
Abstract
Background
Whole-body 131I scintigraphy (WBS) and serial thyroglobulin measurement (Tg) are standard methods for detecting thyroid cancer recurrence after total/near total thyroidectomy and 131I ablation. Some patients develop elevated Tg (Tg-positive) or there is clinical suspicion of recurrence, but WBS are negative (WBS-negative). This may reflect non-iodine-avid recurrence or metastasis. In 2002, the Centers for Medicare and Medicaid Services (CMS) approved positron emission tomography with [18F]fluorodeoxyglucose (FDG-PET) for Tg-positive/WBS-negative patients with follicular-cell-origin thyroid cancer. Limited data are available regarding the performance of combined FDG-PET/computed tomography (FDG-PET/CT) for detecting recurrent thyroid cancer in WBS-neg patients.
Methods
This retrospective review of prospectively collected data analyzed 65 patients who had FDG-PET/CT for suspected thyroid cancer recurrence (April 1998–August 2006). Patients were WBS-negative but were suspected to have recurrence based on Tg levels or clinical grounds. Suspected FDG-PET/CT abnormalities were reported as benign or malignant. Lesions were ultimately declared benign or malignant by surgical pathology or clinical outcome (disease progression).
Results
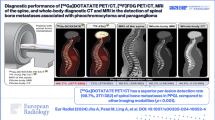
Of 65 patients who underwent FDG-PET/CT, 47 had positive FDG-PET/CT. Of the positive FDG-PET/CT, 43 studies were true positives, with 21 (49%) confirmed pathologically by surgical resection. The four false positives (3/4 confirmed pathologically) included an infundibular cyst, an inflamed supraclavicular cyst, pneumonitis, and degenerative disc disease. Of the 18 FDG-PET/CT studies that were negative, 17 were true negatives and one was a false negative (metastatic papillary carcinoma). Thus, FDG-PET/CT demonstrated a patient-based sensitivity of 98%, specificity of 81%, positive predictive value of 91%, and negative predictive value of 94%.
Conclusions
FDG-PET/CT is useful for detecting thyroid cancer recurrence in WBS-negative patients, and can assist decision making.

Similar content being viewed by others

References
Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin 2007;57:43–66
Roelants V, Nayer PD, Bouckaert A, Beckers C. The predictive value of serum thyroglobulin in the follow-up of differentiated thyroid cancer. Eur J Nucl Med 1997;24:722–7
Grigsby PW, Baglan K, Siegel BA. Surveillance of patients to detect recurrent thyroid carcinoma. Cancer 1999;85:945–51
Grigsby PW, Siegel BA, Bekker S, Clutter WE, Moley JF. Preparation of patients with thyroid cancer for 131I scintigraphy or therapy by 1-3 weeks of thyroxine discontinuation. J Nucl Med 2004;45:567–70
Ashcraft MW, Van Herle AJ. The comparative value of serum thyroglobulin measurements and iodine 131 total body scans in the follow-up study of patients with treated differentiated thyroid cancer. Am J Med 1981;71:806–14
Galligan JP, Winship J, van Doorn T, Mortimer RH. A comparison of serum thyroglobulin measurements and whole body 131I scanning in the management of treated differentiated thyroid carcinoma. Aust NZ J Med 1982;12:248–54
Pacini F, Agate L, Elisei R, et al. Outcome of differentiated thyroid cancer with detectable serum Tg and negative diagnostic 131I whole body scan: comparison of patients treated with high 131I activities versus untreated patients. J Clin Endocrinol Metab 2001;86:4092–7
Schlumberger M, Arcangioli O, Piekarski JD, Tubiana M, Parmentier C. Detection and treatment of lung metastases of differentiated thyroid carcinoma in patients with normal chest x-rays. J Nucl Med 1988;29:1790–4
Pineda JD, Lee T, Ain K, Reynolds JC, Robbins J. Iodine-131 therapy for thyroid cancer patients with elevated thyroglobulin and negative diagnostic scan. J Clin Endocrinol Metab 1995;80:1488–92
Leboulleux S, Schroeder PR, Schlumberger M, Ladenson PW. The role of PET in follow-up of patients treated for differentiated epithelial thyroid cancers. Nat Clin Pract Endocrinol Metab 2007;3:112–21
Dietlein M, Scheidhauer K, Voth E, Theissen P, Schicha H. Fluorine-18 fluorodeoxyglucose positron emission tomography and iodine-131 whole-body scintigraphy in the follow-up of differentiated thyroid cancer. Eur J Nucl Med 1997;24:1342–8
Conti PS, Durski JM, Bacqai F, Grafton ST, Singer PA. Imaging of locally recurrent and metastatic thyroid cancer with positron emission tomography. Thyroid 1999;9:797–804
Grunwald F, Kalicke T, Feine U, et al. Fluorine-18 fluorodeoxyglucose positron emission tomography in thyroid cancer: results of a multicentre study. Eur J Nucl Med 1999;26:1547–52
