that defy the singling out of one isolated factor 20.
The peak in TB notifications in April suggests that the combination of increased transmission in the winter months and the subsequent incubation period, reduced accessibility to services during winter months, peaking of workload in early spring resulting in a deferral of attending medical services, perhaps coupled with reduced resistance against progression to disease may be co-responsible for the observed seasonal pattern. While all these (and perhaps other) factors may be contributors, increased indoor transmission during the coldest season suggests itself to be the primary triggering event.
It is conducive to assume an influence of the ambient temperature on behaviour (indoors versus outdoors activities) and on nutrition. It remains to be demonstrated whether both play a role in Mongolia. Both lead to an increased frequency of primary and exogenous reactivation disease, and the latter to an increased risk of endogenous reactivation. TB among children could help determine the importance of TB resulting from recent infection, but is hampered by the uncertainty surrounding its diagnosis. In South Africa, cases of culture-confirmed TB in children and tuberculous meningitis peaked in the spring and were lowest in autumn and winter 21, which was interpreted as being suggestive of increased transmission during the preceding winter months spent indoors in crowded settings.
To what extent accessibility to services matters remains unclear. The similarity in the pattern observed in urban Ulaanbaatar and the predominantly rural rest of the country would suggest such an influence to be minor. Furthermore, case notifications reach the trough as early as September when temperatures are still around 10°C degrees above zero. In India, seasonality in case notifications was not attributed to health-seeking behaviour 22.
The seasonal pattern in Mongolia remains a remarkably pronounced phenomenon that currently defies a simple explanation. Beyond any doubt, these amplitudes have an immediate and profound effect on TB management. Requirements in supplies cannot be based on experience from the preceding quarters 7, but must rather be based on reports from the same quarter in the previous year. While the issue of supplies in diagnostic material and medications can thus be addressed, adaptation of needs in hospital beds and personnel is much more difficult to tackle.
If increased transmission in winter months indeed results in the surge of sputum smear-positive cases in April, it is likely that these cases represent only a percentage of the newly emerging cases, and thorough contact examinations among persons living under the same roof, with appropriate action, would need to be given much more emphasis than is currently the case.
Statement of interest
None declared.
Acknowledgments
The authors thank Ts. Tserenbaljid, Tuberculosis Dept, National Center for Communicable Diseases, Ulaanbaatar, Mongolia, for her valuable support in data management.
- Received March 1, 2009.
- Accepted April 6, 2009.
- © ERS Journals Ltd
References










