
Abstract
Purpose
To evaluate the impact of preoperative diagnosis in obtaining negative lumpectomy margins.
Materials and Methods
Five hundred and thirty five patients who underwent breast conserving therapy for stage I/II cancer from 1971 to 1996 were included in this IRB-approved retrospective analysis. Three hundred and ninety five patients had a defined inked margin status after initial excision. The following factors were evaluated for correlation with margins at initial excision: age (< or >45), grade (3/1 or 2), family history (present/absent), histology (lobular/other), estrogen receptor (ER) status, presence of extensive intraductal carcinoma (EIC), presence of lymphovascular invasion (LVI), and biopsy type (excisional/preoperative).
Results
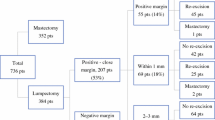
Biopsy type (P < 0.0001), EIC (P = 0.002), ER status (P = 0.02), lobular histology (P = 0.02) and age (P = 0.02) were significantly correlated with initial margin status among the entire group. For patients who underwent preoperative diagnostic biopsy, 52% (35/67) had negative initial margins as compared to 29% (94/328) for excisional biopsy. Among patients who underwent preoperative biopsy, only lobular histology (P = 0.04) and LVI (P = 0.04) were related to initial margin status. The rate of re-excision was 34% for patients diagnosed preoperatively versus 61% with excisional biopsy (P < 0.0001). The percentage of patients with negative final margin status was similar with either core/needle or excisional biopsy (79 and 78%, respectively).
Conclusions
Preoperative diagnosis is the most significant predictor of initial margin status in patients undergoing breast conservation. Patients with lobular histology may require improved preoperative and/or intraoperative assessment to increase the rate of negative margins at initial excision.
Similar content being viewed by others


References
Crowe JP, Rim A, Patrick R, et al. A prospective review of the decline of excisional biopsy. Am J Surg 2002; 184:353–5.
Jackman RJ, Marzoni FA. Stereotactic histologic biopsy with patients prone: technical feasibility in 98% of mammographically detected lesions. AJR 2003; 180:785–94.
Caines JS, Schaller GH, Iles SE, et al. Ten years of breast screening in the Nova Scotia breast screening program, 1991–2001. JACR 2005; 56:82–93.
Fahrbach K, Sledge I, Cella C,Linz H, Ross SD. A comparison of the accuracy of two minimally invasive breast biopsy methods: a systematic literature review and meta-analysis. Arch Gynecol Obstet 2006; 274:63–73.
Verkooijen HM, Core biopsy after radiologic localization (COBRA) study group. Diagnostic accuracy of stereotactic large-core needle biopsy for nonpalpable breast disease: results of a multicenter prospective study with 95% surgical confirmation. Int J Cancer 2002; 99:853–99.
Jackman RJ, Nowels KW, Rodriguez-Soto J, Marzoni FA, Finkelstein SI, Shepard MJ. Stereotactic, automated large-core needle biopsy of nonpalpable breast lesions: false-negative and histologic underestimation rates after long-term follow up. Radiology 1999; 210:799–805.
Yim JH, Barton P, Weber B, et al. Mammographically detected breast cancer. Benefits of stereotactic core versus wire localization biopsy. Ann Surg 1996; 223:688–700.
White RR, Halperin TJ, Olson JA, Soo MS, Bentley RC, Seigler HF. Impact of core-needle breast biopsy on the surgical management of mammographic abnormalities. Ann Surg 2001; 233:769–77.
Smitt MC, Nowels K, Zdeblick M, et al. The importance of the lumpectomy surgical margin status in long term results of breast conservation. Cancer 1995; 77:259–67.
Verkooijen HM, Rinkes IH, Peeters PH, et al. Impact of stereotactic large-core needle biopsy on diagnosis and surgical treatment of non-palpable breast cancer. EJSO 2001; 27:244–49.
Morrow M, Venta L, Stinson T, Bennett C. Prospective comparison of stereotactic core biopsy and surgical excision as diagnostic procedures for breast cancer patients. Ann Surg 2001; 233:537–41.
Fahy BN, Bold RJ, Schneider PD, Khatri V, Goodnight JE. Cost-benefit analysis of biopsy methods for suspicious mammographic lesions. Arch Surg 2001; 136:990–5.
Hemmer PH, Klaase JM, Mastboom WJ, Gerritsen JJ, Mulder HJ, Volker ED. The continued utility of needle localized biopsy for non-palpable breast lesions. EJSO 2004; 30:10–4.
Groenewoud JH, Pijnappel RM, van den Akker-van Marle ME, et al. Cost-effectiveness of stereotactic large core needle biopsy for nonpalpable breast lesions compared to open breast biopsy. Br J Cancer 2004; 90:383–92.
Chen AM, Haffty BG, Lee CH. Local recurrence of breast cancer after breast conservation therapy in patients examined by means of stereotactic core-needle biopsy. Radiology 2002; 225:707–12.
Cangiarella J, Gross J, Symmans WF, et al. The incidence of positive margins with breast conserving therapy following mammotome biopsy for microcalcification. J Surg Oncol 2000; 74:263–6.
Dillon MF, Hill AD, Quinn CM, McDermott EW, O’Higgins N. A pathologic assessment of adequate margin status in breast-conserving therapy. Ann Surg Oncol 2006; 13:333–9.
Fleming FJ, Hill AD, McDermott EW, O’Doherty A, O’Higgins N, Quinn CM. Intraoperative margin assessment and re-excision rate in breast-conserving surgery. EJSO 2004; 30:233–7.
Dillon MF, Hill AD, Fleming FJ, et al. Identifying patients at risk of compromised margins following breast conservation for lobular carcinoma. Am J Surg 2006; 191:201–5.
Moore MM, Borossa G, Imbrie JZ, et al. Association of infiltrating lobular carcinoma with positive surgical margins after breast-conservation therapy. Ann Surg 2000; 231:877–82.
Takehara M, Tamura M, Kameda H, Ogita M. Examination of breast conserving therapy in lobular carcinoma. Breast Cancer 2004; 11:69–72.
Jimenez RE, Bongers S, Bouwman D, Segel M, Visscher DW. Clinicopathologic significance of ductal carcinoma in situ in breast core needle biopsies with invasive cancer. Am J Surg Pathol 2000; 24:123–8.
Dzierzanowski M, Melville K, Barnes PJ, Macintosh RF, Caines JS, Porter GA. Ductal carcinoma in situ in core biopsies containing invasive breast cancer: correlation with extensive intraductal component and lumpectomy margins. J Surg Oncol 2005; 90:71–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Smitt, M.C., Horst, K. Association of Clinical and Pathologic Variables with Lumpectomy Surgical Margin Status after Preoperative Diagnosis or Excisional Biopsy of Invasive Breast Cancer. Ann Surg Oncol 14, 1040–1044 (2007). https://doi.org/10.1245/s10434-006-9308-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-006-9308-1