Wang W, Macapinlac H, Larson SM, et al. [18F]-2-fluoro-2-deoxy-D-glucose positron emission tomography localizes residual thyroid cancer in patients with negative diagnostic (131)I whole body scans and elevated serum thyroglobulin levels. J Clin Endocrinol Metab 1999;84:2291–302
Frilling A, Tecklenborg K, Gorges R, Weber F, Clausen M, Broelsch EC. Preoperative value of 18F fluorodeoxyglucose positron emission tomography in patients with radioiodine-negative recurrent well-differentiated thyroid carcinoma. Ann Surg 2001;234:804–11
Helal BO, Merlet P, Toubert ME, et al. Clinical impact of (18)F-FDG PET in thyroid carcinoma patients with elevated thyroglobulin levels and negative (131)I scanning results after therapy. J Nucl Med 2001;42:1464–9
Schluter B, Bohuslavizki KH, Beyer W, Plotkin M, Buchert R, Clausen M. Impact of FDG PET on patients with differentiated thyroid cancer who present with elevated thyroglobulin and negative 131I scan. J Nucl Med 2001;42:71–6
Giammarile F, Hafdi Z, Bournaud C, et al. Is [18F]-2-fluoro-2-deoxy-d-glucose (FDG) scintigraphy with non-dedicated positron emission tomography useful in the diagnostic management of suspected metastatic thyroid carcinoma in patients with no detectable radioiodine uptake? Eur J Endocrinol 2003;149:293–300
Goshen E, Cohen O, Rotenberg G, Oksman Y, Karasik A, Zwas ST. The clinical impact of 18F-FDG γPET in patients with recurrent well differentiated thyroid carcinoma. Nucl Med Commun 2003;24:959–61
Gabriel M, Froehlich F, Decristoforo C, et al. 99mTc-EDDA/HYNIC-TOC and (18)F-FDG in thyroid cancer patients with negative (131)I whole-body scans. Eur J Nucl Med Mol Imaging 2004;31:330–41
Nahas Z, Goldenberg D, Fakhry C, et al. The role of positron emission tomography/computed tomography in the management of recurrent papillary thyroid carcinoma. Laryngoscope 2005;115:237–43
Palmedo H, Bucerius J, Joe A, et al. Integrated PET/CT in differentiated thyroid cancer: diagnostic accuracy and impact on patient management. J Nucl Med 2006;47:616–24
Alzahrani AS, Mohamed GE, Al Rifai A, et al. Role of [18F]fluorodeoxyglucose positron emission tomography in follow-up of differentiated thyroid cancer. Endocr Pract 2006;12:152–8
Pryma DA, Schoder H, Gonen M, Robbins RJ, Larson SM, Yeung HW. Diagnostic accuracy and prognostic value of 18F-FDG PET in Hurthle cell thyroid cancer patients. J Nucl Med 2006;47:1260–6
Zimmer LA, McCook B, Meltzer C, et al. Combined positron emission tomography/computed tomography imaging of recurrent thyroid cancer. Otolaryngol Head Neck Surg 2003;128:178–84
Shammas A, Degirmenci B, Mountz JM, et al. 18F-FDG PET/CT in patients with suspected recurrent or metastatic well-differentiated thyroid cancer. J Nucl Med 2007;48:221–6
Jabour BA, Choi Y, Hoh CK, et al. Extracranial head and neck: PET imaging with 2-[F-18]fluoro-2-deoxy-D-glucose and MR imaging correlation. Radiology 1993;186:27–35
Nakamoto Y, Tatsumi M, Hammoud D, Cohade C, Osman MM, Wahl RL. Normal FDG distribution patterns in the head and neck: PET/CT evaluation. Radiology 2005;234:879–85
Heller MT, Meltzer CC, Fukui MB, et al. Superphysiologic FDG uptake in the non-paralyzed vocal cord. Resolution of a false-positive PET result with combined PET–CT imaging. Clin Positron Imaging 2000;3:207–11
Lee M, Ramaswamy MR, Lilien DL, Nathan CO. Unilateral vocal cord paralysis causes contralateral false-positive positron emission tomography scans of the larynx. Ann Otol Rhinol Laryngol 2005;114:202–6
Gross ND, Weissman JL, Talbot JM, Andersen PE, Wax MK, Cohen JI. MRI detection of cervical metastasis from differentiated thyroid carcinoma. Laryngoscope 2001;111:1905–9
Torlontano M, Attard M, Crocetti U, et al. Follow-up of low risk patients with papillary thyroid cancer: role of neck ultrasonography in detecting lymph node metastases. J Clin Endocrinol Metab 2004;89:3402–7
Medicare Coverage Database. Centers for Medicare & Medicaid Services, Baltimore. www.cms.hhs.gov/mcd/viewtechassess.asp?where=search&tid=7&basket=ta:7:Systematic+Review+Of+Positron+Emission+Tomography+For+Follow%2DUp+Of+Treated+Thyroid+Cancer (2007). Accessed on 5 June 2007
Ackowledgments
Dr. Hall was supported by the Center for Health Policy, under the auspices of Dr. William Peck, Washington University in St. Louis, St. Louis, MO. The authors declare no conflicts of interest.
Presented at Society of Surgical Oncology (SSO) 60th Annual Cancer Symposium, Washington D.C., March 16, 2007 as an oral presentation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Finkelstein, S.E., Grigsby, P.W., Siegel, B.A. et al. Combined [18F]Fluorodeoxyglucose Positron Emission Tomography and Computed Tomography (FDG-PET/CT) for Detection of Recurrent, 131I-Negative Thyroid Cancer. Ann Surg Oncol 15, 286–292 (2008). https://doi.org/10.1245/s10434-007-9611-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-007-9611-5